

Abstract
A medication indication is a valid reason to use medication. Comprehensive information on medication and its intended indications has valuable potential applications for patient treatments, quality improvements, and clinical decision support. Though there are some publicly available medication resources, this medication and indication information is comprised primarily of labeled uses approved by the FDA. Additionally, linking those medications and the corresponding indications is not easy to accomplish. Furthermore, research that analyzes actual medication and indication occurrences used in real clinical practice is limited. In this study, we compiled clinician-asserted medication and indication pairs from a large cohort of Mayo Clinic electronic medical records (EMRs) and normalized them to the standard forms (ie, medication to the RxNorm ingredient and indication to SNOMED-CT). We then analyzed medication and indication occurrences and compared them with the public resource in various ways, including off-label statistics.
Introduction
A medication indication is a valid reason—most often for medical issues such as signs/symptoms or diseases/disorders—to use medication. The patients’ medication history and intended indications are critical information for future medical treatment, improvements in the quality of clinical care and better clinical decision support. The linkage of medication and its intended indications and normalizing them to standard terminologies aid in clinical knowledge management1,2 and play an important role in enabling the secondary use of electronic medical records (EMRs) for clinical and translational research3,4.
A comprehensive medication and indication linkage is not straightforwardly obtained, although some freely available medication resources exist. Those medication indications are primarily labeled indications provided by manufacturers, which are later approved by the FDA. However, off-label medication use (ie, not approved by the FDA) is common in clinical practice. One in five prescribed medications in the U.S. is off-label and is most often employed as for psychiatric medication, and off-label use represents up to 31% of prescribed psychiatric medication5.
There have been studies to aggregate indication information for prescribed medication from the data recorded by clinicians. Bashford et al.6 observed the relation between new prescriptions for proton pump inhibitors and upper gastrointestinal morbidity in a general practitioner database and showed that new prescriptions did not necessarily reflect changes in licensed indications. Walton et al.7 assessed a clinical decision support system based on computerized physician order entry to obtain medication indications and to record medical problems. They examined three medications to alert off-label uses and observed that the system produced less than optimal accuracy. They claimed that this result demonstrated the challenge in obtaining accurate indication information during the prescription process and suggested potential mandates for indication based prescription.
There also have been research efforts to establish a relationship between medication and indication using EMRs and public medication information resources. Burton et al.8 processed 1.6 million EMRs from the Regenstrief Medical Record System to extract medications and diagnoses. They then linked medications and indications using RxNorm, VA National Drug File Reference Terminology (NDF-RT), and SNOMED-CT and produced 24,398 medication-indication pairs. They achieved overall sensitivity of 67.5% and specificity of 86%. Wei et al.9 create a computable resource of medication and indication pairs, called MEDI, compiled from four publicly available medication resources, such as RxNorm, Side Effect Resource 2, MedlinePlus, and Wikipedia. They apply natural language processing and ontologies to extract indications for prescribable medication. They map medications to RxNorm ingredients and indications to the Unified Medical Language System (UMLS) and ICD9 codes. MEDI contains 63,343 medication and indication pairs. The estimated precision and recall are 56% to 94% and 20% to 51%, respectively depending on the resources. However, it should be noted that those medication-indication linkages from the above studies are not based on the clinician-asserted data in EMRs, but, rather, are derived from using known publicly available medication information resources.
Jung et al.10 developed the method to automatically detect off-label medication uses using a machine learner based on various features including drug and disease similarities, known medication usages, and medication-indication co-occurrence statistics in EMRs. They achieved a precision of 0.945, recall of 0.778 and F- score of 0.853 and produced 10,765 potential novel drug-indication pairs with a probability estimate cut-off of 0.95. Li et al.11 determined the reasons for medication uses based on medical conditions in outpatient notes. They first generated the medication indication knowledge database compiled from MicroMedex, NDF-RT and Adverse Event Reporting System, and ranked indications based on the established and frequent uses. Then, they obtained an overlap between medication conditions in EMRs and the medication indication knowledge database, and selected the highest-rank medication-condition pair as the most likely reason for prescribing medication. They achieve an F-measure of 0.739 in the pilot study.
