

Abstract
Telemedicine is exchange of medical data by electronic telecommunications technology that allows a patient's medical problems evaluated and monitored by a remotely located physician. Over the years, telemedicine and telescreening have become important components in health care, in both disease detection and treatment. Highly visual and image intensive ophthalmology is uniquely suited for telemedicine. Because of rising disease burden coupled with high opportunity cost in detection, diabetic retinopathy is an ideal ophthalmic disease for telescreening and decision-making. It fits to Wilson and Jungner's all 10 criteria of screening for chronic diseases and the American Telehealth Association's 4 screening categories.
Keywords: Diabetic Retinopathy, Screening, Telemedicine
INTRODUCTION
Diabetes mellitus (DM) is a global epidemic.1 An estimated 3.4 million people died in 2004 from consequences of high fasting blood sugar.2 More than 80% of diabetes deaths occur in low- and middle-income countries.3 The World Health Organization (WHO) projects that diabetes will be the 7th leading cause of death in 2030.4 It is estimated that 439 million people are likely to have DM by year 2030 in the world and that this increase is disproportionately more in developing countries (69% in developing countries vs. 20% in developed countries with 2010 as baseline).5 This will result in a heavy burden on the health care system because of several DM related complications.
Diabetic retinopathy (DR), the leading cause of visual disability in diabetics, is an important complication of DM. The reported prevalence of DR in India ranges from 17.6% to 28.2%.6,7,8,9 With this prevalence, the number of people with DM is expected to increase to 79.4 million and patients with DR would increase to 22.4 million in another two decades.5 The potential economic and social burden of DM and DR demands for a definite need for an effective screening strategy, accurate case detection and treatment effective for both DM and DR. Globally, there is an increase in vision-threatening retinopathy.10
Over the past decade, there have been rapid strides in progress in the fields of telecommunication and medical imaging. These have opened newer avenues to creating efficient screening strategy for DR. Newer techniques like stereoscopic imaging, nonmydriatic camera and mobile phone based fundus camera show comparable sensitivity and specificity in diagnosing DR.11,12 India ranks third in the world in number of Internet users by volume. Additionally, 70% has access to mobile phones, and 39% of them live in rural areas. Teledensity has increased from merely 12.1% to 73.3%, a growth of 600%, during the past 5 years.13 This makes screening of DR using imaging and teleophthalmology a distinct possibility that can revolutionize the health care system.
DOES DIABETIC RETINOPATHY FIT INTO SCREENING CRITERIA?
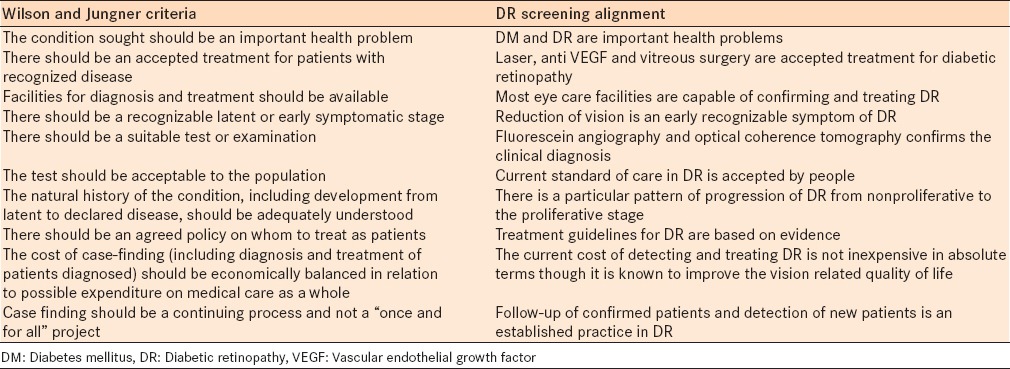
Diabetic retinopathy is a perfect situation for screening. Wilson and Jungner had defined 10 criteria for screening of chronic disease in 1968.14 DR screening fits into this criterion [Table 1].
Table 1.
