

Abstract
Objective:
The objective was to assess the clinical presentation, delay of diagnosis, and the causes of delay in the diagnosis of patients with pregnancy-associated breast cancer (PABC) and patients with non-PABC.
Patients and Methods:
This was a face-to-face interview with women who had histologically confirmed BC. All respondents were interviewed at our hospital.
Results:
We interviewed 56 patients, 36 with non-PABC and 20 with PABC. Of the 20 patients with PABC, BC was diagnosed in 12 (60%) during pregnancy and 8 (40%) during postpartum. 18 of the patients (90%) with PABC presented mainly with a mass 3 (15%) with pain and ulcer, 5 (25%) with skin redness and thickening, 6 (30%) with nipple retraction and 4 (20%) with discharge 12 (60%) patients with PABC had delayed diagnosis and 8 (40%) of this delay was due to physicians’ reassurance, and 2 (10%) because of fear of cancer. Similarly, 35 (97%) patients with non-PABC presented with breast mass, 3 (8.3%) with infrequent pain 4 (11.11%) with inflammation 2 (5.55%) with ulcer 2 (5.55%) with nipple discharge and4 (11.11%) with thickening of the skin compared with PABC patients. Only 4 (11.11%) in non-PABC had delayed diagnosis, and for half of them the delay was due to the fear of cancer. Two patients with PABC and non-PABC were afraid of cancer 16.66% and 5.55%, respectively. However, 8 (60%) of patients with PABC had delayed diagnosis compared to 0% of patients with non-PABC.
Conclusion:
In this study, the majority of patients with PABC or non-PABC presented with a breast lump. Other symptoms were more common in patients with PABC than in patients with non-PABC. An increased awareness of clinicians may help reduce delay in the diagnosis of patients with PABC.
Keywords: Breast, cancer, delay, pregnancy
INTRODUCTION
Breast cancer is an important health problem in Saudi Arabia, especially in the Eastern Province. It ranks first among all newly diagnosed malignant diseases in Saudi women, accounting for 25% in year 2008. The median age at diagnosis was 47 years.[1] The Eastern Region of Saudi Arabia recorded the highest age-standardized rate of 31.8/100,000 women of all the regions in the Kingdom of Saudi Arabia.[1] Breast cancer (BC) patients in the kingdom are one decade younger than in Europe.[2]
Pregnancy-associated breast cancer (PABC) is defined as BC that is diagnosed during pregnancy or within 1-year thereafter, including any time when a woman may be lactating. It is the most frequently diagnosed cancer that co-exists with pregnancy and lactation.[3,4,5,6,7]
To improve the outcome of BC treatment, there should be increased awareness among clinicians and a better understanding of the clinical presentation, predicting factors and causes. Delay in treatment is important since smaller tumors are more likely to be treated successfully. Delayed presentation of BC is associated with larger tumors at presentation, advanced stage, and low survival.[8,9,10,11,12]
In general, delay in diagnosis and treatment of cancer is divided into two: Patient delay, provider and referral delay. Patient delay is defined as the period from the onset of symptoms to the first medical consultation. Provider and referral delay covers the period from the first consultation to definite diagnosis and commencement of treatment.[13]
We conducted this study to assess the clinical presentation, delay of diagnosis, and the causes of delayed diagnosis of patients with PABC and patients with non-PABC in our hospital.
PATIENTS AND METHODS
Structured face-to-face interview was conducted after histological diagnosis of BC was confirmed at our hospital. The study was conducted at King Fahd Hospital of the University at Al-Khobar, KSA from 2007 to 2013.
The interview consisted of detailed questions on demographic characteristics of our patients, clinical presentation including breast mass, pain, redness, ulcers, nipple discharge, and thickening of the skin of the breast. The phases of delay were defined as follows:
Patient delay was defined as the interval between first detection of a symptom and the time of first presentation to a general practitioner, or any health professional
Physicians delay was defined as the interval between the time of first presentation to the general practitioner or health care providers and onward referral to a hospital
Referral delay was defined as the interval between the time of presentation at a general practitioner's or health care provider and the time of commencement of investigation and therapy at special care center. Delay of <3 months was not considered for this study.
