

Abstract
Aims
The associations of mitral annular calcification (MAC) with atrial fibrillation (AF) risk factors and related outcomes suggest a possible association between MAC and AF. The aim of this study was to examine the association between MAC and AF in a racially and ethnically diverse population.
Methods and results
This analysis included 6641 participants (mean age 62 ± 10 years; 53% women; 27% Blacks; 22% Hispanics; 12% Chinese-Americans) from the Multi-Ethnic Study of Atherosclerosis (MESA) who were free of clinical cardiovascular disease and AF at baseline. The presence of MAC was defined by cardiac computed tomography (CT) as an Agatston score >0. Atrial fibrillation was ascertained by hospital discharge records and from Medicare claims data until 31 December 2010. Cox regression was used to compute hazard ratios (HRs) and 95% confidence intervals (95% CIs) for the association between MAC and AF. At baseline, 619 (9.3%) participants had MAC. Over a median follow-up of 8.5 years, 308 (4.6%) participants developed AF. In a multivariable adjusted model, MAC was associated with an increased risk of AF (HR = 1.9, 95% CI = 1.5, 2.5). This association was consistent across subgroups of age, sex, race/ethnicity (Whites vs. non-Whites), hypertension, diabetes, and left atrial enlargement. The addition of MAC to the Framingham Heart Study and CHARGE AF risk scores for AF improved the C-statistics from 0.769 to 0.776 (P = 0.038) and 0.788 to 0.792 (P = 0.089), respectively.
Conclusion
The presence of MAC was predictive of incident AF in MESA. Potentially, these findings suggest a usefulness of cardiac CT to identify individuals at risk for AF.
Keywords: Mitral annulus calcification, Epidemiology, Atrial fibrillation
What's new?
Currently, it is unknown if mitral annular calcium (MAC), detected by a more precise imaging modality such as cardiac computed tomography (CT), is a risk factor for atrial fibrillation (AF) and whether such an association exists in a racially and ethnically diverse population.
Using data from the Multi-Ethnic Study of Atherosclerosis, we showed that MAC is associated with incident AF and this association does not differ by age, sex, race/ethnicity, hypertension, diabetes, or left atrial enlargement. Additionally, we showed that MAC improves discrimination of AF prediction beyond variables included in common risk scores for AF.
These findings suggest a potential usefulness of cardiac CT to identify individuals at risk for developing AF.
Introduction
Mitral annular calcification (MAC) is a chronic degenerative process that affects the base of the mitral valve. Several atrial fibrillation (AF) risk factors such as diabetes and hypertension have been associated with the presence of MAC.1,2 Also, it has been shown that MAC is an independent predictor of future cardiovascular events.3–6 This includes outcomes that have been linked to AF such as myocardial infarction and ischaemic stroke.7,8 These findings suggest a potential association between MAC and AF.
In the Framingham Heart Study, MAC was associated with the development of AF.9 However, this study consists of a predominantly White population and MAC was measured by echocardiography. Currently, it is unknown whether MAC, detected by a more precise imaging modality such as computed tomography (CT), is a risk factor for AF and whether such an association exists in a racially and ethnically diverse population.
The purpose of this study was to examine the association between MAC and incident AF in the Multi-Ethnic Study of Atherosclerosis (MESA). The diverse population of MESA allowed us to examine whether differences between MAC and incident AF exist by race and/or ethnicity. Also, cardiac CT was used to measure MAC and the association between MAC and AF has not been examined using this technique.
Methods
Study population
Details of MESA have been described previously.10 Briefly, between July 2000 and September 2002, 6814 participants were recruited at six field centres in the USA (Baltimore, ML; Chicago, IL; Forsyth County, NC; Los Angeles, CA; New York, NY; and St. Paul, MN). Requirement for study participation included age between 45 and 84 years and for participants not to have clinical cardiovascular disease at the time of study enrollment. For the purpose of this analysis, participants were excluded if they did not undergo baseline MAC measurement, baseline AF was present, or if baseline characteristics and/or follow-up data were missing.
Mitral annular calcification
Mitral annular calcification was assessed by cardiac CT at study enrollment using either cardiac-gated electron-beam CT or multi-detector CT systems depending on the study site.11 All participants in MESA underwent two consecutive scans and the mean MAC value was recorded. The two scans were analysed separately for MAC by two independent analysts. Inter-observer and intra-observer agreement between different CT image analysts who measured MAC on the same cardiac CT image were excellent and have been previously reported.11,12 The MAC score was computed using the phantom-adjusted Agatston method.13 Mitral annular calcification was defined by the presence of calcium (Agatston score >0) on the mitral valve.
Atrial fibrillation
Follow-up phone calls to study participants every 9–12 months were used to identify hospitalizations and medical records, including discharge records. Additionally, for participants ≥65 years enrolled in fee-for-service Medicare, Medicare claims data were used to identify inpatient AF cases. Incident AF was defined by International Classification of Disease Ninth Revision codes 427.31 or 427.32.
