

Abstract
Pustular psoriasis is characterized by abrupt onset of macroscopic pustules associated with erythema and symptoms of burning pain and constitutional symptoms. There are several precipitating factors, both physiological such as pregnancy and routinely prescribed drugs like antihypertensives, antifungals, corticosteroids and progesterone. We present a case of a 50-year-old male patient with pustular psoriasis, well controlled on oral methotrexate, who presented with sudden exacerbation of pustular psoriasis following the use of telmisartan. This case is presented due to the absence of prior reports of telmisartan aggravating pustular psoriasis.
Keywords: Angiotensin II receptor blocker, drug induced, hypertension, psoriasis
INTRODUCTION
Pustular psoriasis refers to the forms of psoriasis characterized by macroscopic pustules. It can be either localized or generalized, localized forms tending toward chronicity and generalized forms varying between acute, sub-acute or life-threatening course.[1] Generalized pustular psoriasis is an uncommon variant where the eruption has sterile pustules as its central feature. Its relationship with psoriasis is clear as the patient may have plaque-type psoriasis prior to[2] or after the onset of pustular psoriasis.
There are several documented triggers of pustular psoriasis, the earliest of which was Von Zumbusch's original patient who was provoked by irritating topical therapy (coal tar, anthralin).[3] In addition, physiological states like pregnancy, factors such as infection,[4] hypocalcemia and hypoparathyroidism[5] have also been implicated in its causation. Several drugs have also been reported to cause generalized pustular psoriasis. We present a case of acute generalized pustular psoriasis exacerbated by telmisartan, which is an antihypertensive of the angiotensin II receptor blocker category.[6] To the best of our knowledge, pustular psoriasis due to telmisartan has not been reported so far.
CASE REPORT
A 50-year-old male patient, a known case of pustular psoriasis, well controlled on oral methotrexate presented with sudden exacerbation with fresh crops of pustules. The patient was a known hypertensive on 10mg Amlodipine per day for 4 years. On having a recorded persistently high blood pressure of 160/100 mm Hg even after enforcing strict diet restrictions and exercise, the patient was prescribed telmisartan by his physician.
The patient reviewed with the General Medicine department 2 weeks later with no complaints and normotensive status. However, 1 week later, the patient visited the Dermatology Out-patient Department (OPD) with complaints of severe burning sensation and several new groups of lesions occurring over his arms and legs. On examination, multiple, well-defined, discrete, pin-point pustules [Figure 1] were seen over the bilateral arms, forearms, thighs and lower legs, with involvement of the bilateral axillae as well. The pustules were present over an erythematous base, seen in clusters, more over the flexor surfaces, and the surrounding skin showed multiple, well-defined areas of exfoliation [Figure 2]. The patient was admitted and treated symptomatically and telmisartan was discontinued. A noticeable gradual regression of new lesions and healing of existing lesions was observed within few days of treatment. The resolution was completed by 1 month, following which the asymptomatic patient was discharged with addition of oral prazosin 2.5 mg after which there was neither exacerbation of older lesions nor provocation of new pustules of psoriasis. The patient had a symptom-free period of 6 months after which he was inadvertently prescribed telmisartan by another physician for control of hypertension. Three weeks later, he visited the Dermatology OPD with complaints of similar pustules all over the body, occurring in crops, associated with photosensitivity and severe burning pain over the lesions. On admission and examination, multiple, discrete, pin-point pustules over an erythematous base with crusting over the surface of few pustules were seen over the right thigh, right side of the neck and bilateral axillae. Multiple, discrete, hyperpigmented papules, erythematous erosions with patches of exfoliation were seen over the chest, abdomen, back, arms, forearms and lower legs bilaterally, suggestive of a previous crop of pustules in the recent past. The present episode also responded well to cessation of telmisartan with complete resolution of all symptoms within 1 week. Normotensive status was obtained and maintained with increased dose of prazosin from 2.5 to 5 mg.
Figure 1.

Pustular lesions over the calf
Figure 2.