The patients were asked to recall the time they first noticed their symptoms and when they decided to seek medical advice. In addition, they were asked to recall the time it took for a referral to be made to the special care center. Any radiological, laboratory, and referral reports available with the patients were examined and considered as part of the interview as these data helped to resolve any conflicting dates of events. Detailed questions concerning the causes of delay of the diagnosis of BC were asked as well. In addition, the patients were informed of the aim of the study prior to the interview. The outcomes of these questions were then reported.
The data were collected for this study during the time of admission to our hospital as part of the review of patients’ history and clinical examination, or during follow-up of patients at our oncology outpatients department. All patients in this study gave verbal consent. None of the patients refused to participate in the interview.
Fisher's exact test was performed to examine whether there was a significant difference between PABC and non-PABC symptoms and signs at the time of presentation, as well as reasons for the delay in the diagnosis of BC. The significant level was determined at 5%.
RESULTS
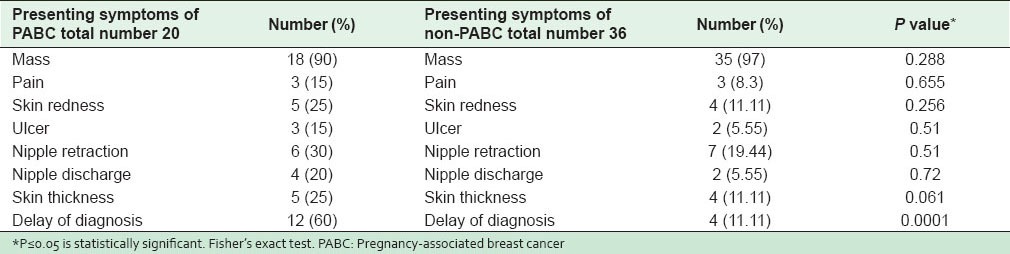
The demographic characteristics of the study population (n = 20 PABC and n = 36 non-PABC) are shown in Table 1. Eighty percent of patients with PABC and 83% of patients with non-PABC were Saudi. Of the patients with PABC, 60% had breast carcinoma during pregnancy, and 40% had BC postpartum. The main symptom of patients with PABC and non-PABC was the discovery of the breast lump, 90% and 97%, respectively, as shown in Table 2. The rest of the symptoms like pain, skin redness, ulcer, nipple retraction, nipple discharge, and skin thickening were more common in patients with PABC compared with patients with non-PABC; (15% vs. 8.3%, 25% vs. 11.11%, 15% vs. 5.5%, 30% vs. 19.44%, 20% vs. 5.5%, and 25% vs. 11.11%, respectively). Sixty percent of patients with PABC had delayed diagnosis compared with only 11.11% of patients with non-PABC.
Table 1.
Demographic characteristics of PABC and BC without pregnancy
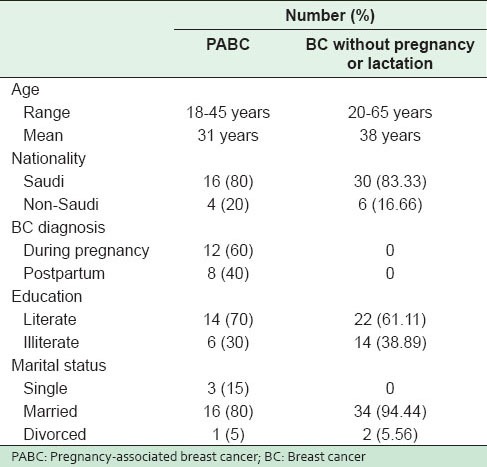
Table 2.
Clinical presentation of PABC and breast carcinoma without pregnancy
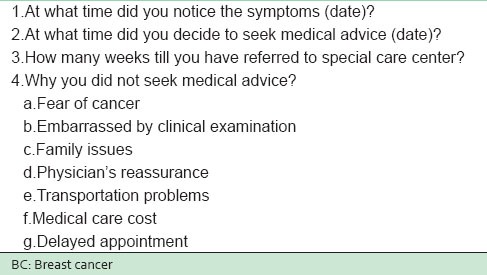
The questions and the responses of BC patients regarding the delay of diagnosis and the causes of the delay during the interview are shown in Table 3.
Table 3.
