

Abstract
Warty dyskeratoma is a rare tumor that presents mainly as an isolated papule or nodule on the scalp, face or neck in the adults. Warty dyskeratoma frequently arises as a single lesion with a central keratotic plug on the skin of middle-aged or elderly people. Multiple warty dyskeratomas are very rare cutaneous lesions which are mostly seen on the scalp. We herein report a multiple warty dyskeratoma in a female patient.
Introduction
Helwig, in 1954 first described a solitary lesion and called it as ‘ isolated Darier disease ‘(1). Three years later this disease was more properly called warty dyskeratoma by Szymanski (2) in his review of seven new cases. Warty dyskeratoma (WD) is a rare tumor that presents mainly as an isolated papule or nodule on the scalp, face or neck (3). WD usually presents solely, but grouped verrucous papules on the scalp have been reported (4–6).
In this study, we report a 55-year-old female who had multiple verrucous papules on her scalp and forehead which histologic features were consistent with WD.
Case Report
A 55 - year— old female was admitted to Uludag University Medical Faculty Dermatology Department in 2014 with a 3 to 4 year history of papules on the scalp, nose and forehead. Dermatologic examination revealed numerous, discrete, brownish hairless papules with a smooth surface on parietal scalp, nose and left forehead. Eight papules were excised over the lesional site and the diameter of these papules ranged from 2 to 6 mm. On histologic examination, there were cup-shaped lesions consisted of a large, well-circumscibed epidermal invagination lined mainly at the periphery and at the base by a proliferation of epithelial cells extending into the papillary dermis. All lesions revealed foci of acantholysis with dyskeratosis. Foci with relatively larger epithelial cells showing abundant eosinophilic cytoplasm and a small dark nucleus, probably representing an early stage of dyskeratosis were seen (Fig. 1). By these histopathological features, all lesions were diagnosed as multiple WD.
Fig. 1.
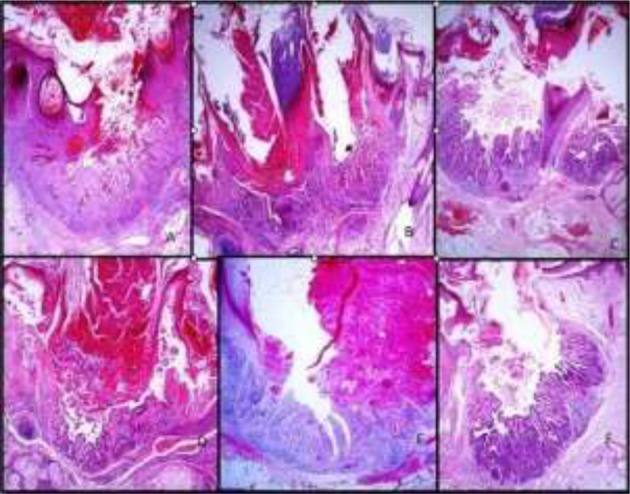
Histopathology of lesions. A,B) A large invagination is connected to the surface (H&E, x100).C,D) Villi at the base of invagination with acantholytic, dyskeratotic cells (H&E, x100). E,F) The villi are covered with a single layer of cells (A) H&E, x100,B) H&E, x200
Discussion
WD is a relatively uncommon benign skin lesion. WD frequently arises as a single lesion with a central keratotic plug on the skin of the head or neck in the adults.
The patient usually states symptoms of pruritus and cheesy drainage from the lesions. Tanay and Mehregan (3) reviewed 112 cases of WD of which were solitary, occuring mainly on sun-exposed sites. The pathogenesis of WD is unknown yet. But ultraviolet radiation, autoimmunity, viral factors, chemical carcinogens, and smoking have been proposed for lesions (7).
