

Abstract
The use of medication in international football has been monitored since the 2002 FIFA World Cup. Team physicians were asked to provide information on prescribed medication 72 h prior to each match for every player. 69% of adult male players reported using medication, with more than half the players using non-steroidal anti-inflammatory drugs (NSAIDs). Up to one-third of all players used NSAIDs prior to every match, regardless of whether they took the field or not. The mean intake of medication was significantly higher during the FIFA Women's World Cup (0.85 vs 0.77 substances per player and per match in men, p<0.001), whereas the use of NSAIDs was similar to that for men. In the Under-20 and Under-17 male competitions, the use of medication was lower as 60% of players used some kind of medication and 43% of the players used NSAIDs during the tournaments. Despite the potential side effects of medication, especially of NSAIDs in the recovery process after a sports activity, there is no evidence of decreasing intake. The reported incidence is alarming, and moreover is most probably underestimated, since self-medication by the players or treatment already prescribed by club physicians is not included in the published reports. Future studies should focus on the daily dosage, time of treatment and especially the medical indication for painkilling agents to better understand the underlying factors.
Keywords: Football, Medicine, Pharmacology, Risk factor, Soccer
Introduction
The FIFA Medical Assessment and Research Centre (F-MARC) was the first medical governing body in international sports to systematically document the use of medication; it has done so since the 1998 FIFA World Cup. For FIFA tournaments, data are collected in connection with doping control after each match. Team physicians are asked to provide information about “any medication taken by the players or administered to them in the 72 hours preceding the match … The team doctor shall also note down, on the basis of the information at his disposal, medications and food supplements taken by the players without medical prescription”.1
Other sports governing bodies such as the IOC and the International Association of Athletics Federations (IAAF) followed suit but only for athletes selected for doping control.2–5
For this review, we present published data from 10 men's, women's and male adolescent FIFA World Cups6–8 (see table 1) and compare them with reports from other sports. This review, and the discussion of overmedication, should be viewed in the context of international campaigns warning against the harms of excessive medication.9
Table 1.
Tournament information
| Tournament | Teams (n) | Players (n) | Matches (n) | Reports (n) | Medications prescribed (n) | Intake of medication (per player, per match) |
|---|---|---|---|---|---|---|
| WC 2014 | 32 | 736 | 64 | 2944 | 2346 | 0.80 |
| WC 2010 | 32 | 736 | 64 | 2944 | 2335 | 0.79 |
| WC 2006 | 32 | 736 | 64 | 2944 | 2052 | 0.70 |
| WC 2002 | 32 | 736 | 64 | 2944 | 2392 | 0.81 |
| W-WC 2007 | 16 | 336 | 32 | 1344 | 1200 | 0.89 |
| W-WC 2003 | 16 | 320 | 32 | 1280 | 1036 | 0.81 |
| U-20 2007 | 24 | 504 | 52 | 2184 | 965 | 0.44 |
| U-20 2005 | 24 | 504 | 52 | 2184 | 1248 | 0.57 |
| U-17 2007 | 24 | 504 | 52 | 2184 | 1036 | 0.47 |
| U-17 2005 | 16 | 320 | 32 | 1280 | 717 | 0.56 |
| Total | 248 | 5432 | 508 | 22 232 | 15 327 | 0.71 |
U, under; W-WC, Women's World Cup.
The 2002, 2006, 2010 and 2014 FIFA World Cups
The mean intake of medication in male professional football is consistent for all World Cups with 0.77 substances per player and per match (see table 1). The most frequently prescribed substance group was non-steroidal anti-inflammatory drugs (NSAIDs; see figure 1), representing 36% of all substances. β-2-Agonists were reported in 44 players (1.2% of all substances, see table 2) during the four tournaments. However, since β-2-agonists are usually taken during the entire season and do not require a therapeutic use exemption anymore, a national team physician might ignore its use in some players. The use of medication over time did not change significantly, neither in the amount nor in its distribution of substance groups.
Figure 1.
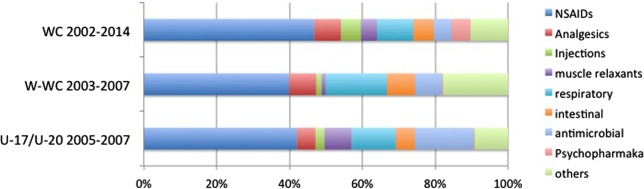
Prescribed medication during the FIFA World Cup. N=9124 for the 2002, 2006, 2010 and 2014 FIFA World Cups; N=2236 for the 2003 and 2007 FIFA Women's World Cup; N=3966 for the 2005 and 2007 FIFA U-17/U-20 World Championships (NSAIDs, non-steroidal anti-inflammatory drugs; U, under; W-WC, Women's World Cup).
