

Abstract
Purpose.
Proliferative vitreoretinopathy (PVR) is the most common cause of poor visual outcomes in association with retinal detachment surgeries and ocular trauma. Daunorubicin (DNR) has shown the strongest efficacy in proliferation inhibition in vitro. However, clinical studies have shown only mild effect owing to limitations of narrow therapeutic window and short vitreous half-life.
Methods.
Three milligrams of DNR-loaded particles were intravitreally injected into 18 pigmented rabbits, and vitreous samples were collected up to 84 days for analysis. Thirty-seven rabbits were used for a dose-escalation (1, 3, 6 mg) safety and efficacy study in a rabbit PVR model using a pretreatment design.
Results.
Loading efficiency of DNR was 108.55 ± 12 μg per 1 mg particles. Eighty-four days of follow-up did not reveal any adverse reaction. Pharmacokinetic analysis demonstrated a vitreous half-life of 29 days with a maximum DNR concentration of 178 ng/mL and a minimum concentration of 29 ng/mL at day 84. Daunorubicin-loaded porous silicon (pSi) particles were dosed 8 to 9 weeks before PVR induction, and PVR severity score was dose dependent (Spearman ρ = −0.25, P = 0.0005). Proliferative vitreoretinopathy with tractional retinal detachment was 88% in the control group, 63% in the low-dose group, 14% in the medium-dose group, and 0% in the high-dose group (Cochran-Armitage Trend Test, Z = 8.99, ρ = −0.67, P < 0.0001).
Conclusions.
Daunorubicin-loaded pSi particles can safely reside in the vitreous for at least 3 months. The pSi-based delivery expanded the therapeutic window of DNR by a factor of 862 and drove down the minimum effective concentration by a factor of 175.
Keywords: intravitreal drug delivery, porous silicon, antiproliferative effects, daunorubicin, pharmacodynamics
This porous silicon–based intravitreal delivery system prolonged daunorubicin vitreous half-life from a few hours to 29 days and expanded its therapeutic window 862 times, which may revive this drug application for unwanted scarring at vitreoretinal interface.
Proliferative vitreoretinopathy (PVR) is the most common cause of poor visual outcomes in association with retinal detachment (RD) surgery and ocular trauma despite extensive advances in vitreoretinal surgical technique.1 Direct delivery of drug to the posterior segment by intravitreal injection or intravitreal implant has demonstrated benefits in treating both vitreoretinal diseases2 and experimental PVR models.1,3 It has been suggested that PVR can be prevented by inhibiting cell growth at the cell proliferation stage, which can last for approximately 6 weeks.4 Although various antiproliferative agents could be candidates for the treatment of PVR, their half-lives in the vitreous are too short (e.g., daunorubicin [DNR], 131 minutes; and 5-fluorouracil, 20 minutes).5–7 Of those anti-PVR compounds investigated, DNR has shown the strongest efficacy.8
Owing to the narrow therapeutic window and short biological half-life in the vitreous cavity, intravitreal slow-release systems for extended drug delivery are necessary to maintain therapeutic drug levels at the disease site for longer. To meet this need, various delivery systems have been explored, such as liposomes, nanoparticles, and implantable devices. For liposomes, vitreous clarity decreases with increasing dose.9 Intravitreal injection of nanoparticles can trigger a macrophage reaction and associated vitritis.10,11 Implants involve an invasive procedure that increases the risk of developing RD, lens damage, and vitreous hemorrhage.11
We have been focusing on developing a long-lasting intravitreal drug delivery system.1,12,13 Recently, we have characterized a porous silicon (pSi)–based intravitreal drug delivery system.14,15 In these studies, we demonstrate that DNR can be covalently loaded into oxidized pSi microparticles and safely reside in rabbit vitreous for 2 to 3 months with good ocular tolerability.14 In the initial DNR loading and release study, the level of free DNR in the rabbit vitreous after 2 weeks is very low. To overcome this limitation, we engineered the pore size of the pSi and enhanced the release rate at 2 weeks from 1.05 to 66.52 ng/mL.15
Although DNR has been used for clinical and experimental treatment of PVR,7 simultaneous pharmacodynamics study with a sustained delivery system is very rare. An intravitreal bolus injection of 5 μg free DNR is the highest tolerated dose reported.16 The therapeutic window following such a single intravitreal injection is so narrow that the therapeutic concentration of the drug can be maintained for only 4 hours.17 The current study's aim was to evaluate a sustained pSi-based intravitreal DNR delivery system in a PVR rabbit eye model. We hypothesize that the minimum therapeutic concentration for a drug becomes lower when the time of drug exposure to the target tissue increases, which could be achieved by using a sustained-release system. Previous reports also suggest that inhibitory drug concentration decreases with increasing time of contact between drug and proliferating cells in vitro.18
Materials and Methods
Synthesis of pSi Microparticles
Porous silicon microparticles were prepared by anodic electrochemical etching of highly doped, (100)-oriented, p-type silicon wafers (boron doped, 1.01 ± 0.02 mΩ·cm resistivity; Siltronix, Inc., Archamps, France), as previously described.15 A strip of aluminum foil was attached to the backside of a silicon wafer with an exposed area of 8.04 cm2 and then mounted in a Teflon etching cell that was fitted with a platinum counter electrode. Particles were etched in a 1:1 (v/v) solution of 48% aqueous hydrofluoric acid (HF) and absolute ethanol (Fisher-Scientific, Pittsburg, PA, USA). The wafers were etched at a constant current density (70 mA/cm2) for 400 seconds, and the porous layer resulting from each etch was removed from the silicon substrate by electropolishing in a 1:29 solution of 48% aqueous HF and absolute ethanol for 120 seconds. The etching and electropolishing procedure was repeated 20 times per wafer. The films were harvested every four etches and the resulting porous layers were ultrasonicated in ethanol (FS5 dual-action ultrasonic cleaner; Thermo Fisher Scientific, Pittsburg, PA, USA) for 30 minutes to form the pSi particles. After ultrasonic treatment, the supernatant was removed and the particles were resuspended in ethanol. This procedure was repeated a total of three times until the supernatant was transparent. The pSi particles were isolated, dried at room temperature, and stored under vacuum in a desiccator.