Multiple WDs are very rare cutaneous lesions which are mostly seen on scalp (4-6,8). Multiple WDs case have been reported by Azuma (4) distributed over scalp, neck, cheek, and hand in one patient. Also Griffiths et al. (5) presented two female cases with 25 and 15 discrete hyperkeratotic papules and those lesions were established to be WD. Lastly Koç et al. (6) reported a case, which had 15 skin colored verrucous papules on scalp diagnosed as WD. All cases that previously reported usually involved scalp as our case and expect the case which Azuma was reported (4) other all patients were female (Table 1).
Table 1.
The details of the multiple WD patients in the literature
On histologic examination, the center of WD is occupied by a large, cup-shaped invagination connected to the surface by a channed filled with keratinous material (8). Kaddu (8) demonstrated a wider morphologic spectrum incluiding cup-shaped, cystic, and nodular in WD. Differential diagnosis includes Darier’s disease, acantholytic squamous cell carcinoma, and keratoacanthoma. Darier’s disease may be excluded by the lack of typical clinical features. The acantholytic type of squamous cell carcinoma is concerned, several distinguishing histopathologic criteria suggeted architectural configuration of a cyst in WD and lack of atypia and mitotic figures (10). Unlike WD, keratoacanthoma usually lacks prominent areas of acantholytic dyskeratosis.
It is noteworthy that there have been occasional reports of WDs arising on the mucosal surfaces, mainly including the oral mucosa, anatomic sites that normally lack hair follicle (7). All mucosal lesions presented as single nodule. However there was an association between WD and hair follicles in multiple WDs. Consequently, mucosal lesions might represent a different origin rather than multiple skin WDs.
Acknowledgements
The authors declare that there is no conflict of interest.
References
- Helwig EB (1954). Proceedings of the 20th seminar on skin neoplasms and dermatoses. International Congress of Clinical Pathologists, Washington, DC, September11, Published by the American Society of Clinical Pathology [Google Scholar]
- Szymanski FJ (1957). Warty dyskeratoma: a benign cutaneous tumor resembling Darier's disease microscopically. Arch Dermatol, 75: 567–572. [DOI] [PubMed] [Google Scholar]
- Tanay A, Mehregan AH (1969). Warty dyskeratoma. Dermatologica ;138: 155–164. [DOI] [PubMed] [Google Scholar]
- Azuma Y, Matsukawa A (1993). Warty dyskeratoma with multiple lesions. J Dermatol, 20(6): 374–377. [DOI] [PubMed] [Google Scholar]
- Griffiths TW, Hashimoto K, Sharata HH, Ellis CN (1997). Multiple Warty dyskeratomas of the scalp. Clin Exp Dermatol, 22(4): 189–191. [PubMed] [Google Scholar]
- Koç M, Kavala M, Kocatürk E, Mete O, Can B, Zindanci I, Aktaş S (2009). Multıple warty dyskeratomas on the scalp. Dermatol Online J, 15(2): 8. [PubMed] [Google Scholar]
- DiMaio DJ, Cohen PR (1998). Incidental focal acantholyticdyskeratosis. J Am Acad Dermatol, 1998; 38: 243–245. [DOI] [PubMed] [Google Scholar]
- Kaddu S, Dong H, Mayer G, Kerl H, Cerroni L (2002). Warty dyskeratoma – ‘‘follicular dyskeratoma’’: analysis of clinicopathologic features of a distinctive follicular adnexal neoplasm. J Am Acad Dermatol, 47: 423. [DOI] [PubMed] [Google Scholar]
- Ackerman AB, Troy JL, Rosen LB, Jerasutus S, White CR, King DF (1988). Warty dyskeratomavs squamous-cell carcinoma with acantholytic cells. In: Differential diagnosis in dermatopathology II. Philadelphia: Lea & Febiger [Google Scholar]
- Kirkham N (2009). Tumors and cysts of the epidermis. In: Elder DE, editor. Lever's histopathology of the skin. 10th ed. Lippincott Williams and Wilkins: Philadelphia [Google Scholar]