Wilson and Jungner screening criteria and DR screening alignment
DIABETIC RETINOPATHY SCREENING CRITERIA
One of the main motivations for screening for DR is the established efficacy of laser photocoagulation in preventing visual loss. Two large randomized clinical trials, the DR study, and the early treatment DR study, have provided the strongest support for therapeutic benefit of photocoagulation.15,16 This is further augmented from the current evidence of benefit from anti VEGF therapy in a few of randomized trials.17,18,19 Since some patients with vision-threatening pathologies may not have symptoms, ongoing evaluation for retinopathy is a valuable and required strategy.
The American Diabetes Association recommends retinopathy screening with yearly retinal examination beginning at the time of diagnosis of diabetes for all patients age 30 years and older.20 Annual examinations are recommended for patients under age 30 years beginning within 3–5 years after diagnosis of diabetes. The classical tools used in DR screening include direct ophthalmoscopy, indirect ophthalmoscopy, slit lamp biomicroscopy and fundus photography. These are either optometrist led (direct ophthalmoscopy, fundus photography) or ophthalmologist led (direct and indirect ophthalmoscopy, slit lamp biomicroscopy and fundus photography).
WHAT IS TELEMEDICINE IN DIABETIC RETINOPATHY CARE?
Telemedicine is exchange of medical data by electronic telecommunications technology that allows a patient's medical problems evaluated and monitored by a remotely located physician.21 Application of telemedicine for screening of a disease is called telescreening. Ophthalmology being highly visual and image intensive, is uniquely suited for telemedicine and telescreening.
Normally, diabetics do not visit an ophthalmologist unless they have visual defects. The fundus images can be captured at the physician's or diabetologists facility at the time of a regular diabetic check-up. This kind of opportunistic screening helps in improved screening of these patients. The fundus pictures obtained in a nonmydriatic digital retinal camera are then transmitted through internet, to a reading and grading center where a retinal expert or a trained grader reads them remotely.12 The images are read, a report regarding the status of the retinopathy is generated and the follow-up suggestions are made by the ophthalmologist at a remote location; this report is returned by internet to the patient's location from where the images were taken originally. In areas of scarce medical care, a mobile van with communication capabilities and fundus camera helps. The diabetic patients are pooled in one area, and their fundus pictures are captured and sent to a centralized reading center. The other sequences are similar.
In addition to technical similarity, teleophthalmology in DR care is both efficient and cost-effective. The efficacy of digital photography vis-à-vis the traditional film-based photography and single-field fundus photo vis-à-vis the traditional seven-field fundus photo are recently reported by the American Academy of Ophthalmology.22 We have reported that nonmydriatic fundus photography compared to indirect ophthalmoscopy was 62.5% (95% confidence interval [CI]: 24–91) sensitive and 98.7% (95% CI: 93–99) sensitive;23 we have also reported that telescreening is as good as ophthalmologist led screening for detection of DR.24 Rudnisky et al. have reported good agreement between high-resolution stereoscopic digital fundus photography and contact lens biomicroscopy25 At the same time, despite lack of face-to-face contact, patient satisfaction has remained unchanged in telescreening.26,27,28,29,30,31 It is also less expensive in places with higher patient workload32 and is convenient as it saves the opportunity costs connected with DR screening such as time, travel, and loss of income.33 Rachapelle et al.34 also reported that using the WHO threshold of cost-effectiveness, rural teleophthalmology is cost-effective compared to no screening as long it is done at interval longer than 1-year.
GUIDELINES FOR DIABETIC RETINOPATHY SCREENING PROGRAM
The American Telemedicine Association (ATA) and Ocular Telehealth Special Interest Group have established the guidelines for DR telescreening in 2004.35 They recommend that equipment used in telehealth system must conform to the local requirements and that the technology should adhere to standards of Digital Imaging and Communication in Medicines (DICOM).