Average particle and pore size of the pSiO2 particles were determined from scanning electron microscope (SEM) plan-view images from randomly selected particles (n > 5) by using a Phillips XL30 field emission electron microscope operating at an accelerating voltage of 5 kV (FEI Phillips, Hillsboro, OR, USA). The particle thickness and open porosity were calculated by optical measurements of the reflectivity spectrum as a function of liquid infiltration by using the spectroscopy liquid infiltration method (SLIM).19
Daunorubicin Loading Into Porous Silica (pSiO2) Microparticles
Daunorubicin was loaded into particles by covalent attachment by creating a chemical bond between the drug and functional groups placed on the particle surface, as previously described.15 Briefly, pSi particles were heated from room temperature to 800°C inside a muffle furnace (Thermo Fisher Scientific), and maintained at 800°C for 1 hour to obtain full oxidization. The resulting pSiO2 particles were then treated with an aqueous HCl solution (2% concentrated HCl by volume) for 1 hour, rinsed three times with water, and dried. The particles were then vortexed in 1% 3-aminopropyltrimethoxysilane (Sigma-Aldrich Corp., St. Louis, MO, USA) in ethanol solution for 1 hour, rinsed with ethanol and dried, resulting in alkylamine-modified particles. The amine-functionalized porous SiO2 particles were reacted with 0.1 M succinic anhydride (99%; Sigma-Aldrich Corp.) in N,N-dimethylformamide (Sigma-Aldrich) for 16 to 17 hours and rinsed with water to obtain a carboxylic acid functional surface (pSiO2-CO2H).14 The surface carboxyl species were then activated by treatment with an aqueous solution containing 68 mM N-(3-dimethylaminopropyl)-N′-ethylcarbodiimide hydrochloride (8.45 mg; Sigma-Aldrich Corp.) and 6.5 mM N-hydroxysulfosuccinimide (0.92 mg, Sulfo-NHS; Pierce Biotechnology, Inc., Rockford, IL, USA). The coupling reagents were added to a dispersion of pSiO2-CO2H particles in aqueous phosphate-buffered saline (PBS, pH 7.4; Fisher Scientific) containing 10% dimethyl sulfoxide (Alfa Aesar, Ward Hill, MA, USA) by volume. Daunorubicin was then coupled to the activated surface by addition of an aqueous solution (400 μL) containing 1 mg/mL DNR hydrochloride (Tocris Biosciences, Bristol, UK) to the particle mixture. After the loading procedure, the particles were pelleted by centrifugation and rinsed with ethanol five times until the washing solution was transparent in order to remove unloaded drug and any excess cross-linkers.
The presence of the functional linker on the pSiO2-CO2H surface, as well as the successful covalent attachment of DNR to the microparticles, was confirmed by attenuated total reflectance Fourier transform infrared (ATR-FTIR) spectroscopy using a Nicolet 6700 FT-IR spectrometer with Smart-ATR attachment (Nicolet Instruments, Inc., Madison, WI, USA). Drug-loading efficiency of DNR pSiO2-COO-DNR was analyzed by thermogravimetry (TGA) as described before.15 The pSiO2-COO-DNR samples (3–5 mg) were placed in a zirconia ceramic crucible. Samples were heated at a constant rate of 10 deg C/min up to 800°C in nitrogen atmosphere with a purge rate of 10 mL/min by using a Q600 simultaneous TGA/differential scanning calorimetry (DSC) apparatus (TA Instruments, New Castle, DE, USA). Weight percent loading efficiency of DNR in the samples was determined by analyzing TGA curves of pSiO2-CO2H (pSiO2 with carboxylic acid functional surface) as well as pSiO2-COO-DNR (pSiO2 containing DNR covalently attached to the pore walls).