A large-scale study that analyzed diverse medication and indication pairs used in real clinical practice was limited due to technical difficulties in extracting these medications and indications from EMRs and limited access to a large amount of appropriate clinical data. In this study, we compiled medication and indication occurrences from a cohort consisting of 140K patients whose medical home is at Mayo Clinic and normalized them to the standard terminologies (ie, medication to the RxNorm ingredient (IN) and indication to SNOMED-CT). We then analyzed the medication and indication occurrences in various ways, including off-label statistics and also compared them with the public medication indication resource, MEDI.
Backgrounds
This study utilized the medical terminology and ontology to normalize medications and their indications, and the existing tools to extract them. We briefly describe them as follows:
RxNorm
RxNorm is a terminology for normalized medication names developed by the U.S. National Library of Medicine (NLM). It contains the prescription medications and many nonprescription formulations approved for human use. RxNorm uses term types to describe generic and branded names at different levels of specificity and conceptually unique medication descriptions are assigned by a concept unique identifier (RxCUI). RxNorm provides normalized medication names that link to medication variants frequently used in pharmacy management such as First Databank12, Micromedex13, MediSpan14, Gold Standard15, Multum16, and NDF-RT17. Hence, RxNorm enables various systems using different medication terminologies to share and exchange data. RxNorm is becoming part of Meaningful Use to support the expanding functionality of health record technology18.
SNOMED-CT
SNOMED-CT (Systematized Nomenclature of Medicine-Clinical Terms) is a systematically organized collection of medical terminology providing codes, terms, synonyms and definitions used in clinical documentation. SNOMED-CT provides the core general terminology for EMRs. SNOMED CT is one of the standard uses in U.S. Federal Government systems for the electronic exchange of clinical health information. It covers clinical findings, symptoms, diagnoses, procedures, body structures, organisms and other etiologies, substances, pharmaceuticals, devices and specimen (http://www.ihtsdo.org/snomed-ct). It also supports in organizing EMRs by mapping and encoding various medical concepts to the standard for clinical care and research19.
MedXN
MedXN (Medication eXtraction and Normalization) is a UIMA (Unstructured Information Management Architecture) based pipeline to extract medication information and map it to the most specific RxNorm concept20 (http://sourceforge.net/projects/ohnlp/files/MedXN/). MedXN focuses on medication normalization by mapping the comprehensive medication description to the best matching RxCUI using flexible matching, abbreviation expansion, inference, etc. MedXN uses externalized resources (ie, medication dictionary, attribute definitions, and regular expression attribute patterns) to allow a simple customization process for the needs of end users. For medication RxCUI assignment, MedXN produced an F-measure of 0.932. In this study, we used MedXN for normalizing medications (ie, mapping medications to RxNorm).
MedTagger
MedTagger is the open-source pipeline (http://sourceforge.net/projects/ohnlp/files/MedTagger/) that contains a suite of programs including three major components: indexing based on dictionaries, information extraction based on patterns, and machine learning-based named entity recognition21,22. In this study, we used MedTagger’s indexing functionality to map medication indications to SNOMED-CT.
MEDI
MEDI (MEDication Indication) is an open-source computable medication indication resource that is compiled from four publicly available medication resources, such as RxNorm, Side Effect Resource 2, MedlinePlus, and Wikipedia (http://knowledgemap.mc.vanderbilt.edu/research/content/MEDI). In this study, we compared Mayo medication-indication pairs with MEDI (MEDI_01212013_UMLS.csv) that contains 3,112 medications, 4,396 indications, and 53,106 medication-indication pairs. MEDI also contains a maker, ‘possible label use,’ which denotes whether a given indication is highly likely on-label or not. We utilized this information to analyze potential off-label uses in Mayo medication-indication pairs.