Baseline characteristics
Participant characteristics collected during the initial MESA visit were used in this analysis. Age, sex, race/ethnicity, income, and education were self-reported. Annual income was categorized into three levels (<$20 000, $20 000–$49 999, and ≥$50 000). Similarly, education was categorized into ‘high school or less,’ ‘some college,’ and ‘college or more.’ Smoking was defined as ever (e.g. current or former) or never smoker. Blood samples were obtained after a 12 h fast and measurements of total cholesterol, high-density lipoprotein (HDL) cholesterol, plasma glucose, and high-sensitivity C-reactive protein (hs-CRP) were used in this analysis. Additionally, a subgroup of study participants' blood samples were analysed for levels of amino-terminal-pro-brain natriuretic peptide (NT-proBNP) and these values were used. Diabetes was defined as fasting glucose values ≥126 mg/dL or a history of diabetes medication use. After the participant rested for 5 min in a seated position, blood pressure was recorded three separate times and the mean of the last two values was used in this analysis. Hypertension was defined as a systolic/diastolic blood pressure values ≥140/90 mm Hg and/or a history of antihypertensive medication use. The use of aspirin, statins, and antihypertensive and lipid-lowering medications were self-reported. Body mass index was computed as the weight in kilograms divided by the square of the height in meters. Using baseline electrocardiogram data, left ventricular hypertrophy was defined by the Cornell criteria (R wave amplitude AVL plus S wave amplitude V3 ≥2800 mm for men and ≥2000 mm for women) and left atrial enlargement was defined by Novacode criteria (Novacode 7.1).14,15 In a subgroup of MESA participants who had cardiac magnetic resonance imaging (MRI) data (N = 4 896), left ventricular end-diastolic mass and left ventricular ejection fraction were recorded. Briefly, whole-body MRI scanners using electrocardiogram triggered segmented k-space fast gradient-echo pulse sequences during breath holds were used. Myocardial horizontal and vertical tagging were performed on three left ventricular short-axis slices (base, mid, and apex) by non-selective radiofrequency pulses separated by a spatial modulation of magnetization-encoding gradients. Imaging and analytical methods for this technique have been described.16
Statistical analysis
Categorical variables were reported as frequency and percentage while continuous variables were recorded as mean ± standard deviation. Statistical significance for categorical variables was tested using the χ2 method and the Wilcoxon rank-sum procedure for continuous variables. Follow-up time was defined as the time between the initial study visit until the diagnosis of AF or until death, loss to follow-up, or end of follow-up which was 31 December 2010. Kaplan–Meier estimates were used to compute cumulative incidence of AF by MAC and the difference in estimates was compared using the log-rank procedure.17 Cox proportional-hazards regression was used to compute hazard ratios (HRs) and 95% confidence intervals (95% CI) for the association between MAC and AF. In all models, the association of MAC and AF was assessed by the presence of MAC (Agatston score >0) vs. no MAC (Agatston score = 0). Additionally, MAC scores were analysed as a continuous variable using the base-2 logarithm of the MAC score plus one (log2[MAC + 1]) to examine the risk of AF when the MAC score doubles. The addition of one allows for non-zero values to be included. We also constructed a restricted cubic spline model to examine the graphical dose–response relationship between MAC and the multivariable HR for AF and incorporated knots at the 5th, 50th, and 95th percentiles.18 Multivariable models were constructed with incremental adjustments as follows: Model 1 adjusted for age, sex, race/ethnicity (Whites vs. non-Whites), income, and education; Model 2 adjusted for Model 1 covariates plus smoking status, systolic blood pressure, diabetes, body mass index, total cholesterol, HDL cholesterol, antihypertensive and lipid-lowering medication use, aspirin, hs-CRP, left ventricular hypertrophy, and left atrial enlargement. We tested for interactions between our main effect variable and age (dichotomized at 65 years), sex, race/ethnicity (Whites vs. non-Whites), hypertension, diabetes, and left atrial enlargement.
Several sensitivity analyses were performed. In participants with available MRI data (N = 4 896), we further adjusted for left ventricular end-diastolic mass and left ventricular ejection fraction, separately. Similarly, we further adjusted for NT-proBNP (ln[NT-proBNP]) among participants who had baseline measurements (N = 5 490).19 Additionally, due to a potential relationship between MAC and coronary artery calcium (CAC), we further adjusted for this variable (log2[CAC + 1]) among participants with CAC data (N = 6 614).20
We assessed the ability of MAC to predict AF by computing the C-statistic using covariates from the Framingham Heart Study (age, sex, body mass index, systolic blood pressure, antihypertensive medication use, PR interval, clinically significant cardiac murmur, and heart failure) and the Cohorts for Heart and Aging Research in Genomic Epidemiology (CHARGE) AF (age, race, height, weight, systolic blood pressure, diastolic blood pressure, current smoking, antihypertensive medication use, diabetes, history of myocardial infarction, and history of heart failure, PR interval, and electrocardiogram-derived left ventricular hypertrophy) consortium risk models for AF.21,22 The Multi-Ethnic Study of Atherosclerosis participants had no evidence of clinical cardiovascular disease at baseline and these covariates were coded as not being present. The added predictive ability of MAC was evaluated by the difference in C-statistics of the models before and after inclusion of MAC in the predictive models. We additionally investigated the integrated discrimination improvement (IDI) and relative IDI.23 Integrated discrimination improvement quantifies the increase in the difference between the mean predicted risks for participants who do and do not develop AF after adding MAC to the model. Additionally, net reclassification improvement (NRI) which quantifies any desirable change in predicted risk was computed for the following risk categories: <2.5, 2.5–5%, >5%.24
The proportional-hazards assumption was not violated in our analysis. Statistical significance was defined as P< 0.05. SAS Version 9.3 was used for all analyses.