In Vivo Pharmacokinetic Study
Eighteen New Zealand Red rabbits were used to study the intraocular pharmacokinetics of pSiO2-COO-DNR particles. All animal studies were performed according to the ARVO Statement for the Use of Animals in Ophthalmic and Vision Research, and the protocols were approved by the Institutional Animal Care and Use Committee of the University of California, San Diego. Only one eye of each animal was used for pSiO2-COO-DNR intravitreal injection. For the intravitreal injection procedure, the rabbits were anesthetized with subcutaneous injections of 25 mg/kg ketamine (Fort Dodge Animal Health, Fort Dodge, IA, USA) and 5 mg/kg xylazine (Akorn, Inc., Decatur, IL, USA). Slit lamp and indirect ophthalmoscopy were performed on all animal eyes before injection. Baseline fundus images were recorded with a digital camera (Canon T2i; Canon, Inc., Tokyo, Japan) with the following settings: F-stop, f/16; exposure time, 1/20 second; ISO, auto, no flash. After eye disinfection preparations, pSiO2-COO-DNR particles suspended in 150 μL sterile balanced salt solution were injected into the mid vitreous cavity of the right eyes with a 1-mL syringe and 27-gauge ½-inch needle under direct view of a surgical microscope after a paracentesis to remove 80 μL aqueous humor. Considering the inherent variation of pSi suspension, after injection, leftover particles in tubes and syringes corresponding to each rabbit were carefully collected, rinsed with deionized water, dried in vacuum, and weighed for mass balance. The eyes were examined at days 1, 7, 21, 35, 56, and 84 after injection by using slit lamp biomicroscopy, a handheld tonometer (Tonopen; Medtronic, Jacksonville, FL, USA) for IOP, and indirect ophthalmoscopy. Color fundus photographs were taken at each examination. Three rabbits were killed at each time point. Afterward, eye globes were enucleated and dissected. After the cornea and lens were removed, the vitreous was sampled by using a 3-mL syringe as we have described previously.15 Whole vitreous was centrifuged for 15 minutes at 14674g, and vitreous supernatant was subjected to HPLC/MS/MS analysis as we have described previously.15 Briefly, the chromatographic separation was performed on a Shiseido Capcell Pak MG III C-18 column (2.0-mm ID × 50-mm length, 3 μm) with a guard column. Mobile phase A was 2.5% by volume methanol (HPLC-grade; Sigma Aldrich Corp.) in water with 0.1% formic acid (Sigma-Aldrich Corp.). Pure methanol with 0.1% formic acid by volume was used as mobile phase B. The liquid chromatography electrospray ionization (LC-ESI)-MS/MS was operated under selected reaction monitoring scan mode to detect DNR and the spiked internal standard doxorubicin (Fisher Bioreagents, Inc., Pittsburg, PA, USA). An LC-ESI-MS/MS run of normal rabbit vitreous supernatant was used as a blank control.
Efficacy Study Design and PVR Induction
For this efficacy study, our goal was to test how long the therapeutic DNR level can be sustained in the vitreous by showing its effect on a PVR model. Therefore, DNR-loaded pSi particles or empty pSi particles (as control) were injected into the rabbit vitreous 8 weeks before the induction of PRV. Thirty-seven New Zealand Red rabbits were used for PVR induction and test of clinical efficacy of pSiO2-COO-DNR particles. Only one eye of each animal was used. Eyes of 27 rabbits were injected with pSiO2-COO-DNR and used as the treatment group, while the other eight rabbits were injected with empty pSi particles and used as a control group. In addition, three rabbits had a partial gas compression vitrectomy and were used as additional control. For the pSiO2-COO-DNR injection, three doses (6, 3, and 1 mg) were tested. For the eight control rabbits, 2 to 6 mg empty pSi particles were injected to match the dose of pSi in the treatment group. For the partial gas vitrectomy, 0.1 mL perfluoropropane gas was injected into the mid vitreous cavity of the right eyes of three rabbits by using a 1-mL luer lock syringe with an air filter and 27-gauge ½-inch needle under direct view of a surgical microscope. No gas-liquid exchange was performed. Mass balance was performed for each pSi particle injection. After the intravitreal injection, clinical examinations were performed every 2 weeks and electroretinogram (ERG) was performed at days 14, 42, and 56. Eight or 9 weeks after microparticle injection, primary homologous rabbit retinal pigment epithelium (RPE) cells were intravitreally injected to induce PVR (four rabbits in high-dose group were injected 9 weeks after pSiO2-COO-DNR injection).20 For the cell injection, approximately 0.1 mL aqueous humor was removed by anterior chamber paracentesis before the intravitreal cell injection. Rabbit primary RPE cells (passage 2) were trypsinized and centrifuged. After the cell viability was confirmed by the trypan blue exclusion test, cells were resuspended in sterile PBS with a final concentration of 2.5 × 106 cell/mL. Each rabbit eye received 0.1 mL primary RPE suspension injected slowly into the vitreous cavity next to the optic disc under direct view of a surgical microscope by using a 0.3-mL insulin syringe with 30-gauge ½-inch needle. After the cell injection, the fundus of each rabbit was examined on days 3, 7, 14, 21, and 28 by two ophthalmologists, and color fundus photos were taken at each examination. Two grading systems were used to score the severity of PVR.21,22 Grading system 121 consists of stage 0: normal retina; stage 1: surface wrinkling (the retina shows an irregular surface of the medullary wings or visual streaks with a beaten metal appearance); stage 2: mild pucker (single or multiple small focal nonelevated contractions resulting in slight displacement of vessels toward the center are observed); stage 3: severe pucker (the preretinal contraction involves the whole area of the wing[s] and may consist of a single pucker or multiple puckers; the retina may be tented up but not by vitreous strands); stage 4: elevated pucker (anterior–posterior traction is observed, with the pucker[s] becoming elevated by vitreous strands); stage 5: partial RD (detachment of the medullary wing occurs but involves only one wing; RD is seen with or without vitreous strands); stage 6: low detachment (RD involves both medullary wings, but the remainder of the avascular retina is attached); and stage 7: total detachment (RD is seen over most of the avascular retina, usually with an appearance of a closed funnel detachment; retinal holes and neovascularization are visible). Grading system 222 includes Fastenberg's classification stage 1: intravitreal membrane; stage 2: focal traction, localized vascular changes including hyperemia, engorgement, dilatation, or blood vessel elevation; stage 3: localized detachment of medullar ray; stage 4: extensive RD, total medullar ray detachment, peripapillary RD; and stage 5: total RD, retinal folds and holes. After the 4-week examination, rabbits were killed. Immediately, eye globes were enucleated and put into cold 4% glutaraldehyde. The rabbit eye has only approximately 1-mm width of pars plana23 that is located between 1 to 2 mm from the limbus.24 To avoid introducing artifactual RD, 1-mm holes were made in the sclera at 3 and 9 o'clock, 1 mm behind the limbus, to help fixative penetration. After 48 hours of fixation, the eyeballs were processed for paraffin embedding and hematoxylin-eosin staining.