Generalized pustular eruption with exfoliation over the back
DISCUSSION
Psoriasis is influenced by several environmental and other risk factors such as alcohol, smoking, emotional stress, sunlight, infections and drugs.[1] Generalized pustular psoriasis is the most severe type of psoriasis and is characterized by diffuse erythema, scattering of pustules, high-grade fever and malaise, which were sudden in onset. The pustular form of psoriasis is also triggered by similar factors. However, the drugs provoking pustulation among psoriatics are slightly different and listed below [Table 1].
Table 1.
Drugs provoking pustular psoriasis
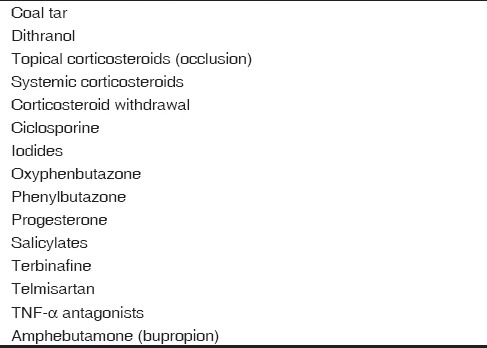
There are innumerable new drugs being discovered and used in various fields of medicine, the effects of which on pustular psoriasis are unknown. The list of drugs triggering the onset of pustular psoriasis is therefore evergrowing, and the most common of these can be easily grouped as PILs to STOP, namely progesterone, iodide, lithium, salicylates, terbinafine, oxyphenbutazone, phenylbutazone and bupropion, used to aid cessation of smoking. The most important trigger however is corticosteroid therapy, which can act via the topical as well as systemic routes and also due to sudden withdrawal of corticosteroids. Cyclosporine withdrawal is also an important precipitant.[1] Losartan, an angiotensin II receptor blocker, has been implicated by Lamba et al., in triggering psoriasis.[7] Another drug, candesartan, belonging to the same class, was reported by Kawamura and Ochiai[8] to induce pustular psoriasis by up-regulation of bradykinin. The effect of the present drug, temisartan, intriggering pustular psoriasis is only yet to be documented. This is of growing concern as telmisartan and other angiotensin II receptor blockers are being used extensively in hypertension and hypertensive heart disease owing to its potent, long-acting nature, selective mechanism of action and considerable safety of use.[9]
Pustular psoriasis provoked by telmisartan can be considered as drug-induced disease as the discontinuation of drug stopped the further progression of disease. This case highlights the fact that treating physicians should be aware of drugs that exacerbate the disease and that caution should be exercised while starting a new drug in patients with pustular psoriasis.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Griffiths CE, Barker JN. Psoriasis. In: Burns T, Breathnach S, Cox N, Griffiths C, editors. Rook's Textbook of Dermatology. 8thed. Vol. 20. London: Blackwell Science; 2012. pp. 44–54. [Google Scholar]
- 2.Johann E, Gudjonsson, Elder JT. Psoriasis. In: Wolff K, Goldsmith LA, Katz SI, Gilchrest BA, Paller AS, Leffell DJ, editors. Fitzpatrick's Dermatology in General Medicine. 8thed. New York: McGraw-Hill; 2012. pp. 211–5. [Google Scholar]
- 3.Von Zumbusch LR. Psoriasis und pustulösesExanthem. Arch Dermatol Syphilol. 1910;99:335–46. [Google Scholar]
- 4.Baker H, Ryan TJ. Generalized pustular psoriasis. Br J Dermatol. 1968;80:771–93. doi: 10.1111/j.1365-2133.1968.tb11947.x. [DOI] [PubMed] [Google Scholar]
- 5.Risum G. Psoriasis exacerbated by hypoparathyroidism with hypocalcaemia. Br J Dermatol. 1973;89:309–12. doi: 10.1111/j.1365-2133.1973.tb02980.x. [DOI] [PubMed] [Google Scholar]
- 6.Matsubara H. Pathophysiological role of angiotensin II type 2 receptor in cardiovascular and renal diseases. Circ Res. 1998;83:1182–91. doi: 10.1161/01.res.83.12.1182. [DOI] [PubMed] [Google Scholar]
- 7.Lamba G, Palaniswamy C, Singh T, Shah D, Lal S, Vinnakota R, et al. Psoriasis Induced by losartan therapy: A case report and review of the literature. Am J Ther. 2011;18:e78–80. doi: 10.1097/MJT.0b013e3181c6c0c2. [DOI] [PubMed] [Google Scholar]
- 8.Kawamura A, Ochiai T. Candesartan cilexetil induced pustular psoriasis. Eur J Dermatol. 2003;13:406–7. [PubMed] [Google Scholar]
- 9.Wienen W, Entzeroth M, van Meel JC, Stangier J, Busch U, Ebner T, et al. A review on telmisartan: A novel, long-acting angiotensin II-receptor antagonist. Cardiovasc Drug Rev. 2000;18:127–54. [Google Scholar]