Results
Of the 6814 participants from the original MESA cohort, 58 participants had a diagnosis of AF before study enrollment. The majority of these cases were detected by Medicare linkage and only one case was present in the baseline electrocardiogram. Of those that remained, 6 participants with missing follow-up data, and 109 participants with either missing baseline characteristics or missing medication data also were excluded. A total of 6641 study participants (mean age 62 ± 10 years; 53% women; 38% Whites; 27% Blacks; 22% Hispanics; 12% Chinese-Americans) had available MAC measurements and were included in the final analysis.
A total of 619 (9.3%) study participants had baseline MAC. Baseline characteristics for study participants are shown in Table 1. Participants with MAC were more likely to be older, female, and to have lower levels of education and income compared with participants without MAC. A higher percentage of White participants (12%) were observed to have MAC compared with other races (7.4% Blacks; 10% Hispanics; 5.8% Chinese-Americans) (P < 0.0001). Participants with MAC had higher values for body mass index, hs-CRP, and systolic blood pressure, and also were more likely to be diabetic and to have left ventricular hypertrophy and left atrial enlargement. Additionally, these participants were more likely to use aspirin, statins, and antihypertensive and lipid-lowering medications.
Table 1.
Baseline characteristics of study participants stratified by MAC (N = 6641)
| Characteristic | MAC (n = 619) | No MAC (n = 6022) | P-value* |
|---|---|---|---|
| Age, mean (SD), years | 72 (7.7) | 61 (9.9) | <0.0001 |
| Male sex (%) | 248 (40) | 2882 (48) | 0.0002 |
| Race/ethnicity | |||
| White (%) | 301 (49) | 2248 (37) | |
| Black (%) | 134 (22) | 1689 (28) | |
| Chinese-American (%) | 36 (5.8) | 758 (13) | |
| Hispanic (%) | 148 (24) | 1327 (22) | <0.0001 |
| Education | |||
| High school or less (%) | 285 (46) | 2132 (35) | |
| Some college (%) | 157 (25) | 1735 (29) | |
| College or more (%) | 177 (29) | 2155 (36) | <0.0001 |
| Annual income | |||
| < $20 000 (%) | 248 (40) | 1531 (25) | |
| $20 000 to $49 999 (%) | 216 (35) | 2109 (35) | |
| ≥$50 000 (%) | 155 (25) | 2382 (40) | <0.0001 |
| Body mass index, mean (SD) kg/m2 | 29 (5.7) | 28 (5.5) | 0.0010 |
| Current or former smoker (%) | 303 (49) | 2984 (50) | 0.78 |
| Diabetes (%) | 136 (22) | 793 (13) | <0.0001 |
| Hypertension (%) | 423 (68) | 2742 (46) | <0.0001 |
| Systolic Blood Pressure, mean (SD), mm Hg | 135 (23) | 125 (21) | <0.0001 |
| Total cholesterol, mean (SD), mg/dL | 194 (38) | 194 (35) | 0.47 |
| HDL cholesterol, mean (SD), mg/dL | 52 (15) | 51 (15) | 0.082 |
| Antihypertensive medications (%) | 333 (54) | 2106 (35) | <0.0001 |
| Statins (%) | 145 (23) | 831 (14) | <0.0001 |
| Aspirin (%) | 204 (33) | 1,368 (23) | <0.0001 |
| Lipid-lowering medications (%) | 159 (26) | 904 (15) | <0.0001 |
| hs-CRP, mean (SD), mg/L | 3.9 (5.8) | 3.8 (5.9) | 0.017 |
| ECG-left ventricular hypertrophy (%) | 34 (5.5) | 222 (3.7) | 0.026 |
| ECG-left atrial enlargement (%) | 149 (24) | 846 (14) | <0.0001 |
ECG, electrocardiogram; HDL, high-density lipoprotein; hs-CRP, high-sensitivity C-reactive protein; MAC, mitral annular calcium; SD, standard deviation.
*Statistical significance for continuous data was tested using the Wilcoxon rank-sum procedure and categorical data were tested using the χ2 test.