Statistical Analysis
For the in vivo pharmacokinetic study, free drug concentrations in the vitreous were normalized by the mean of real injected doses determined by mass balance. The drug concentration–time data were analyzed for noncompartmental modeling by using Phoenix WinNonlin 6.3. The ocular safety data from tonometry and ERG were acquired through repeated examination at multiple time points; therefore, generalized estimating equation (GEE) was used within the SAS (version 9.4) environment to compare IOP or ERG b-wave amplitude between drug-dosed eyes and their fellow eyes while adjusting for variable dosing. The distribution of the response variables was checked and ranks were used if not normally distributed. For the analysis of PVR grading, each study eye was graded five times during a 4-week period. Proliferative vitreoretinopathy severity across the dose groups was compared by using GEE with ordinal model for multinomial data, adjusting for examination time. All analyses were performed by using JMP 11 or SAS 9.4 statistical software (SAS Institute, Inc., Cary, NC, USA) and P values smaller than 0.05 were considered to be significant.
Results
Characterization of the Particle Texture
The SEM measurements revealed an average particle width of 15 ± 2 μm, length of 20 ± 5 μm, and average pore size of 95 ± 17 nm. The SLIM measurement indicated the thickness of the microparticles as 13.6 ± 0.36 μm, and the average porosity as 69.8% ± 1.11%.
Drug Loading by Covalent Attachment
Daunorubicin covalent attachment to microparticles was confirmed by FTIR. Characteristic vibrational bands were observed at ∼1719 cm−1 (C = O), ∼1640 cm−1 (amide I), and ∼1556 cm−1 (amide II) (results not shown). The shift in the characteristic vibrational bands associated with amide bonds before and after DNR grafting provided evidence of successful drug loading by covalent attachment.15 The DNR loading efficiency in pSiO2-COO-DNR particles as calculated by TGA was 108.55 ± 12 μg/mg.
Pharmacokinetics in the Rabbit Vitreous
After mass balance calculation, the mean injected dose of pSiO2-COO-DNR for the pharmacokinetics study was 3.75 ± 1.05 mg. During the 84 days of follow-up after the injection, degradation of pSiO2-COO-DNR manifested by a decrease in number of particles and a color shift from deep red to lighter orange as shown in Figure 1. The LC-MS/MS detected that free DNR concentrations were normalized by the mean injected dose; the vitreous free DNR concentration–time curve is demonstrated in Figure 2. After pSiO2-COO-DNR intravitreal injection, free drug in the vitreous had a rise phase within the first week followed by a slow decrease phase encompassing almost 80 days. The maximum drug concentration (Cmax) was 178 ng/mL at day 7 (Tmax) following the injection. The minimum drug concentration was 29 ng/mL detected at the last time point of 84 days. The free drug elimination half-life from vitreous was 29 days (Table).
Figure 1.
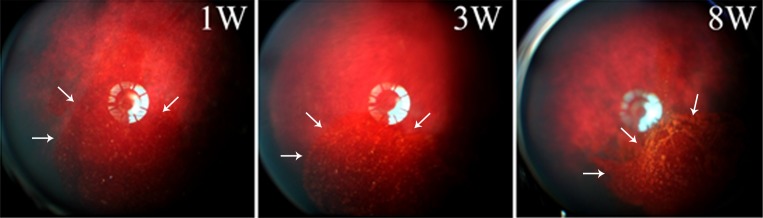
Representative fundus images from one single rabbit showing the color changes of pSiO2-COO-DNR in vitreous from dark red to orange then yellowish, along with DNR release and particle degradation over time.
Figure 2.