Materials and Methods
Data
We use all clinical notes of a cohort consisting of 140K patients whose medical home is at Mayo Clinic. The clinical notes consist of a variety of sections, such as Impression/Report/Plan, Current Medications, History of Present Illness etc., and each section contains specific content. Medication information appears in numerous ways across sections. However, most medication mentions are found in the Current Medication section, which contains medications currently being taken by patients. Therefore, it is the most important section regarding to medication information for patient care. The format of the Current Medication section is much like a grocery list. However, it contains the most diverse medication description patterns23. Some medication entries in the Current Medication section also occur with clinician-asserted indications, followed by “Indication:” or “Indication, Site, Instruction:” (See the example in Figure 1). In this study, we investigated the clinician-asserted medication and indication pairs extracted from the Current Medication section in clinical notes.
Figure 1.
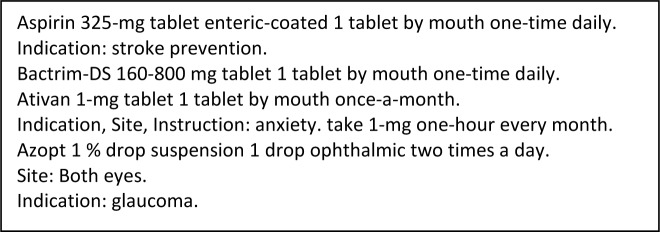
Medication and indication descriptions in the Current Medication section
Medication-indication pair extraction
The MedXN system was employed to extract medications and map them to RxNorm. An indication was extracted using regular expressions in the following ways: (1) extracted strings after ‘Indication:’ and (2) extracted strings after ‘Indication, Site, Instruction:’ In (1) we treated all extracted strings as an indication, but in (2) we selected only the concept classified as ‘disease’ and ‘finding’ in UMLS as an indication because there might be non-indication mentions, such as ‘site’ or ‘instruction’ that are generally not a disease or disorder.
The medication name extracted from MedXN is a generic (ie, ingredient, precise ingredients, multiple ingredients) or brand name (ie, trade name), and an indication is free-text signs/symptoms and disease/disorder expressed in various ways. In order to properly analyze overall medication-indication occurrence statistics, the synonyms of medication names and indications need to be normalized to the standard terminologies.
After we compiled all medication and indication pairs, each medication was mapped to an RxNorm ingredient (IN), and an indication was mapped to a SNOMED-CT concept. A medication name that is not an ingredient (ie, brand name) was mapped to an ingredient using RxNorm relationship (ie, “tradename_of” “has_precise_ingredient” in RXNREL.rrf). We used MedTagger to process free-text indication strings and map them to SNOMED-CT with UMLS CUI.
Finally, we aggregated all normalized indications (SNOMED-CT with UMLS CUI) along with their frequency for a given normalized medication (RxNorm IN with RxCUI) to obtain medication and indication pairs—ie, each indication for a given medication is counted across all clinical notes to obtain the global number of occurrences. Figure 2 shows the overall process employed to obtain medication and indication pairs from clinical notes.
Figure 2.
A workflow to extract medication and indication pairs.
Comparison of Mayo medication-indication with MEDI
We compared the normalized Mayo medication-indication pairs with MEDI (MEDI_01212013_UMLS.csv) to determine to what extent they share the same medication-indication pairs. In MEDI, medication and indication are normalized to RxNorm IN and UMLS CUI, respectively. The normalized indications of the Mayo data are SNOMED-CT concepts that are a part of UMLS and that also have UMLS CUI assigned. Hence, we first found medications that have the same RxNorm IN (ie, RxCUI) and we then checked to see if they shared the same UMLS CUI for an indication.