Table 2.
Number of players using a substance prior to a match or during the tournament
| 2002–2014 FIFA WC | 2003–2007 FIFA Women's WC | 2005–2007 FIFA U-17/U-20 WC | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Players (n) | Players (n) | Players (n) | ||||||||||
| Per match | During the tournament | Per match | During the tournament | Per match | During the tournament | |||||||
| (N=11 776) | Per cent | (n=2944) | Per cent | (N=2624) | Per cent | n=656 | Per cent | N=7831 | Per cent | n=1832 | Per cent | |
| Any medication | 5179 | 44.0 | 2029 | 68.9 | 1315 | 50.1 | 469 | 71.5 | 2644 | 33.8 | 1097 | 59.9 |
| NSAIDs | 3737 | 31.7 | 1604 | 54.5 | 806 | 30.7 | 334 | 50.9 | 1534 | 19.6 | 793 | 43.3 |
| Injections* | 422 | 3.6 | 234 | 7.9 | 32 | 1.2 | 18 | 2.7 | 89 | 1.1 | 49 | 2.7 |
| Analgesics | 588 | 5.0 | 376 | 12.8 | 143 | 5.4 | 95 | 14.5 | 188 | 2.4 | 137 | 7.5 |
| β-2-Agonists | 142 | 1.2 | 44 | 1.5 | 104 | 4.0 | 28 | 4.3 | 77 | 1.0 | 24 | 1.3 |
| Myorelaxants | 395 | 3.4 | 225 | 7.6 | 25 | 1.0 | 23 | 3.5 | 294 | 3.8 | 20 | 1.1 |
| Any supplement | 2985 | 25.3 | 984 | 33.4 | 880 | 33.5 | 229 | 45.6 | 3104 | 39.6 | 906 | 49.5 |
*Injections of corticosteroids and/or anaesthetics. NSAID, non-steroidal anti-inflammatory drugs; U, under; WC, World Cup.
FIFA Women's World Cup and the Under-17 and Under-18 FIFA World Championships
The reported use of medication during the 2003 and 2007 FIFA Women's World Cup was significantly higher than in the Men's World Cups (0.85 vs 0.77, p≤0.001) and than in adolescent football players participating in Under-17 (U-17) and U-20 tournaments (0.51, p≤0.001; see table 1). Contraceptive agents were not included in the analysis. Whereas the incidence of the use of NSAIDs was similar between adult male and female players, significantly fewer NSAIDs were administered to adolescent players, suggesting increased consumption with age (see table 2).
In 14.9% of female players, oral contraceptive use was reported. This is less than what was reported by Alaranta et al10 for other team sport events (24%), and especially in speed, power and endurance events (40%).
NSAIDs and other analgesics
The NSAIDs category was the one that was most reported in every tournament (see figure 1). In total 54.5% of male players and 50.9% of female players participating in the FIFA World Cup used an NSAID at least once during the tournament; 43.3% adolescent players did so too. Hence, on average, more than seven male and female players per national team were using NSAIDs prior to every match, as were 4.5 players in U-17 and U-20 tournaments (see table 2). Ten per cent of the male and female players were using more than one type of NSAIDs at one time, thus increasing the risk of side effects.
There was no difference in use of medication and NSAIDs, in particular between players participating in the match and substitutes who did not play at all; nor was there a correlation between injuries reported and reported use of medication.7 The most frequently prescribed application form was the oral route (93%). In only 7%, NSAIDs were administered topically,6 although percutaneous application of NSAIDs might be as efficient as oral preparation in the treatment of soft-tissue injuries.11 12
Other analgesics (such as paracetamol (acetaminophen) and metamizol) were rarely used (5.4% of all substances), although they might be as efficient as NSAIDs in treating postexercise pain. Acetylsalicylic acid accounted for 2.8% of all painkilling agents (NSAIDs, analgesics and myorelaxants) in adolescent players as well as in 2.3% of female adults and 1.2% of male adult football players. As its anti-inflammatory and painkilling functions are weak and it carries an increased risk for traumatic haemorrhage, acetylsalicylic acid is not suitable for use in sports medicine.