Daunorubicin concentration detected by LC-MS/MS in the vitreous supernatant over time. t > MIC indicates DNR concentration in vitreous stayed above the MIC for at least 84 days (observed) and the predicted t > MIC was longer. Each error bar is constructed by using one standard error from the mean. Cmax, maximum concentration detected; MIC, minimum inhibitory concentration; t, time (days).
Table.

Long-Term Ocular Safety of pSiO2-COO-DNR in Rabbit Eyes
In general, no toxicity was observed. The rabbits gained weight normally over the course of the study. The average body weight at intravitreal injection was 3.66 ± 0.49 kg and the average body weight at sacrifice was 4.19 ± 0.48 kg, a gain of 15% within 8 weeks. Gross ocular examination by slit lamp and indirect ophthalmoscope revealed no abnormality. The IOP was measured from both eyes before each scheduled sacrifice time point. The IOP was compared between right eyes and left eyes while adjusting for dose (β = −0.45, P = 0.18). The least squares means for right (drug injected) and left (control) eyes were 12.04 mm Hg (standard error = 0.69) and 11.35 mm Hg (standard error = 0.69), respectively, P = 0.59, n = 32. Electroretinograms, including dark adapted, light adapted, and flicker, were performed before sacrifice or before PVR induction. The b-wave amplitude of each ERG type was compared between the right eye (drug injected) and the left eye (control) in a multivariate regression model, adjusting for drug dose and ERG examination time points. No difference was found between the treated eyes and their fellow eyes (Fig. 3). The drug doses were not significantly associated with ERG b-wave amplitudes (dark adapted: β = 2.72, P = 0.75; light adapted: β = −2.21, P = 0.73; flicker: β = −5.69, P = 0.26). In the later examinations both eyes matured into higher amplitudes (dark adapted: β = 21.71, P < 0.0001; light adapted: β = 15.77, P < 0.0001; flicker: β = 11.31, P < 0.0001).
Figure 3.

Electroretinogram b-wave amplitude (μV) of both the pSiO2-COO-DNR injected eyes and their contralateral eyes. There is no significant difference of b-wave amplitude between the right and left eyes in either type of ERG. dark, dark-adapted ERG; flicker, flicker ERG; light, light-adapted ERG.
Therapeutic Effect of pSiO2-COO-DNR in Rabbit PVR Model
From the mass balance, nine rabbit eyes had a high dose of pSiO2-COO-DNR (dose range, 6.82∼4.77 mg; average, 5.57 mg); seven rabbits eyes had a medium dose (dose range, 3.28∼2.2 mg; average, 2.83 mg); eight rabbits eyes had a low dose (dose range, 1.66∼0.7 mg; average, 1.04 mg); and eight rabbits eyes had empty pSiO2 particles as control (dose range, 7.42∼2.28 mg; average, 4.85 mg). In addition, three rabbits had gas vitrectomy in their right eyes and served as additional control.
After intravitreal RPE cell injection, clinical PVR grading was performed with indirect ophthalmoscope at days 3, 7, 14, 21, and 28. Proliferative vitreoretinopathy severity was dose dependent with a significant negative association between PVR grade and pSiO2-COO-DNR dose (Spearman ρ = −0.25, P = 0.0005; Fig. 4).
Figure 4.

Rabbit PVR severity (grading) over time (4-week period) stratified by the dose groups. From the high- to the low-dose group, PVR severity increases.
Based on Fastenberg's grading, PVRs of grade 3 and above are accompanied by tractional RDs and therefore represent clinically significant PVR. All PVR in eyes with gas vitrectomy was above grade 3, and 88% of eyes with empty pSi had PVR of grade 3 or above (Figs. 5D, 5E). In contrast, no PVR at grade 3 or above was seen in the high-dose group, with only 14% in the medium-dose group (Figs. 5A, 5B); however, 63% PVR at grade 3 and above was seen in the low-dose group (Fig. 5C). After coding the dose levels (0 = both empty pSi and gas vitrectomy controls, 1 = low-dose group, 2 = medium-dose group, and 3 = high-dose group) and dichotomizing the PVR grading by using grade 3, Cochran-Armitage Trend Test showed significant association between PVR of grade 3 and above and the dose levels of DNR (Z = 8.99, P < 0.0001, Spearman correlation = −0.67; Fig. 6).
Figure 5.

Representative images showing the development of PVR following intravitreal injection of primary RPE cells. The images in the same row all come from the same rabbit eye at different time points. (A) High-dose group. (B) Medium-dose group. (C) Low-dose group. (D) Empty pSiO2 control group. (E) Gas control group. Blue arrows indicate cell clumps in the vitreous; black arrows indicate thin membrane in the vitreous; green arrows indicate early retinal elevation caused by traction; and white arrows indicate complete elevation of medullary ray.
Figure 6.

The proportion of PVR accompanying retinal detachment (PVR_RD) increases with decrease of intravitreal dosing of pSiO2-COO-DNR. 0, both empty pSi and gas vitrectomy controls; 1, low-dose group; 2, medium-dose group; 3, high-dose group.