Medication-indication pair assessment
Various statistics, including numbers of medications/indications/medication-indication pairs, comparisons (ie, match and mismatch) with MEDI, and potential off-label medication indications, have been analyzed. For comparison with MEDI, we used two types of matches—ie, ‘Exact match’ and ‘Flexible match.’ In exact match, if both Mayo’s medication (RxCUI) and the corresponding indication (UMLS CUI) appear in MEDI, we treat them as a ‘match,’ otherwise, we treat them as a ‘mismatch.’ In flexible match, a ‘match’ means that two of indications each in Mayo and MEDI for the same medication are within two steps of navigation in the network where the nodes are the FIND and DISO concepts in the UMLS and the edges are concept relations defined in the UMLS concept relation table (ie, MRREL), otherwise, it is a ‘mismatch.’
For the normalization of indication, we used SNOMED-CT in the UMLS. SNOMED-CT is known to have a fine granularity—ie, the detailed classifications for similar medical concepts although they are semantically the same in general. Since indications in clinical notes generally are not described in such detail or precise manner, this fine granularity classification may cause mismatches when compared with the data that are built from different sources. For this reason, we also investigated the flexible match that may represent more reasonable match statistics.
Results
Mayo medication-indication statistics
Table 1 contains basic statistics delineating Mayo’s medication and indication occurrences. Each column represents the unique number of medications, indications, and medication-indication pairs, respectively. The term ‘Original’ denotes the medication and indication descriptions as they appear in clinical notes. In ‘Normalized,’ medications were mapped to RxNorm ingredients, and indications were mapped to SNOMED-CT. In the normalization process, 434 medications out of 5,128 original medications did not have the ingredient relationship in RxNorm’s RXNREL.rrf and 7,769 indications out of 88,522 original indications were not able to map to SNOMED-CT using our dictionary lookup algorithm. After the normalization process (without considering mismatches), the number of medication, indications, and medication-indication pairs were decreased significantly (to approximately 29%, 6%, and 21% of the original size, respectively)
Table 1.
Mayo medication and indication statistics
| # medications | # indications | # medication-indication pairs | |
|---|---|---|---|
| Original | 5,128 | 88,522 | 140,499 |
| Normalized | 1,494 | 5,066 | 29,823 |
Mayo vs. MEDI medication-indication occurrences
We compared Mayo’s normalized medication and indication occurrences with those of MEDI (MEDI_01212013_UMLS.csv). Since MEDI’s normalization is the same as Mayo’s (ie, MEDI’s medications are normalized to RxNorm ingredient and indications are normalized to UMLS CUI), we were able to identify matches between Mayo’s and MEDI’s medication and indication pairs. Table 2 shows overall matched and mismatched medication-indication pairs between Mayo and MEDI. Mayo’s medication-indication pairs are stratified by the log of the patient-level occurrences. Each row represents the cases that have greater or equal to the log of the number of patients who have a given medication-indication pairs.
Table 2.
Mayo’s medication-indication pairs compared with MEDI.
| log2(#pts) | # total | Exact match | Flexible match | ||
|---|---|---|---|---|---|
| # matches (%) | # mismatches (%) | # matches (%) | # mismatches (%) | ||
| 0 (1) | 29823 | 4347 (15%) | 25476 (85%) | 17285 (58%) | 12538 (42%) |
| 1 (2) | 15677 | 3244 (21%) | 12433 (79%) | 9482 (60%) | 6195 (40%) |
| 2 (4) | 8095 | 2262 (28%) | 5833 (72%) | 5101 (63%) | 2994 (37%) |
| 3 (8) | 4715 | 1601 (34%) | 3114 (66%) | 3084 (65%) | 1631 (35%) |
| 4 (16) | 2850 | 1108 (39%) | 1742 (61%) | 1911 (67%) | 939 (33%) |
| 5 (32) | 1710 | 712 (42%) | 998 (58%) | 1159 (68%) | 551 (32%) |
| 6 (64) | 997 | 452 (45%) | 545 (55%) | 675 (68%) | 322 (32%) |
| 7 (128) | 608 | 291 (48%) | 317 (52%) | 412 (68%) | 196 (32%) |
| 8 (256) | 331 | 171 (52%) | 160 (48%) | 226 (68%) | 105 (32%) |
(%) denotes a percentage of the given case out of # total.