Over a median follow-up of 8.5 years, 308 (4.6%) participants developed AF. The incidence rate of AF was almost four-fold greater in those with MAC than in those without MAC (incidence rates per 1000 person-years: MAC, 19.8 (95% CI = 16.0, 24.5); no MAC 4.8 (95% CI = 4.2, 5.5); P < 0.0001). Unadjusted cumulative incidence curves for AF by MAC are shown in Figure 1 (log-rank P < 0.0001).
Figure 1.

Unadjusted cumulative incidence of AF by MAC (N = 6641)*. *Cumulative incidence curves are different (log-rank P < 0.0001). AF, atrial fibrillation; MAC, mitral annular calcium.
In a multivariable Cox regression analysis, the presence of MAC was associated with almost double the risk of AF (Table 2). These results were consistent across subgroups stratified by age, sex, race/ethnicity (Whites vs. non-Whites), hypertension, diabetes, and left atrial enlargement (Table 2).
Table 2.
Risk of AF with MAC
| MAC events/no. at risk | No MAC events/no. at risk | Model 1a HR (95% CI) | P-value | Model 2b HR (95% CI) | P-value | Interaction P-valuec | |
|---|---|---|---|---|---|---|---|
| All participants | 85/619 | 223/6022 | 2.0 (1.5, 2.6) | <0.0001 | 1.9 (1.5, 2.5) | <0.0001 | – |
| Age, years | |||||||
| <65 | 4/95 | 56/3683 | 2.5 (0.90, 6.9) | 0.081 | 1.3 (0.44, 3.7) | 0.66 | 0.88 |
| ≥65 | 81/524 | 167/2339 | 2.4 (1.8, 3.1) | <0.0001 | 2.3 (1.8, 3.0) | <0.0001 | |
| Sex | |||||||
| Female | 39/371 | 80/3140 | 2.1 (1.4, 3.2) | 0.0004 | 1.9 (1.3, 2.9) | 0.0023 | 0.79 |
| Male | 46/248 | 143/2882 | 1.9 (1.4, 2.8) | 0.0002 | 1.9 (1.3, 2.7) | 0.0004 | |
| Race | |||||||
| White | 50/301 | 118/2248 | 1.8 (1.3, 2.5) | 0.0012 | 1.7 (1.2, 2.4) | 0.0034 | 0.33 |
| Non-White | 35/318 | 105/3774 | 2.4 (1.6, 3.6) | <0.0001 | 2.2 (1.5, 3.4) | <0.0001 | |
| Hypertension | |||||||
| No | 15/195 | 66/3259 | 1.4 (0.75, 2.5) | 0.32 | 1.4 (0.74, 2.5) | 0.32 | 0.76 |
| Yes | 70/424 | 157/2763 | 2.2 (1.6, 2.9) | <0.0001 | 2.1 (1.6, 2.8) | <0.0001 | |
| Diabetes | |||||||
| No | 66/483 | 191/5229 | 1.8 (1.4, 2.5) | <0.0001 | 1.8 (1.3, 2.4) | 0.0002 | 0.36 |
| Yes | 19/136 | 32/793 | 3.3 (1.8, 6.1) | 0.0001 | 3.2 (1.7, 6.0) | 0.0003 | |
| Left atrial enlargement | |||||||
| No | 61/470 | 176/5176 | 1.9 (1.4, 2.6) | <0.0001 | 1.8 (1.3, 2.5) | 0.0001 | 0.75 |
| Yes | 24/149 | 47/846 | 2.2 (1.3, 3.7) | 0.0045 | 2.2 (1.3, 3.9) | 0.0034 | |
AF, atrial fibrillation; CI, confidence interval; HDL, high-density lipoprotein; hs-CRP, high-sensitivity C-reactive protein; HR, hazard ratio; MAC, mitral annular calcium.
aAdjusted for age, sex, race/ethnicity, income, and education.
bAdjusted for Model 1 plus smoking status, systolic blood pressure, diabetes, body-mass index, total cholesterol, HDL-cholesterol, antihypertensive and lipid-lowering medications, aspirin, hs-CRP, left ventricular hypertrophy, and left atrial enlargement.
cInteractions tested using Model 2.
We observed a dose–response relationship between MAC and the risk of AF. When MAC was used in a restricted cubic spline model as a continuous variable (log2[MAC + 1]), doubling of the MAC score was associated with a 20% increase in the risk of AF in an unadjusted model (HR = 1.2, 95% CI = 1.18, 1.3) and a 10% increased risk when adjusted for covariates in Model 1 (HR = 1.1, 95% CI = 1.08, 1.2) and Model 2 (HR = 1.1, 95% CI = 1.08, 1.2). Figure 2 shows the association of MAC with AF across MAC values.
Figure 2.
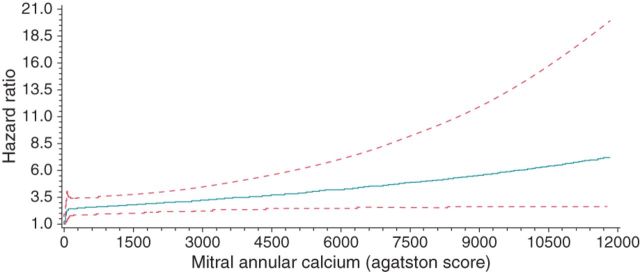
Multivariable-Adjusted Risk of AF by MAC*. *Each HR was computed with the median MAC value of 0 as the reference and was adjusted for age, sex, and race/ethnicity. Dotted-lines represent the 95% confidence interval. AF, atrial fibrillation; MAC, mitral annular calcium; HR, hazard ratio.