Questions to be answered by BC patients during interview
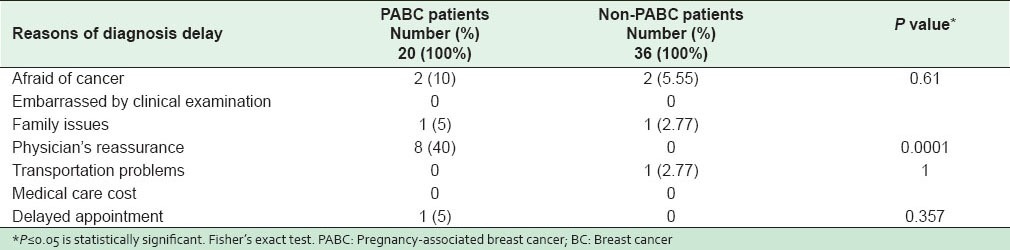
Of the patients with PABC, who had delayed diagnosis, 40% of the delay was due to the reassurance by physicians. No delay of diagnosis was reported by patients with non-PABC. Furthermore, the other causes of delayed diagnosis like fear of cancer, family issues, and long delay in getting an appointment were more common in patients with PABC compared to non-PABC patients, 10% versus 5.55%, 5% versus. 2.77% and 5% versus 0%, respectively. Problems with transportation were more common with patients with non-PABC than patients with PABC, 2.77% versus 0% as shown in Table 4.
Table 4.
Reasons of BC diagnosis delay
DISCUSSION
Our study found that the main presenting symptom of patients with BC was breast mass (lump), and 90% or more of PABC and non-PABC had a breast lump either by itself or in association with other symptoms. According to the Merck Manual of diagnosis and therapy, >80% of BC are discovered when a woman feels a lump herself. Furthermore, most patients with PABC present with painless masses, 90% of which are detected by self-examination.[14]
The physiologic changes that occur in the breast during pregnancy and lactation leading to ductal and lobular proliferation, which alter breast structure resulting in enlargement, increased nodularity and temperature, firmness, nearly doubled breast size, and increased susceptibility to infections can partly obscure the symptoms of BC.[15,16]
In our study, pain, skin thickness, ulcer, nipple retraction and discharge, and skin redness were more than double in patients with PABC compared to non-PABC patients, which can partly be explained by the physiologic changes that occur during pregnancy and lactation.
Because of these changes both the physicians and patients sometimes assume that the density, nipple retraction, redness, skin thickness, discharge or even breast mass are a normal part of pregnancy and lactation. This unfortunately leads to misapprehension of the situation and the reluctance on the part of the physicians to undertake invasive diagnostic procedures.
It is very important that all breast complaints and symptoms, especially those not resolving within 4 weeks, whether associated with gestation or not, are evaluated aggressively to document the nature of the symptoms so that BC can be excluded or treated.[17,18,19]
The strength of our study was the direct personal interviews with our BC patients regarding the date of the onset of symptoms and the date of the first consultation. The use of radiological, laboratory and referral report, when available, were probably more reliable and made our findings more accurate than data-based hospital records. In addition, a delay of <3 months was not considered for this study to minimize the estimates of duration of symptoms, and avoid false reporting or faulty recall by the BC patients. However, the retrospective nature of the data collection on the duration of symptoms poses a potential bias to the validity of these findings. Besides, the sample size of our study was small.
Delay in diagnosing BC is common.[20,21,22] Many studies in developed countries have reported 4–54% frequency in the delay of BC diagnosis of >3 months prior to the initiation of investigation and therapy of women with BC in hospital.[14,23,24,25] In developing countries, the reported frequency of diagnosis delay of >3 months was 72.6% of patients with BC.[26]
Often the diagnosis of PABC is delayed because neither the patient nor the physician suspects malignancy.[27,28]
In our study, 60% of the delay in the diagnosis of patients with PABC was due to false assurance. However, in comparison, non-PABC patients did not report any diagnosis delay. Two patients in each group were afraid of cancer, so they did not seek medical advice themselves. This accounts for 10% of PABC patients and 5.55% of non-PABC patients whose diagnoses were delayed. One patient, 5% of PABC was not able to go to the hospital and seek medical advice because she had to take care of her children attending school. One patient, 2.77% of the non-PABC patients were unable to go to the hospital because of the lack of transportation and inability to pay for it. Whether the pregnancy itself negatively affects survival remains debatable. However, the results of a recent study showed similar overall survival for patients diagnosed with PABC compared with nonpregnant patients.[29] In our study, the fear of cancer, distance to the hospital and family issues still played a role in delaying the diagnosis of BC. Other studies have reported similar findings.[30,31]
In summary, this study showed that >90% of both patients with PABC and non-PABC presenting with a breast mass discovered it themselves. However, in patients with PABC, other symptoms of BC were more common, which could have obscured and delayed the diagnosis. Therefore, the delayed diagnosis of BC is common in patients with PABC compared to patients with non-PABC. The delays are mainly caused by an underestimation of BC symptoms during pregnancy and lactation. Therefore, an increased awareness of clinicians may help reduce the delay in the diagnosis of women with PABC. This would help to reduce the misreading of symptoms and assurance of patients complaining of breast symptoms and the consequent delays in diagnosis and treatment.