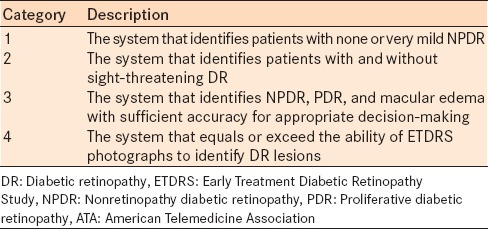
The ATA recognizes four categories of telescreening programs [Table 2]:
Table 2.
ATA telescreening categories
While fundus photo taken in nonmydriatic fundus camera is often used in telescreening, mydraisis usually reduces the proportion of ungradable photographs.36 One could consider mydrasis based on the visual acuity (<20/40) and age (>59 years)37 or in case of unsatisfactory nonmydiatric fundus camera photograph.38
CURRENT STATUS
The setting
Currently, the use of telescreening for DR is used in two settings: (a) Screening by nonphysician/nonophthalmologist. This is usually by an optician/optometrist using a fundus camera, and the diagnosis is given from a remote location; (b) Screening retinopathy by physician/nonophthalmologist. This seems to be an ideal situation as physicians are the first contact for a person with DM.
The screening tools
These include a wide variety of fundus cameras-traditional fundus camera, miniature tabletop fundus camera integrated adaptor-detector based handheld ophthalmic cameras, and smartphone based ophthalmic cameras. Of these, the smartphone based cameras are more cost-effective though; but they need mydriasis.
The image transmission
Majority of telemedicine models today use the internet to transmit images.33,39 Satellite transmission is a more preferred option in rural areas and mobile clinics because of less optimal infrastructure. The images and reports are transmitted digitally via electronic picture archiving and communication systems (PACS). A PACS consists of four components: The imaging instrumentation, a secured network for transmission of patient information, workstations for interpreting and reviewing images, and archives for the storage and retrieval of images and reports. The universal format for PACS image storage and transfer is DICOM. To minimize errors, data communications should be compliant with DICOM standards.
The reporting
This includes grading of image quality, presence or absence of retinopathy, referable/nonreferable retinopathy and the grading severity of the disease.
The current status of telescreening in DR is shown in Figure 1.
Figure 1.

Current status of telescreening in diabetic retinopathy
FUTURE DIRECTIONS
Recent advances in better and faster telecommunication technology including “cloud” storage, miniaturization of diagnostic equipment including digital cameras, and automation of retinal image analysis, offer excellent opportunities to expand telescreening services to more remote areas. In coming years, there would be a shift from telephone landlines to wireless, and from manual to automatic detection of retinal lesions that will enhance the teleophthalmology capabilities both in value and volume. In all probability, automatic detection of retinal lesion images will play a major role in screening and management of DR in future.40
Over the years, telemedicine and screening have become important components in health care, in both disease detection and treatment. The first step in telemedicine in management of DR is screening for patients with retinopathy. The emerging screening criteria proposed over the past 40 plus years ago by Wilson and Jungner should respond to a recognized need.41 They include the following: The objectives of screening should be defined at the outset; there should be a defined target population; there should be scientific evidence of screening program effectiveness; the program should integrate education, clinical services, and management; there should be quality assurance, with mechanisms to minimize potential risks of screening; the program should ensure informed choice, confidentiality and respect for autonomy; the program should promote equity and access to screening for the entire target population; program evaluation should be planned from the outset; finally the overall benefits of screening should outweigh the harm.
Footnotes
Source of Support: Hyderabad Eye Research Foundation, Hyderabad; Medical Research Foundation, Chennai; Aravind Research Foundation, Madurai.
Conflict of Interest: None declared.