The association between MAC and AF remained significant after further adjustment of Model 2 for left ventricular end-diastolic mass (HR = 2.2, 95% CI = 1.6, 3.1), left ventricular ejection fraction (HR = 2.4, 95% CI = 1.7, 3.3), NT-proBNP (HR = 1.6, 95% CI = 1.2, 2.1), and CAC (HR = 1.8, 95% CI = 1.3, 2.3), separately.
The addition of MAC to the Framingham Heart Study and CHARGE AF risk scores improved the C-statistics from 0.769 to 0.776 (P = 0.038) and 0.788 to 0.792 (P = 0.089), respectively. Also, the addition of MAC to the Framingham Heart Study and the CHARGE AF risk scores yielded an IDI of 0.0037 (95% CI = 0.0017, 0.073) and 0.0028 (95% CI = 0.0008, 0.0061) with relative IDI of 0.12 (95% CI = 0.055, 0.18) and 0.077 (95% CI = 0.023, 0.13), and categorical NRI of 0.050 (95% CI = 0.021, 0.093) and 0.039 (95% CI = 0.014, 0.078), respectively.
Discussion
In this analysis from MESA, the presence of MAC was associated with an increased risk of incident AF. This association was consistent across subgroups stratified by age, sex, race/ethnicity, hypertension, diabetes, and left atrial enlargement. The risk of AF was shown to increase with higher levels of MAC, suggesting that the level of MAC severity plays a role in the magnitude of AF risk. Additionally, MAC was found to improve reclassification beyond variables included in the Framingham Heart Study and CHARGE AF risk scores for AF prediction.
Mitral annular calcification has been shown to predict incident AF in the Framingham Heart Study and results were similar to those presented in this report (HR = 1.6, 95% CI = 1.1, 2.2).9 In contrast with our study in which MAC was detected by cardiac CT, MAC was measured by echocardiography in the Framingham Study. Mitral annular calcification measurements by echocardiography were not obtained in MESA and we were unable to directly compare the results from the Framingham Study with our results. However, it has been proposed that CT is a better method to detect valvular calcification compared with echocardiography.2 Additionally, the Framingham Heart Study is limited regarding racial and ethnic diversity. To our knowledge, our study is the first to report the association of MAC with incident AF in a racially and ethnically diverse population by cardiac CT.
Several cardiovascular risk factors which also are risk factors for AF have been associated with the progression of MAC.1,2,21,25 These include older age, White race, diabetes, and hypertension.25,26 Therefore, it is plausible that the presence of MAC reflects the detection of patients who are more likely to develop AF as they share similar risk factors. However, MAC was a significant predictor of AF after adjustment for these potential confounders, suggesting that MAC is independently associated with an increased risk of AF.
Mitral annular calcification has been associated with enlarged left atria in the Strong Heart Study and the association of left atrial size with AF is well established.27–30 Furthermore, in the Framingham Heart Study, the association between MAC and incident AF was attenuated after adjustment for left atrial size measured by echocardiography (HR = 1.4, 95% CI = 0.9, 2.0).9 These findings suggest that the association between MAC and AF is mediated by left atrial enlargement. It also is plausible that the presence of MAC coincides with enlarged left atria and MAC identifies persons who are more likely to have enlargement of these structures. However, our results show that the association between MAC and AF does not differ by electrocardiogram-diagnosed left atrial enlargement and our results remained significant after adjusting for this variable. The differences between the current study and the results reported from Framingham possibly are explained by differences in population diversity and/or the detection method of MAC. For example, Whites have a higher prevalence of AF and larger left atrial dimensions than Blacks.31 Potentially, adjustment for left atrial enlargement did not have the same impact in the racially and ethnically diverse population of MESA compared with the predominantly White population of the Framingham Study. Additionally, left atrial enlargement in our study was defined by electrocardiographic data. However, this method has been shown to be specific and highly predictive of left atrial enlargement when measurements were confirmed by echocardiography.32
The degenerative calcification of the mitral valve has been closely linked with systemic inflammation.33 Additionally, persons with AF have been shown to have higher levels of inflammatory markers than persons without AF.34 Potentially, the association of MAC with AF is mediated through inflammatory processes as evidenced by systemic biomarkers. However, our results remained significant after adjustment for markers of inflammation, suggesting that the relationship between MAC and AF unlikely is to be fully explained by inflammation.