Injections with local anaesthetics or corticosteroids were mostly intra-articular, followed by intramuscular applications.8 They were performed in almost 8% of all players participating in adult male tournaments, and in about 3% of female adults and male adolescent football players (see table 2). The amount of administration seems to depend highly on the national team physician. Whereas 23 of 32 team physicians did not perform any injections for musculoskeletal symptoms during the 2014 World Cup,8 four players from one national team received peritendinous or intra-articular glucocorticoid injections prior to almost every match. The indication for these injections was not reported. Nevertheless, such repetitive practice during a tournament prior to each match is questionable since the long-term safety of intra-articular application may substantially worsen the injury if play is resumed immediately.13
The medical team (ie, likely team physician) was an important influence as to the use of medication. As reported in the 2002 FIFA World Cup, one country reported using more than one type of NSAID per player per match throughout the tournament. Also, allopurinol—a gout medication reducing uric acid but thought to prevent skeletal and cardiac muscle damage14—was prescribed to 40% of the players from one country during the tournament.
The high use of medication and NSAIDs in particular is not limited to international football. Similar use of medication has been reported during the Sydney Olympics in 2000,2 in top-level track and field athletes,5 triathletes15 and also in collegiate athletes.16 17 An unpublished review18 of articles published between 2003 and 20103–7 10 17 19 found that power/sprint disciplines show a similar ‘substance profile’ as ball sports.
Although endurance athletes rarely used NSAIDs (6.8%±0.2 vs 27.3%±0.4 in power/sprint disciplines), their declared use of corticosteroids (15.0%±0.3 vs 4.6%±0.1) and β-2-agonists (6.8±0.2 vs 2.3%±0.1) increased significantly (p<0.05). In popular events such as the Bonn Marathon 2009,20 Berlin Marathon 201021 and El Andalus Ultramarathon,22 47–61% of athletes used NSAIDs or other painkilling agents. The participants using NSAIDs had an almost five times higher incidence of adverse events (gastrointestinal cramps and bleeds, haematuria or cardiovascular events, such as arrhythmia and palpitation), which increased significantly with the analgesic dosage. It is noteworthy that serious adverse events occurred only in patients who were using NSAIDs (3 athletes with oliguria/anuria using ibuprofen, and 4 gastric bleeds, all using 500–1000 mg acetylsalicylic acid).21 It is alarming that most athletes are not aware of the potentially deleterious adverse effects of NSAIDs after strenuous exercise, and that physicians are rarely asked for advice prior to its use.16 20–23
The routine use of NSAIDs in sport is harmful in the short term and potentially also in the long term. Owing to its anti-inflammatory effect, NSAIDs delay bone healing,24 25 decrease protein synthesis and inhibit peritendinous hyperaemia and satellite cells in skeletal muscle after exercise.26–28 A randomised controlled trial has shown that NSAIDs permit earlier mobilisation, weight bearing and return to play compared with placebo after ankle sprains. However, there are also reports of more swelling, an increased incidence of residual instability and a decreased range of motion in ankles.29 This might be due to lower load-to-failure properties of the ‘healed’ ligament after the use of NSAIDs.30 Also, DOMS (delayed onset of muscle soreness) can be treated with NSAIDs to reduce pain and enable earlier return to play. However, accompanying muscle weakness and imbalance are not improved. A precipitate return to sport before muscular balance is re-established might put the player at risk for inappropriate biomechanical stress and overuse injuries.31 32
Knowledge translation and important questions
F-MARC campaigned to reduce the use of NSAIDs prior to the 2010 FIFA World Cup by informing all team physicians about NSAIDs and their potential side effects on recovery processes after exercise bouts and on tissue healing. Despite this initiative, the reported intake of NSAIDs remained unchanged in 2010 and 2014.
Our review poses several salient questions: What is the indication for which one-third of players use NSAIDs prior to every match, particularly when this greatly exceeds the rate of reported injuries during the FIFA World Cup? Is the high prescription practice due to a high number of non-time loss, chronic and overuse injuries?33 Are painkilling medications used routinely by the players to overcome fatigue and muscle soreness due to physical overload, or even improve recovery? Or has it simply become ‘part of the game’ for players and team physicians?
Footnotes
Competing interests: None.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.FIFA, Fédération Internationale de Football Association. FIFA Anti-Doping Regulations 2015. http://www.fifa.com/mm/document/footballdevelopment/medical/01/17/17/09/anti-dopingen_neutral.pdf (accessed 1 Mar 2015).