REFERENCES
- 1.Danaei G, Finucane MM, Lu Y, Singh GM, Cowan MJ, Paciorek CJ, et al. National, regional, and global trends in fasting plasma glucose and diabetes prevalence since 1980: Systematic analysis of health examination surveys and epidemiological studies with 370 country-years and 2·7 million participants. Lancet. 2011;378:31–40. doi: 10.1016/S0140-6736(11)60679-X. [DOI] [PubMed] [Google Scholar]
- 2.Geneva: World Health Organization; 2009. World Health Organization. Global Health Risks. Mortality and Burden of Disease Attributable to Selected Major Risks. [Google Scholar]
- 3.Mathers CD, Loncar D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med. 2006;3:e442. doi: 10.1371/journal.pmed.0030442. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Geneva: World Health Organization; 2011. World Health Organization. Global Status Report on Noncommunicable Diseases 2010. [Google Scholar]
- 5.Shaw JE, Sicree RA, Zimmet PZ. Global estimates of the prevalence of diabetes for 2010 and 2030. Diabetes Res Clin Pract. 2010;87:4–14. doi: 10.1016/j.diabres.2009.10.007. [DOI] [PubMed] [Google Scholar]
- 6.Dandona L, Dandona R, Naduvilath TJ, McCarty CA, Rao GN. Population based assessment of diabetic retinopathy in an urban population in southern India. Br J Ophthalmol. 1999;83:937–40. doi: 10.1136/bjo.83.8.937. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Rema M, Premkumar S, Anitha B, Deepa R, Pradeepa R, Mohan V. Prevalence of diabetic retinopathy in urban India: The Chennai Urban Rural Epidemiology Study (CURES) eye study, I. Invest Ophthalmol Vis Sci. 2005;46:2328–33. doi: 10.1167/iovs.05-0019. [DOI] [PubMed] [Google Scholar]
- 8.Narendran V, John RK, Raghuram A, Ravindran RD, Nirmalan PK, Thulasiraj RD. Diabetic retinopathy among self reported diabetics in southern India: A population based assessment. Br J Ophthalmol. 2002;86:1014–8. doi: 10.1136/bjo.86.9.1014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Agarwal RP, Ranku M, Beniwal R, Gothwal SR, Jain GC, Kochar DK, et al. Prevalence of diabetic retinopathy in type 2 diabetes in relation to risk factors: Hospital based study. Int J Diabetes Dev Ctries. 2003;23:16–9. [Google Scholar]
- 10.Yau JW, Rogers SL, Kawasaki R, Lamoureux EL, Kowalski JW, Bek T, et al. Global prevalence and major risk factors of diabetic retinopathy. Diabetes Care. 2012;35:556–64. doi: 10.2337/dc11-1909. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Tennant MT, Greve MD, Rudnisky CJ, Hillson TR, Hinz BJ. Identification of diabetic retinopathy by stereoscopic digital imaging via teleophthalmology: A comparison to slide film. Can J Ophthalmol. 2001;36:187–96. doi: 10.1016/s0008-4182(01)80039-9. [DOI] [PubMed] [Google Scholar]
- 12.Liesenfeld B, Kohner E, Piehlmeier W, Kluthe S, Aldington S, Porta M, et al. A telemedical approach to the screening of diabetic retinopathy: Digital fundus photography. Diabetes Care. 2000;23:345–8. doi: 10.2337/diacare.23.3.345. [DOI] [PubMed] [Google Scholar]
- 13.Telecom Regulatory Authority of India. [Last accessed on 2014 Dec 24]. Available from: http://www.trai.gov.in/WriteReadData/WhatsNew/Documents/IndicatorReports-01082013. pdfhttp://www.trai.gov.in/WriteReadData/WhatsNew/Documents/Indicator%20Reports%20-01082013.pdf .