ACKNOWLEDGMENT
We would like to extend our sincere gratitude to our statistician, Nithya Jayaseeli, MSc, for her valuable contribution and revision of the statistical analysis.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Bazarbashi S, Al-Zahrani A. Saudi Cancer Registry: Riyadh; 2008. Cancer Incidence Report Saudi Arabia. [Google Scholar]
- 2.Najjar H, Easson A. Age at diagnosis of breast cancer in Arab nations. Int J Surg. 2010;8:448–52. doi: 10.1016/j.ijsu.2010.05.012. [DOI] [PubMed] [Google Scholar]
- 3.Donegan WL. Cancer and pregnancy. CA Cancer J Clin. 1983;33:194–214. doi: 10.3322/canjclin.33.4.194. [DOI] [PubMed] [Google Scholar]
- 4.Fiorica JV. Special problems. Breast cancer and pregnancy. Obstet Gynecol Clin North Am. 1994;21:721–32. [PubMed] [Google Scholar]
- 5.Meshikhes AW, Al-Mubarek MA, Al-Tufaif AA. Breast cancer during pregnancy and lactation. Saudi Med J. 2004;25:531–2. [PubMed] [Google Scholar]
- 6.Antonelli NM, Dotters DJ, Katz VL, Kuller JA. Cancer in pregnancy: A review of the literature. Part I. Obstet Gynecol Surv. 1996;51:125–34. doi: 10.1097/00006254-199602000-00022. [DOI] [PubMed] [Google Scholar]
- 7.Gemignani ML, Petrek JA. Breast cancer during pregnancy: Diagnostic and therapeutic dilemmas. Adv Surg. 2000;34:273–86. [PubMed] [Google Scholar]
- 8.Woo JC, Yu T, Hurd TC. Breast cancer in pregnancy: A literature review. Arch Surg. 2003;138:91–8. doi: 10.1001/archsurg.138.1.91. [DOI] [PubMed] [Google Scholar]
- 9.Borges VF, Schedin PJ. Pregnancy-associated breast cancer: An entity needing refinement of the definition. Cancer. 2012;118:3226–8. doi: 10.1002/cncr.26643. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Richards MA, Westcombe AM, Love SB, Littlejohns P, Ramirez AJ. Influence of delay on survival in patients with breast cancer: A systematic review. Lancet. 1999;353:1119–26. doi: 10.1016/s0140-6736(99)02143-1. [DOI] [PubMed] [Google Scholar]
- 11.Burgess CC, Ramirez AJ, Richards MA, Love SB. Who and what influences delayed presentation in breast cancer? Br J Cancer. 1998;77:1343–8. doi: 10.1038/bjc.1998.224. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Eedarapalli P, Jain S. Breast cancer in pregnancy. J Obstet Gynaecol. 2006;26:1–4. doi: 10.1080/01443610500363808. [DOI] [PubMed] [Google Scholar]
- 13.Facione NC. Delay versus help seeking for breast cancer symptoms: A critical review of the literature on patient and provider delay. Soc Sci Med. 1993;36:1521–34. doi: 10.1016/0277-9536(93)90340-a. [DOI] [PubMed] [Google Scholar]
- 14.Pavlidis NA. Coexistence of pregnancy and malignancy. Oncologist. 2002;7:279–87. [PubMed] [Google Scholar]
- 15.Moore HC, Foster RS., Jr Breast cancer and pregnancy. Semin Oncol. 2000;27:646–53. [PubMed] [Google Scholar]
- 16.Tabbarah HJ. Cancer and pregnancy. In: Haskell CM, editor. Cancer Treatment. Philadelphia: WB Saunders; 2001. pp. 425–34. [Google Scholar]
- 17.Taylor D, Lazberger J, Ives A, Wylie E, Saunders C. Reducing delay in the diagnosis of pregnancy-associated breast cancer: How imaging can help us. J Med Imaging Radiat Oncol. 2011;55:33–42. doi: 10.1111/j.1754-9485.2010.02227.x. [DOI] [PubMed] [Google Scholar]