- 2.Corrigan B, Kazlauskas R. Medication use in athletes selected for doping control at the Sydney Olympics (2000). Clin J Sports Med 2003;13:33–40. 10.1097/00042752-200301000-00007 [DOI] [PubMed] [Google Scholar]
- 3.Tsitsimpikou C, Tsiokanos A, Tsarouhas K, et al. . Medication use by athletes at the Athens 2004 Summer Olympic Games. Clin J Sports Med 2009;19:33–8. 10.1097/JSM.0b013e31818f169e [DOI] [PubMed] [Google Scholar]
- 4.Thuyne WV, Delbeke FT. Declared use of medication in sports. Clin J Sports Med 2008;18:143–7. 10.1097/JSM.0b013e318163f220 [DOI] [PubMed] [Google Scholar]
- 5.Tscholl P, Alonso JM, Dolle G, et al. . The use of drugs and nutritional supplements in top-level track and field athletes. Am J Sports Med 2010;38:133–40. 10.1177/0363546509344071 [DOI] [PubMed] [Google Scholar]
- 6.Tscholl P, Feddermann N, Junge A, et al. . The use and abuse of painkillers in international soccer: data from 6 FIFA tournaments for female and youth players. Am J Sports Med 2009;37:260–5. 10.1177/0363546508324307 [DOI] [PubMed] [Google Scholar]
- 7.Tscholl P, Junge A, Dvorak J. The use of medication and nutritional supplements during FIFA World Cups 2002 and 2006. Br J Sports Med 2008;42:725–30. 10.1136/bjsm.2007.045187 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Tscholl PM, Dvorak J. Abuse of medication during international football competition in 2010—lesson not learned. Br J Sports Med 2012;46:1140–1. 10.1136/bjsports-2011-090806 [DOI] [PubMed] [Google Scholar]
- 9.Moynihan R, Heneghan C, Godlee F. Too much medicine: from evidence to action. BMJ 2013;347:f7141 10.1136/bmj.f7141 [DOI] [PubMed] [Google Scholar]
- 10.Alaranta A, Alaranta H, Heliovaara M, et al. . Ample use of physician-prescribed medications in Finnish elite athletes. Int J Sports Med 2006;27:919–25. 10.1055/s-2006-923811 [DOI] [PubMed] [Google Scholar]
- 11.Efe T, Sagnak E, Roessler PP, et al. . Penetration of topical diclofenac sodium 4% spray gel into the synovial tissue and synovial fluid of the knee: a randomised clinical trial. Knee Surg Sports Traumatol Arthrosc 2014;22:345–50. 10.1007/s00167-013-2408-0 [DOI] [PubMed] [Google Scholar]
- 12.Kuehl KS. Review of the efficacy and tolerability of the diclofenac epolamine topical patch 1.3% in patients with acute pain due to soft tissue injuries. Clin Ther 2010;32:1001–14. 10.1016/j.clinthera.2010.06.001 [DOI] [PubMed] [Google Scholar]
- 13.Orchard JW, Steet E, Massey A, et al. . Long-term safety of using local anesthetic injections in professional rugby league. Am J Sports Med 2010;38:2259–66. 10.1177/0363546510372796 [DOI] [PubMed] [Google Scholar]
- 14.Sanchis-Gomar F, Pareja-Galeano H, Gomez-Cabrera MC, et al. . Allopurinol prevents cardiac and skeletal muscle damage in professional soccer players. Scand J Med Sci Sports 2015;25:e110–15. 10.1111/sms.12213 [DOI] [PubMed] [Google Scholar]
- 15.Wharam PC, Speedy DB, Noakes TD, et al. . NSAID use increases the risk of developing hyponatremia during an Ironman triathlon. Med Sci Sports Exerc 2006;38:618–22. 10.1249/01.mss.0000210209.40694.09 [DOI] [PubMed] [Google Scholar]
- 16.Holmes N, Cronholm PF, Duffy AJ III, et al. . Nonsteroidal anti-inflammatory drug use in collegiate football players. Clin J Sports Med 2013;23:283–6. 10.1097/JSM.0b013e318286d0fa [DOI] [PubMed] [Google Scholar]
- 17.Warner DC, Schnepf G, Barrett MS, et al. . Prevalence, attitudes, and behaviors related to the use of nonsteroidal anti-inflammatory drugs (NSAIDs) in student athletes. J Adolesc Health 2002;30:150–3. 10.1016/S1054-139X(01)00325-1 [DOI] [PubMed] [Google Scholar]