- 14.Wilson JM, Jungner G. Geneva: WHO; 1968. Principles and Practice of Screening for Disease. 86/4/07. [Google Scholar]
- 15.Photocoagulation for diabetic macular edema. Early Treatment Diabetic Retinopathy Study report number 1. Early Treatment Diabetic Retinopathy Study research group. Arch Ophthalmol. 1985;103:1796–806. [PubMed] [Google Scholar]
- 16.Treatment techniques and clinical guidelines for photocoagulation of diabetic macular edema. Early Treatment Diabetic Retinopathy Study Report Number 2. Early Treatment Diabetic Retinopathy Study Research Group. Ophthalmology. 1987;94:761–74. doi: 10.1016/s0161-6420(87)33527-4. [DOI] [PubMed] [Google Scholar]
- 17.Massin P, Bandello F, Garweg JG, Hansen LL, Harding SP, Larsen M, et al. Safety and efficacy of ranibizumab in diabetic macular edema (RESOLVE Study): A 12-month, randomized, controlled, double-masked, multicenter phase II study. Diabetes Care. 2010;33:2399–405. doi: 10.2337/dc10-0493. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Elman MJ, Ayala A, Bressler NM, Browning D, Flaxel CJ, Glassman AR, et al. Intravitreal Ranibizumab for Diabetic Macular Edema with Prompt versus Deferred Laser Treatment: 5-Year Randomized Trial Results. Ophthalmology. 2015;122:375–81. doi: 10.1016/j.ophtha.2014.08.047. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Korobelnik JF, Do DV, Schmidt-Erfurth U, Boyer DS, Holz FG, Heier JS, et al. Intravitreal aflibercept for diabetic macular edema. Ophthalmology. 2014;121:2247–54. doi: 10.1016/j.ophtha.2014.05.006. [DOI] [PubMed] [Google Scholar]
- 20.American Diabetes Association. Position statement: Diabetic retinopathy. Clinical Practice Guidelines 2001. Diabetes Care. 2001;24(Supp 1):S73–6. [Google Scholar]
- 21.Zimmer-Galler IE, Zeimer R. Telemedicine in diabetic retinopathy screening. Int Ophthalmol Clin. 2009;49:75–86. doi: 10.1097/IIO.0b013e31819fd60f. [DOI] [PubMed] [Google Scholar]
- 22.Williams GA, Scott IU, Haller JA, Maguire AM, Marcus D, McDonald HR. Single-field fundus photography for diabetic retinopathy screening: A report by the American Academy of Ophthalmology. Ophthalmology. 2004;111:1055–62. doi: 10.1016/j.ophtha.2004.02.004. [DOI] [PubMed] [Google Scholar]
- 23.Raman R, Rani PK, Sharma T. The sensitivity and specificity of nonmydriatic digital stereoscopic retinal imaging in detecting diabetic retinopathy: Response to Ahmed et al. Diabetes Care. 2007;30:e47. doi: 10.2337/dc07-0052. [DOI] [PubMed] [Google Scholar]
- 24.Raman R, Bhojwani DN, Sharma T. How accurate is the diagnosis of diabetic retinopathy on telescreening? The Indian scenario. Rural Remote Health. 2014;14:2809. [PubMed] [Google Scholar]
- 25.Rudnisky CJ, Hinz BJ, Tennant MT, de Leon AR, Greve MD. High-resolution stereoscopic digital fundus photography versus contact lens biomicroscopy for the detection of clinically significant macular edema. Ophthalmology. 2002;109:267–74. doi: 10.1016/s0161-6420(01)00933-2. [DOI] [PubMed] [Google Scholar]
- 26.Kumari Rani P, Raman R, Manikandan M, Mahajan S, Paul PG, Sharma T. Patient satisfaction with tele-ophthalmology versus ophthalmologist-based screening in diabetic retinopathy. J Telemed Telecare. 2006;12:159–60. doi: 10.1258/135763306776738639. [DOI] [PubMed] [Google Scholar]
- 27.Kumar S, Yogesan K, Hudson B, Tay-Kearney ML. Internetbased electronics eye care consultations: Patient perspective. In: Yogesan K, Kumar S, Goldschmidth L, Cuadros J, editors. Tele-ophthalmology. Berlin, Germany: Springer Verlag; 2008. pp. 133–8. [Google Scholar]