Our results should be read in the context of certain limitations. AF cases were ascertained from hospitalization discharge records and inpatient Medicare claims data using International Classification of Disease codes which possibly resulted in misclassification. However, this method has been reported to have adequate positive predictive value for identifying AF events.35,36 Paroxysmal AF cases potentially were missed due to the time-dependent nature of this condition. Routine monitoring for AF (e.g. Holter monitors) was not performed in MESA and therefore asymptomatic cases of AF possibly were missed. However, we do not know of any reason to suggest that the resulting bias, if any, would have been differential in nature, rather than merely reducing effect estimates toward the null (e.g. diminishing power to detect a statistically significant result). Several potential confounders were included in our multivariable models that likely influenced the development of AF but we acknowledge that residual confounding remains a possibility. For example, the duration and severity of these potential confounders were unable to be fully adjusted for in our models (e.g. duration of hypertension, glucose control in diabetics, and continued tobacco use). Computed tomography allows excellent visualization of the anatomical details of the mitral valve and reliably measures the amount of calcification on the mitral valve annulus.37 However, the utility of this measurement regarding AF risk assessment remains uncertain and further research is needed to determine its clinical significance. Potentially, persons who undergo cardiac CT for evaluation of chest pain are able to simultaneously be screened for AF risk using MAC measurements.38
Conclusion
In conclusion, we have shown that MAC is independently associated with an increased risk of AF and improves AF risk prediction. These findings suggest a potential usefulness of cardiac CT to identify individuals at risk for developing AF.
Funding
This research was supported by contracts N01-HC-95159 through N01-HC-95169 from the National Heart, Lung, and Blood Institute and by grants UL1-RR-024156 and UL1-RR-025005 from NCRR.
Acknowledgements
The authors thank the other investigators, the staff, and the participants of the MESA study for their valuable contributions. A full list of participating MESA investigators and institutions can be found at http://www.mesa-nhlbi.org.
Conflict of interest: S.N. is a consultant and principal investigator for research funding awarded to Johns Hopkins University from Biosense Webster Inc.
References
- 1.Elmariah S, Budoff MJ, Delaney JA, Hamirani Y, Eng J, Fuster V, et al. Risk factors associated with the incidence and progression of mitral annulus calcification: the multi-ethnic study of atherosclerosis. Am Heart J. 2013;166:904–12. doi: 10.1016/j.ahj.2013.08.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Kanjanauthai S, Nasir K, Katz R, Rivera JJ, Takasu J, Blumenthal RS, et al. Relationships of mitral annular calcification to cardiovascular risk factors: the Multi-Ethnic Study of Atherosclerosis (MESA) Atherosclerosis. 2010;213:558–62. doi: 10.1016/j.atherosclerosis.2010.08.072. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Potpara TS, Vasiljevic ZM, Vujisic-Tesic BD, Marinkovic JM, Polovina MM, Stepanovic JM, et al. Mitral annular calcification predicts cardiovascular morbidity and mortality in middle-aged patients with atrial fibrillation: the Belgrade Atrial Fibrillation Study. Chest. 2011;140:902–10. doi: 10.1378/chest.10-2963. [DOI] [PubMed] [Google Scholar]
- 4.Fox CS, Vasan RS, Parise H, Levy D, O'Donnell CJ, D'Agostino RB, et al. Mitral annular calcification predicts cardiovascular morbidity and mortality: the Framingham Heart Study. Circulation. 2003;107:1492–6. doi: 10.1161/01.cir.0000058168.26163.bc. [DOI] [PubMed] [Google Scholar]
- 5.Fox E, Harkins D, Taylor H, McMullan M, Han H, Samdarshi T, et al. Epidemiology of mitral annular calcification and its predictive value for coronary events in African Americans: the Jackson Cohort of the Atherosclerotic Risk in Communities Study. Am Heart J. 2004;148:979–84. doi: 10.1016/j.ahj.2004.05.048. [DOI] [PubMed] [Google Scholar]