- 18.Ulery M, Carter L, McFarlin BL, Giurgescu C. Pregnancy-associated breast cancer: Significance of early detection. J Midwifery Womens Health. 2009;54:357–63. doi: 10.1016/j.jmwh.2008.12.007. [DOI] [PubMed] [Google Scholar]
- 19.Litton JK, Theriault RL, Gonzalez-Angulo AM. Breast cancer diagnosis during pregnancy. Womens Health (Lond Engl) 2009;5:243–9. doi: 10.2217/whe.09.2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Tartter PI, Pace D, Frost M, Bernstein JL. Delay in diagnosis of breast cancer. Ann Surg. 1999;229:91–6. doi: 10.1097/00000658-199901000-00012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Azim HA, Jr, Santoro L, Russell-Edu W, Pentheroudakis G, Pavlidis N, Peccatori FA. Prognosis of pregnancy-associated breast cancer: A meta-analysis of 30 studies. Cancer Treat Rev. 2012;38:834–42. doi: 10.1016/j.ctrv.2012.06.004. [DOI] [PubMed] [Google Scholar]
- 22.Loibl S, Han SN, von Minckwitz G, Bontenbal M, Ring A, Giermek J, et al. Treatment of breast cancer during pregnancy: An observational study. Lancet Oncol. 2012;13:887–96. doi: 10.1016/S1470-2045(12)70261-9. [DOI] [PubMed] [Google Scholar]
- 23.Arndt V, Stürmer T, Stegmaier C, Ziegler H, Dhom G, Brenner H. Patient delay and stage of diagnosis among breast cancer patients in Germany-A population based study. Br J Cancer. 2002;86:1034–40. doi: 10.1038/sj.bjc.6600209. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Velikova G, Booth L, Johnston C, Forman D, Selby P. Breast cancer outcomes in South Asian population of West Yorkshire. Br J Cancer. 2004;90:1926–32. doi: 10.1038/sj.bjc.6601795. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Montella M, Crispo A, D’Aiuto G, De Marco M, de Bellis G, Fabbrocini G, et al. Determinant factors for diagnostic delay in operable breast cancer patients. Eur J Cancer Prev. 2001;10:53–9. doi: 10.1097/00008469-200102000-00006. [DOI] [PubMed] [Google Scholar]
- 26.Norsa’adah B, Rampal KG, Rahmah MA, Naing NN, Biswal BM. Diagnosis delay of breast cancer and its associated factors in Malaysian women. BMC Cancer. 2011;11:141. doi: 10.1186/1471-2407-11-141. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Jenner DC, Middleton A, Webb WM, Oommen R, Bates T. In-hospital delay in the diagnosis of breast cancer. Br J Surg. 2000;87:914–9. doi: 10.1046/j.1365-2168.2000.01460.x. [DOI] [PubMed] [Google Scholar]
- 28.Goodson WH, 3rd, Moore DH., 2nd Causes of physician delay in the diagnosis of breast cancer. Arch Intern Med. 2002;162:1343–8. doi: 10.1001/archinte.162.12.1343. [DOI] [PubMed] [Google Scholar]
- 29.Amant F, von Minckwitz G, Han SN, Bontenbal M, Ring AE, Giermek J, et al. Prognosis of women with primary breast cancer diagnosed during pregnancy: Results from an international collaborative study. J Clin Oncol. 2013;31:2532–9. doi: 10.1200/JCO.2012.45.6335. [DOI] [PubMed] [Google Scholar]
- 30.Richardson JL, Langholz B, Bernstein L, Burciaga C, Danley K, Ross RK. Stage and delay in breast cancer diagnosis by race, socioeconomic status, age and year. Br J Cancer. 1992;65:922–6. doi: 10.1038/bjc.1992.193. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Bish A, Ramirez A, Burgess C, Hunter M. Understanding why women delay in seeking help for breast cancer symptoms. J Psychosom Res. 2005;58:321–6. doi: 10.1016/j.jpsychores.2004.10.007. [DOI] [PubMed] [Google Scholar]