- 28.Tuulonen A, Ohinmaa T, Alanko HI, Hyytinen P, Juutinen A, Toppinen E. The application of teleophthalmology in examining patients with glaucoma: A pilot study. J Glaucoma. 1999;8:367–73. [PubMed] [Google Scholar]
- 29.Paul PG, Raman R, Rani PK, Deshmukh H, Sharma T. Patient satisfaction levels during teleophthalmology consultation in rural South India. Telemed J E Health. 2006;12:571–8. doi: 10.1089/tmj.2006.12.571. [DOI] [PubMed] [Google Scholar]
- 30.Kurji K, Kiage D, Rudnisky CJ, Damji KF. Improving diabetic retinopathy screening in Africa: Patient satisfaction with teleophthalmology versus ophthalmologist-based screening. Middle East Afr J Ophthalmol. 2013;20:56–60. doi: 10.4103/0974-9233.106388. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Luzio S, Hatcher S, Zahlmann G, Mazik L, Morgan M, Liesenfeld B, et al. Feasibility of using the TOSCA telescreening procedures for diabetic retinopathy. Diabet Med. 2004;21:1121–8. doi: 10.1111/j.1464-5491.2004.01305.x. [DOI] [PubMed] [Google Scholar]
- 32.Bjørvig S, Johansen MA, Fossen K. An economic analysis of screening for diabetic retinopathy. J Telemed Telecare. 2002;8:32–5. doi: 10.1258/1357633021937433. [DOI] [PubMed] [Google Scholar]
- 33.Gomez-Ulla F, Alonso F, Aibar B, Gonzalez F. A comparative cost analysis of digital fundus imaging and direct fundus examination for assessment of diabetic retinopathy. Telemed J E Health. 2008;14:912–8. doi: 10.1089/tmj.2008.0013. [DOI] [PubMed] [Google Scholar]
- 34.Rachapelle S, Legood R, Alavi Y, Lindfield R, Sharma T, Kuper H, et al. The cost-utility of telemedicine to screen for diabetic retinopathy in India. Ophthalmology. 2013;120:566–73. doi: 10.1016/j.ophtha.2012.09.002. [DOI] [PubMed] [Google Scholar]
- 35.Cavallerano J, Lawrence MG, Zimmer-Galler I, Bauman W, Bursell S, Gardner WK, et al. Telehealth practice recommendations for diabetic retinopathy. Telemed J E Health. 2004;10:469–82. doi: 10.1089/tmj.2004.10.469. [DOI] [PubMed] [Google Scholar]
- 36.Murgatroyd H, Ellingford A, Cox A, Binnie M, Ellis JD, MacEwen CJ, et al. Effect of mydriasis and different field strategies on digital image screening of diabetic eye disease. Br J Ophthalmol. 2004;88:920–4. doi: 10.1136/bjo.2003.026385. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Raman R, Rani PK, Mahajan S, Paul P, Gnanamoorthy P, Krishna MS, et al. The tele-screening model for diabeticretinopathy: Evaluating the influence of mydriasis on the gradability of a single-field 45 degrees digital fundus image. Telemed J E Health. 2007;13:597–602. doi: 10.1089/tmj.2006.0084. [DOI] [PubMed] [Google Scholar]
- 38.Murgatroyd H, Cox A, Ellingford A, Ellis JD, Macewen CJ, Leese GP. Can we predict which patients are at risk of having an ungradeable digital image for screening for diabetic retinopathy? Eye (Lond) 2008;22:344–8. doi: 10.1038/sj.eye.6702611. [DOI] [PubMed] [Google Scholar]
- 39.Aiello LM, Bursell SE, Cavallerano J, Gardner WK, Strong J. Joslin Vision Network Validation Study: Pilot image stabilization phase. J Am Optom Assoc. 1998;69:699–710. [PubMed] [Google Scholar]
- 40.Abràmoff MD, Niemeijer M, Suttorp-Schulten MS, Viergever MA, Russell SR, van Ginneken B. Evaluation of a system for automatic detection of diabetic retinopathy from color fundus photographs in a large population of patients with diabetes. Diabetes Care. 2008;31:193–8. doi: 10.2337/dc08-0952. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Andermann A, Blancquaert I, Beauchamp S, Déry V. Revisiting Wilson and Jungner in the genomic age: A review of screening criteria over the past 40 years. Bull World Health Organ. 2008;86:317–9. doi: 10.2471/BLT.07.050112. [DOI] [PMC free article] [PubMed] [Google Scholar]