Discussion
Although modern microvitreoretinal surgery to repair RDs has become increasingly safer, retina surgery can still trigger unwanted scarring on or under the retina to form PVR, which fails to allow reattachment or causes redetachment of the retina, resulting in a very poor prognosis of eyesight. Proliferative vitreoretinopathy can develop in approximately 10% of retinal surgery cases and pharmacologic prevention is still an unmet need.25,26 To date, the only clinically effective pharmacologic agent to lessen PVR formation is DNR, which is used in perfusion solution (7.5 μg/mL) for 10 minutes during the vitrectomy.2 Another well-known antiproliferative agent, 5-fluorouracil, has conflicting reports from different clinical trials.27,28 Earlier in vivo preclinical studies have demonstrated that DNR is effective in reducing experimental PVR formation if it is simultaneously injected with the PVR-inducing cells into the vitreous cavity.18,29 Using a macrophage intravitreal injection–induced PVR model, Hui et al.30 have demonstrated that vitreous half-life or sustained drug level in the vitreous is a key factor for inhibiting experimental PVR formation. They have shown that DNR-containing liposomes inhibit PVR better than free drug by 17%. Subsequently, investigators have evaluated sustained DNR release (up to 4 weeks) on experimental PVR in a concurrent mode.31–33 In contrast to these earlier studies, the current study was designed to inject the DNR-loaded delivery system first, then subsequently induce PVR. This strategy allowed us to test the sustainability of the drug delivery system and avoid short-lived drug effect from the initial burst release. The current pharmacokinetic study revealed a very long vitreous half-life for this pSi-based delivery system (29 days). More importantly, the vitreous drug concentration at the last time point (84 days) was still 29 ng/mL, which has been shown to be an effective concentration in a previous study (20 ng/mL).32 On the basis of that study, we waited for 8 weeks after intravitreal injection of the pSi-based delivery system loaded with DNR, because vitreous mean concentration of DNR at day 56 was 33 ng/mL and underwent a very slow tapering to 29 ng/mL at day 86. Indeed, the pretreatment study demonstrated that even the medium-dose group showed significantly less PVR than the controls no matter which PVR grading system is used. The rabbits in the medium-dose group for both the pretreatment study and the pharmacokinetic study received similar intravitreal injection doses (2.83 and 3.75 mg pSiO2-COO-DNR). Compared with the medium-dose group, the low-dose group (receiving 1.66 mg pSiO2-COO-DNR) had significantly more PVR, while the high-dose group (receiving 5.57 mg pSiO2-COO-DNR) had significantly less PVR. These data suggest that the optimal sustained DNR level in the vitreous needed for complete inhibition of PVR formation (IC90) should be approximately 50 ng/mL, which is 1.5 times (5.57 mg/3.75 mg) the level (33 ng/mL) observed in the current pharmacokinetic study at 56 days. This projected vitreous concentration (50 ng/mL) should be approximately the concentration yielded from intravitreal injection of 5.57 mg pSiO2-COO-DNR (high-dose group). In the high-dose group of the current study, no rabbits had PVR severer than Fastenberg's grade 3 (with tractional retinal detachment). The current dose-escalation design and dose-dependent efficacy results, for the first time, allowed us to scientifically project an effective vitreous DNR concentration for inhibiting PVR formation.
The current study also demonstrated that even at high doses, this pSi-based DNR delivery system was well tolerated by the rabbit eyes because both IOP and ERGs were in normal range, as determined by the noninjected fellow eyes. This was largely due to the relatively low DNR vitreous concentration because of slow release from the pSi. Although each milligram of pSi particles contained 108.55 μg DNR, and 5.57 mg particles were injected, the maximum DNR concentration in the vitreous was only 178 ng/mL; this is well below the reported intravitreal toxic dose in the rabbit eye (7.9 μg per eye)34 or the dose used in the irrigation solution for clinical trial (7.5 μg/mL).2 For an intravitreal bolus injection, the therapeutic window or margin of safety is 7.9 μg/4.7 μg or 1.68.34 The current study demonstrated that 108.55 μg DNR in pSi per eye was not toxic, and the effective vitreous concentration was 50 ng/mL or 75 ng/eye (1.5 mL vitreous), which translates into a therapeutic window or margin of safety of 1447. That represents a therapeutic window expansion of 862 times. On the other hand, the slow-release system provided sustained drug levels at the vitreous and retina for a prolonged period, which drove the minimum effective concentration of DNR necessary to inhibit PVR from 4.7 μg intravitreal injection, or 7.5 μg/mL 1-hour intravitreal infusion, to a much lower concentration of 30 to 50 ng/mL for a 4-week presence (from day 56 to 86). This constitutes a 175 times lower minimum effective concentration.
In summary, the current pSi-based DNR delivery system can safely reside in the vitreous and provide therapeutic drug concentrations for at least 3 months. It is very important for a drug delivery system to provide 2 to 3 months of therapeutic drug levels to fight PVR because the risk of PVR formation has a time window of 1 to 4 months after retina injury or surgery.35
Acknowledgments
Supported by the National Institutes of Health (NIH) under Grant NIH EY020617 (LC) and partially by University of California San Diego (UCSD) Vision Research Core Grant P30EY022589. The work was also partially supported by Research to Prevent Blindness, UCSD.