- 18.Tscholl PM, Alonso JM, Junge A, et al. Risk factors for the use of medication in elite athletes. Paper presented at: Oslo: ECSS, 2009. [Google Scholar]
- 19.Huang SH, Johnson K, Pipe AL. The use of dietary supplements and medications by Canadian athletes at the Atlanta and Sydney Olympic Games. Clin J Sports Med 2006;16:27–33. 10.1097/01.jsm.0000194766.35443.9c [DOI] [PubMed] [Google Scholar]
- 20.Brune K, Niederweis U, Kaufmann A, et al. . [Drug use in participants of the Bonn Marthon 2009]. MMW Fortschr Med 2009;151:39–41. [PubMed] [Google Scholar]
- 21.Küster M, Renner B, Oppel P, et al. . Consumption of analgesics before a marathon and the incidence of cardiovascular, gastrointestinal and renal problems: a cohort study. BMJ Open 2013;3:e002090 10.1136/bmjopen-2012-002090 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Scheer BV, Murray A. Al Andalus Ultra Trail: an observation of medical interventions during a 219-m, 5-day ultramarathon stage race. Clin J Sports Med 2011;21:444–6. 10.1097/JSM.0b013e318225b0df [DOI] [PubMed] [Google Scholar]
- 23.Gorski T, Cadore EL, Pinto SS, et al. . Use of NSAIDs in triathletes: prevalence, level of awareness and reasons for use. Br J Sports Med 2011;45:85–90. 10.1136/bjsm.2009.062166 [DOI] [PubMed] [Google Scholar]
- 24.Bergenstock M, Min W, Simon AM, et al. . A comparison between the effects of acetaminophen and celecoxib on bone fracture healing in rats. J Orthop Trauma 2005;19:717–23. 10.1097/01.bot.0000184144.98071.5d [DOI] [PubMed] [Google Scholar]
- 25.Giannoudis PV, MacDonald DA, Matthews SJ, et al. . Nonunion of the femoral diaphysis. The influence of reaming and non-steroidal anti-inflammatory drugs. J Bone Joint Surg Br 2000;82:655–8. 10.1302/0301-620X.82B5.9899 [DOI] [PubMed] [Google Scholar]
- 26.Kjaer M, Bayer ML, Eliasson P, et al. . What is the impact of inflammation on the critical interplay between mechanical signaling and biochemical changes in tendon matrix? J Appl Physio 2013;115:879–83. 10.1152/japplphysiol.00120.2013 [DOI] [PubMed] [Google Scholar]
- 27.Trappe TA, White F, Lambert CP, et al. . Effect of ibuprofen and acetaminophen on postexercise muscle protein synthesis. Am J Physiol Endocrinol Metab 2002;282:E551–6. 10.1152/ajpendo.00352.2001 [DOI] [PubMed] [Google Scholar]
- 28.Mackey AL. Does an NSAID a day keep satellite cells at bay? J Appl Physiol 2013;115:900–8. 10.1152/japplphysiol.00044.2013 [DOI] [PubMed] [Google Scholar]
- 29.Slatyer MA, Hensley MJ, Lopert R. A randomized controlled trial of piroxicam in the management of acute ankle sprain in Australian Regular Army recruits. The Kapooka Ankle Sprain Study. Am J Sports Med 1997;25:544–53. 10.1177/036354659702500419 [DOI] [PubMed] [Google Scholar]
- 30.Elder CL, Dahners LE, Weinhold PS. A cyclooxygenase-2 inhibitor impairs ligament healing in the rat. Am J Sports Med 2001;29:801–5. [DOI] [PubMed] [Google Scholar]
- 31.Lewis PB, Ruby D, Bush-Joseph CA. Muscle soreness and delayed-onset muscle soreness. Clin Sports Med 2012;31:255–62. 10.1016/j.csm.2011.09.009 [DOI] [PubMed] [Google Scholar]
- 32.Mackey AL, Mikkelsen UR, Magnusson SP, et al. . Rehabilitation of muscle after injury—the role of anti-inflammatory drugs. Scan J Med Sci Sports 2012;22:e8–14. 10.1111/j.1600-0838.2012.01463.x [DOI] [PubMed] [Google Scholar]
- 33.Clarsen B, Myklebust G, Bahr R. Development and validation of a new method for the registration of overuse injuries in sports injury epidemiology: the Oslo Sports Trauma Research Centre (OSTRC) overuse injury questionnaire. Br J Sports Med 2013;47:495–502. 10.1136/bjsports-2012-091524 [DOI] [PubMed] [Google Scholar]