- 6.Kohsaka S, Jin Z, Rundek T, Boden-Albala B, Homma S, Sacco RL, et al. Impact of mitral annular calcification on cardiovascular events in a multiethnic community: the Northern Manhattan Study. JACC. 2008;1:617–23. doi: 10.1016/j.jcmg.2008.07.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Soliman EZ, Safford MM, Muntner P, Khodneva Y, Dawood FZ, Zakai NA, et al. Atrial fibrillation and the risk of myocardial infarction. JAMA Intern Med. 2014;174:107–14. doi: 10.1001/jamainternmed.2013.11912. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Wolf PA, Abbott RD, Kannel WB. Atrial fibrillation as an independent risk factor for stroke: the Framingham Study. Stroke. 1991;22:983–8. doi: 10.1161/01.str.22.8.983. [DOI] [PubMed] [Google Scholar]
- 9.Fox CS, Parise H, Vasan RS, Levy D, O'Donnell CJ, D'Agostino RB, et al. Mitral annular calcification is a predictor for incident atrial fibrillation. Atherosclerosis. 2004;173:291–4. doi: 10.1016/j.atherosclerosis.2003.12.018. [DOI] [PubMed] [Google Scholar]
- 10.Bild DE, Bluemke DA, Burke GL, Detrano R, Diez Roux AV, Folsom AR, et al. Multi-ethnic study of atherosclerosis: objectives and design. Am J Epidemiol. 2002;156:871–81. doi: 10.1093/aje/kwf113. [DOI] [PubMed] [Google Scholar]
- 11.Carr JJ, Nelson JC, Wong ND, McNitt-Gray M, Arad Y, Jacobs DR, Jr, et al. Calcified coronary artery plaque measurement with cardiac CT in population-based studies: standardized protocol of Multi-Ethnic Study of Atherosclerosis (MESA) and Coronary Artery Risk Development in Young Adults (CARDIA) study. Radiology. 2005;234:35–43. doi: 10.1148/radiol.2341040439. [DOI] [PubMed] [Google Scholar]
- 12.Budoff MJ, Takasu J, Katz R, Mao S, Shavelle DM, O'Brien KD, et al. Reproducibility of CT measurements of aortic valve calcification, mitral annulus calcification, and aortic wall calcification in the multi-ethnic study of atherosclerosis. Acad Radiol. 2006;13:166–72. doi: 10.1016/j.acra.2005.09.090. [DOI] [PubMed] [Google Scholar]
- 13.Agatston AS, Janowitz WR, Hildner FJ, Zusmer NR, Viamonte M, Jr, Detrano R. Quantification of coronary artery calcium using ultrafast computed tomography. J Am Coll Cardiol. 1990;15:827–32. doi: 10.1016/0735-1097(90)90282-t. [DOI] [PubMed] [Google Scholar]
- 14.Devereux RB, Casale PN, Eisenberg RR, Miller DH, Kligfield P. Electrocardiographic detection of left ventricular hypertrophy using echocardiographic determination of left ventricular mass as the reference standard. Comparison of standard criteria, computer diagnosis and physician interpretation. J Am Coll Cardiol. 1984;3:82–7. doi: 10.1016/s0735-1097(84)80433-7. [DOI] [PubMed] [Google Scholar]
- 15.Rautaharju PM, Park LP, Chaitman BR, Rautaharju F, Zhang ZM. The Novacode criteria for classification of ECG abnormalities and their clinically significant progression and regression. J Electrocardiol. 1998;31:157–87. [PubMed] [Google Scholar]
- 16.Fernandes VR, Cheng S, Cheng YJ, Rosen B, Agarwal S, McClelland RL, et al. Racial and ethnic differences in subclinical myocardial function: the Multi-Ethnic Study of Atherosclerosis. Heart. 2011;97:405–10. doi: 10.1136/hrt.2010.209452. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Gray RJ, Tsiatis AA. A linear rank test for use when the main interest is in differences in cure rates. Biometrics. 1989;45:899–904. [PubMed] [Google Scholar]
- 18.Marrie RA, Dawson NV, Garland A. Quantile regression and restricted cubic splines are useful for exploring relationships between continuous variables. J Clin Epidemiol. 2009;62:511–7 e1. doi: 10.1016/j.jclinepi.2008.05.015. [DOI] [PubMed] [Google Scholar]
- 19.Patton KK, Heckbert SR, Alonso A, Bahrami H, Lima JA, Burke G, et al. N-terminal pro-B-type natriuretic peptide as a predictor of incident atrial fibrillation in the Multi-Ethnic Study of Atherosclerosis: the effects of age, sex and ethnicity. Heart. 2013;99:1832–6. doi: 10.1136/heartjnl-2013-304724. [DOI] [PubMed] [Google Scholar]
- 20.Hamirani YS, Nasir K, Blumenthal RS, Takasu J, Shavelle D, Kronmal R, et al. Relation of mitral annular calcium and coronary calcium (from the Multi-Ethnic Study of Atherosclerosis [MESA]) Am J Cardiol. 2011;107:1291–4. doi: 10.1016/j.amjcard.2011.01.005. [DOI] [PubMed] [Google Scholar]
- 21.Schnabel RB, Sullivan LM, Levy D, Pencina MJ, Massaro JM, D'Agostino RB, Sr, et al. Development of a risk score for atrial fibrillation (Framingham Heart Study): a community-based cohort study. Lancet. 2009;373:739–45. doi: 10.1016/S0140-6736(09)60443-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Alonso A, Krijthe BP, Aspelund T, Stepas KA, Pencina MJ, Moser CB, et al. Simple risk model predicts incidence of atrial fibrillation in a racially and geographically diverse population: the CHARGE-AF consortium. J Am Heart Assoc. 2013;2:e000102. doi: 10.1161/JAHA.112.000102. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Pencina MJ, D'Agostino RB, Sr, D'Agostino RB, Jr, Vasan RS. Evaluating the added predictive ability of a new marker: from area under the ROC curve to reclassification and beyond. Stat Med. 2008;27:157–72. doi: 10.1002/sim.2929. [DOI] [PubMed] [Google Scholar]