Disclosure: H. Hou, None; K. Huffman, None; S. Rios, None; W.R. Freeman, Spinnaker Biosciences (I, C); M.J. Sailor, Spinnaker Biosciences (I); L. Cheng, Spinnaker Biosciences (I, C)
References
- 1.Cheng L,, Hostetler K,, Valiaeva N,, et al. Intravitreal crystalline drug delivery for intraocular proliferation diseases. Invest Ophthalmol Vis Sci. 2010; 51: 474–481. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Wiedemann P,, Hilgers RD,, Bauer P,, Heimann K.Adjunctive daunorubicin in the treatment of proliferative vitreoretinopathy: results of a multicenter clinical trial: Daunomycin Study Group. Am J Ophthalmol. 1998; 126: 550–559. [DOI] [PubMed] [Google Scholar]
- 3.Berger AS,, Cheng CK,, Pearson PA, et al. Intravitreal sustained release corticosteroid-5-fluoruracil conjugate in the treatment of experimental proliferative vitreoretinopathy. Invest Ophthalmol Vis Sci. 1996; 37: 2318–2325. [PubMed] [Google Scholar]
- 4.Wu EC,, Andrew JS,, Cheng L,, Freeman WR,, Pearson L,, Sailor MJ.Real-time monitoring of sustained drug release using the optical properties of porous silicon photonic crystal particles. Biomaterials. 2011; 32: 1957–1966. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Schmidt Laugesen C,, Steffansen B,, Scherfig E,, la Cour M.Pharmacokinetics of intravitreal 5-fluorouracil prodrugs in silicone oil: experimental studies in pigs. Acta Ophthalmol Scand. 2005; 83: 184–190. [DOI] [PubMed] [Google Scholar]
- 6.Sundaram V,, Barsam A,, Virgili G.Intravitreal low molecular weight heparin and 5-Fluorouracil for the prevention of proliferative vitreoretinopathy following retinal reattachment surgery. Cochrane Database Syst Rev. 2013; 1:CD006421. [DOI] [PubMed]
- 7.Moysidis SN,, Thanos A,, Vavvas DG.Mechanisms of inflammation in proliferative vitreoretinopathy: from bench to bedside. Mediators Inflamm. 2012; 2012: 815937. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Hou J,, Li Y,, Zhou Z, et al. Antiproliferative property of hexadecyloxypropyl 9-[2-(phosphonomethoxy) ethyl] guanine (HDP-PMEG) for unwanted ocular proliferation. Mol Vis. 2011; 17: 627–637. [PMC free article] [PubMed] [Google Scholar]
- 9.Cheng L,, Hostetler KY,, Chaidhawangul S,, et al. Intravitreal toxicology and duration of efficacy of a novel antiviral lipid prodrug of ganciclovir in liposome formulation. Invest Ophthalmol Vis Sci. 2000; 41: 1523–1532. [PubMed] [Google Scholar]
- 10.Harrison J,, Bartlett CA,, Cowin G, et al. In vivo imaging and biodistribution of multimodal polymeric nanoparticles delivered to the optic nerve. Small. 2012; 8: 1579–1589. [DOI] [PubMed] [Google Scholar]
- 11.Wang J,, Jiang A,, Joshi M,, Christoforidis J.Drug delivery implants in the treatment of vitreous inflammation. Mediators Inflamm. 2013; 2013: 780634. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Cheng L,, Hostetler KY,, Lee J, et al. Characterization of a novel intraocular drug-delivery system using crystalline lipid antiviral prodrugs of ganciclovir and cyclic cidofovir. Invest Ophthalmol Vis Sci. 2004; 45: 4138–4144. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Wang H,, Chhablani J,, Freeman WR,, et al. Intraocular safety and pharmacokinetics of hexadecyloxypropyl-cidofovir (HDP-CDV) as a long-lasting intravitreal antiviral drug. Invest Ophthalmol Vis Sci. 2011; 52: 9391–9396. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Chhablani J,, Nieto A,, Hou H, et al. Oxidized porous silicon particles covalently grafted with daunorubicin as a sustained intraocular drug delivery system. Invest Ophthalmol Vis Sci. 2013; 54: 1268–1279. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Hou H,, Nieto A,, Ma F,, Freeman WR,, Sailor MJ,, Cheng L.Tunable sustained intravitreal drug delivery system for daunorubicin using oxidized porous silicon. J Control Release. 2014; 178C: 46–54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Hui YN,, Liang HC,, Cai YS,, Kirchhof B,, Heimann K.Corticosteroids and daunomycin in the prevention of experimental proliferative vitreoretinopathy induced by macrophages. Graefes Arch Clin Exp Ophthalmol. 1993; 231: 109–114. [DOI] [PubMed] [Google Scholar]
- 17.Wiedemann P,, Sorgente N,, Bekhor C,, Patterson R,, Tran T,, Ryan SJ.Daunomycin in the treatment of experimental proliferative vitreoretinopathy: effective doses in vitro and in vivo. Invest Ophthalmol Vis Sci. 1985; 26: 719–725. [PubMed] [Google Scholar]
- 18.Khawly JA,, Saloupis P,, Hatchell DL,, Machemer R.Daunorubicin treatment in a refined experimental model of proliferative vitreoretinopathy. Graefes Arch Clin Exp Ophthalmol. 1991; 229: 464–467. [DOI] [PubMed] [Google Scholar]
- 19.Pacholski C,, Sartor M,, Sailor MJ,, Cunin F,, Miskelly GM.Biosensing using porous silicon double-layer interferometers: reflective interferometric Fourier transform spectroscopy. J Am Chem Soc. 2005; 127: 11636–11645. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Yang CH,, Huang TF,, Liu KR,, Chen MS,, Hung PT.Inhibition of retinal pigment epithelial cell-induced tractional retinal detachment by disintegrins a group of Arg-Gly-Asp-containing peptides from viper venom. Invest Ophthalmol Vis Sci. 1996; 37: 843–854. [PubMed] [Google Scholar]
- 21.Agrawal RN,, He S,, Spee C,, Cui JZ,, Ryan SJ,, Hinton DR.In vivo models of proliferative vitreoretinopathy. Nat Protoc. 2007; 2: 67–77. [DOI] [PubMed] [Google Scholar]
- 22.Fastenberg DM,, Diddie KR,, Dorey K,, Ryan SJ.The role of cellular proliferation in an experimental model of massive periretinal proliferation. Am J Ophthalmol. 1982; 93: 565–572. [DOI] [PubMed] [Google Scholar]
- 23.Funk R,, Rohen JW.SEM studies on the functional morphology of the rabbit ciliary process vasculature. Exp Eye Res. 1987; 45: 579–595. [DOI] [PubMed] [Google Scholar]
- 24.Chen M,, Li X,, Liu J,, Han Y,, Cheng L.Safety and pharmacodynamics of suprachoroidal injection of triamcinolone acetonide as a controlled ocular drug release model. J Control Release. 2015; 203C; 107–117. [DOI] [PubMed] [Google Scholar]
- 25.Charteris DG.Proliferative vitreoretinopathy: pathobiology surgical management, and adjunctive treatment. Br J Ophthalmol. 1995; 79: 953–960. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Scheer S,, Morel C,, Touzeau O,, Sahel JA,, Laroche L.Pharmacological adjuvants for surgical treatment of proliferative vitreoretinopathy [in French]. J Fr Ophtalmol. 2004; 27: 1051–1059. [DOI] [PubMed] [Google Scholar]
- 27.Asaria RHY,, Kon CH,, Bunce C, et al. Adjuvant 5-fluorouracil and heparin prevents proliferative vitreoretinopathy: results from a randomized, double-blind, controlled clinical trial. Ophthalmology. 2001; 108: 1179–1183. [DOI] [PubMed] [Google Scholar]
- 28.Charteris DG,, Aylward GW,, Wong D,, Groenewald C,, Asaria RHY,, Bunce C.A randomized controlled trial of combined 5-fluorouracil and low-molecular-weight heparin in management of established proliferative vitreoretinopathy. Ophthalmology. 2004; 111: 2240–2245. [DOI] [PubMed] [Google Scholar]
- 29.Chen EP,, Steinhorst UH,, Samsa GP,, Saloupis PT,, Hatchell DL.The effect of combined daunorubicin and triamcinolone acetonide treatment on a refined experimental model of proliferative vitreoretinopathy. Invest Ophthalmol Vis Sci. 1992; 33: 2160–2164. [PubMed] [Google Scholar]
- 30.Hui Y-N,, Liang H-C,, Cai Y-S,, Kirchhof B,, Heimann K.Corticosteroids and daunomycin in the prevention of experimental proliferative vitreoretionopathy induced by macrophages. Graefes Arch Clin Exp Ophthalmol. 1993; 231: 109–114. [DOI] [PubMed] [Google Scholar]
- 31.Hashizoe M,, Ogura Y,, Takanashi T,, Kunou N,, Honda Y,, Ikada Y.Implantable biodegradable polymeric device in the treatment of experimental proliferative vitreoretinopathy. Curr Eye Res. 1995; 14: 473–477. [DOI] [PubMed] [Google Scholar]
- 32.Rahimy MH,, Peyman GA,, Fernandes ML,, el-Sayed SH,, Luo Q,, Borhani H.Effects of an intravitreal daunomycin implant on experimental proliferative vitreoretinopathy: simultaneous pharmacokinetic and pharmacodynamic evaluations. J Ocul Pharmacol. 1994; 10: 561–570. [DOI] [PubMed] [Google Scholar]
- 33.Kuo HK,, Chen YH,, Wu PC, et al. Attenuated glial reaction in experimental proliferative vitreoretinopathy treated with liposomal doxorubicin. Invest Ophthalmol Vis Sci. 2012; 53: 3167–3174. [DOI] [PubMed] [Google Scholar]
- 34.Santana M,, Wiedemann P,, Kirmani M,, et al. Daunomycin in the treatment of experimental proliferative vitreoretinopathy: retinal toxicity of intravitreal daunomycin in the rabbit. Graefes Arch Clin Exp Ophthalmol. 1984; 221: 210–213. [DOI] [PubMed] [Google Scholar]
- 35.Mietz H,, Heimann K.Onset and recurrence of proliferative vitreoretinopathy in various vitreoretinal disease. Br J Ophthalmol. 1995; 79: 874–877. [DOI] [PMC free article] [PubMed] [Google Scholar]