- 24.Pencina MJ, D'Agostino RB, Sr, Steyerberg EW. Extensions of net reclassification improvement calculations to measure usefulness of new biomarkers. Stat Med. 2011;30:11–21. doi: 10.1002/sim.4085. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Kannel WB, Wolf PA, Benjamin EJ, Levy D. Prevalence, incidence, prognosis, and predisposing conditions for atrial fibrillation: population-based estimates. Am J Cardiol. 1998;82:2N–9N. doi: 10.1016/s0002-9149(98)00583-9. [DOI] [PubMed] [Google Scholar]
- 26.Go AS, Hylek EM, Phillips KA, Chang Y, Henault LE, Selby JV, et al. Prevalence of diagnosed atrial fibrillation in adults: national implications for rhythm management and stroke prevention: the AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study. JAMA. 2001;285:2370–5. doi: 10.1001/jama.285.18.2370. [DOI] [PubMed] [Google Scholar]
- 27.Kizer JR, Bella JN, Palmieri V, Liu JE, Best LG, Lee ET, et al. Left atrial diameter as an independent predictor of first clinical cardiovascular events in middle-aged and elderly adults: the Strong Heart Study (SHS) Am Heart J. 2006;151:412–8. doi: 10.1016/j.ahj.2005.04.031. [DOI] [PubMed] [Google Scholar]
- 28.Parkash R, Green MS, Kerr CR, Connolly SJ, Klein GJ, Sheldon R, et al. The association of left atrial size and occurrence of atrial fibrillation: a prospective cohort study from the Canadian Registry of Atrial Fibrillation. Am Heart J. 2004;148:649–54. doi: 10.1016/j.ahj.2004.04.029. [DOI] [PubMed] [Google Scholar]
- 29.Henry WL, Morganroth J, Pearlman AS, Clark CE, Redwood DR, Itscoitz SB, et al. Relation between echocardiographically determined left atrial size and atrial fibrillation. Circulation. 1976;53:273–9. doi: 10.1161/01.cir.53.2.273. [DOI] [PubMed] [Google Scholar]
- 30.Dittrich HC, Pearce LA, Asinger RW, McBride R, Webel R, Zabalgoitia M, et al. Left atrial diameter in nonvalvular atrial fibrillation: an echocardiographic study. Stroke prevention in atrial fibrillation investigators. Am Heart J. 1999;137:494–9. doi: 10.1016/s0002-8703(99)70498-9. [DOI] [PubMed] [Google Scholar]
- 31.Marcus GM, Olgin JE, Whooley M, Vittinghoff E, Stone KL, Mehra R, et al. Racial differences in atrial fibrillation prevalence and left atrial size. Am J Med. 2010;123:375 e1–7. doi: 10.1016/j.amjmed.2009.05.019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Hazen MS, Marwick TH, Underwood DA. Diagnostic accuracy of the resting electrocardiogram in detection and estimation of left atrial enlargement: an echocardiographic correlation in 551 patients. Am Heart J. 1991;122:823–8. doi: 10.1016/0002-8703(91)90531-l. [DOI] [PubMed] [Google Scholar]
- 33.Fox CS, Guo CY, Larson MG, Vasan RS, Parise H, O'Donnell CJ, et al. Relations of inflammation and novel risk factors to valvular calcification. Am J Cardiol. 2006;97:1502–5. doi: 10.1016/j.amjcard.2005.11.086. [DOI] [PubMed] [Google Scholar]
- 34.Aviles RJ, Martin DO, Apperson-Hansen C, Houghtaling PL, Rautaharju P, Kronmal RA, et al. Inflammation as a risk factor for atrial fibrillation. Circulation. 2003;108:3006–10. doi: 10.1161/01.CIR.0000103131.70301.4F. [DOI] [PubMed] [Google Scholar]
- 35.Alonso A, Agarwal SK, Soliman EZ, Ambrose M, Chamberlain AM, Prineas RJ, et al. Incidence of atrial fibrillation in Whites and African-Americans: the atherosclerosis risk in Communities (ARIC) study. Am Heart J. 2009;158:111–7. doi: 10.1016/j.ahj.2009.05.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Jensen PN, Johnson K, Floyd J, Heckbert SR, Carnahan R, Dublin S. A systematic review of validated methods for identifying atrial fibrillation using administrative data. Pharmacoepidemiol Drug Saf. 2012;21:141–7. doi: 10.1002/pds.2317. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Willmann JK, Kobza R, Roos JE, Lachat M, Jenni R, Hilfiker PR, et al. ECG-gated multi-detector row CT for assessment of mitral valve disease: initial experience. Eur Radiol. 2002;12:2662–9. doi: 10.1007/s00330-002-1454-7. [DOI] [PubMed] [Google Scholar]
- 38.Ladapo JA, Jaffer FA, Hoffmann U, Thomson CC, Bamberg F, Dec W, et al. Clinical outcomes and cost-effectiveness of coronary computed tomography angiography in the evaluation of patients with chest pain. J Am Coll Cardiol. 2009;54:2409–22. doi: 10.1016/j.jacc.2009.10.012. [DOI] [PubMed] [Google Scholar]