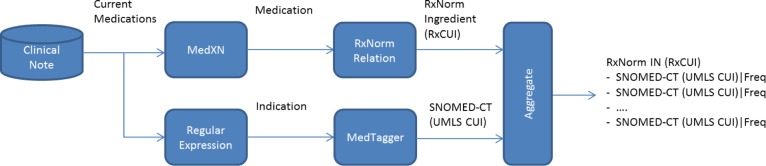
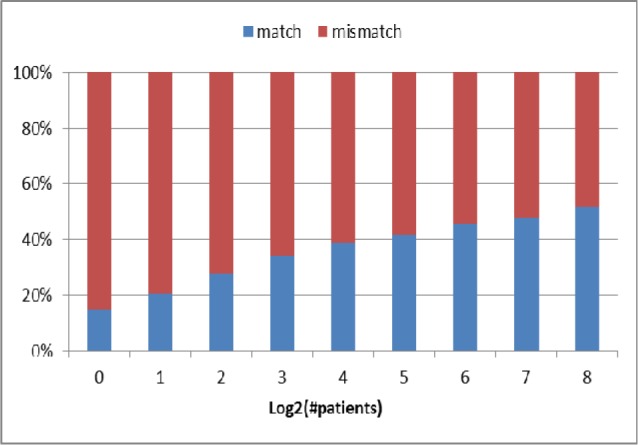
Mayo’s medication indications that appear in a low number of patients might be incorrect or simply noise, because of human mistakes or the system error in extracting or normalizing indications. Hence, we investigated statistics at a different level based on patient volume, as shown in Table 2. The higher the number of patients who have the given medication indication—ie, the higher the number in log2(#pts)—the greater the reliability of the given medication-indication pairs. We can also assume that the portion of the number of matches between Mayo and MEDI would be increased as the given medication indications occur in the higher number of patients. As expected, the match ratio of Mayo’s medication-indication pairs with MEDI increases when the given medication indications appear in a higher number of patients (see Figure 3 and 4). This phenomenon is more significant in the original match than the flexible match.
Figure 3.
A ratio of match and mismatch Mayo’s medication-indication with MEDI (Exact match)
Figure 4.
A ratio of match and mismatch Mayo’s medication-indication with MEDI (Flexible match)
In MEDI, there exists a marker that denotes ‘possible label use’ whether the given indication can be considered as a labeled use or not. In Table 3, the column ‘# potential off-labels in matches’ denotes the number of matched Mayo medication-indication pairs with MEDI, but their indications are not considered as a ‘possible label use’ in MEDI. The column ‘# potential off-labels in mismatches’ denotes the number of the mismatched Mayo medication-indication pairs, in that the Mayo medication is in MEDI but its corresponding indication is not in MEDI. In light of these facts, we may consider those two cases above (ie, ‘# potential off-labels in matches’ and ‘# potential off-labels in mismatches’) as the potential off-label candidates. However, those indications should be further reviewed and validated thoroughly to determine true off-label uses.
Table 3.
Statistics of potential off-label indications in Mayo.
| log2(#pts) | # total | Exact match | Flexible match | ||
|---|---|---|---|---|---|
| # potential off-labels in matches (%) | # potential off-labels in mismatches (%) | # potential off-labels in matches (%) | # potential off-labels in mismatches (%) | ||
| 0 (1) | 29823 | 1901 (6%) | 23905 (80%) | 9733 (33%) | 10967 (37%) |
| 1 (2) | 15677 | 1349 (9%) | 11706 (75%) | 5106 (33%) | 5468 (35%) |
| 2 (4) | 8095 | 897 (11%) | 5498 (68%) | 2643 (33%) | 2659 (33%) |
| 3 (8) | 4715 | 613 (13%) | 2917 (62%) | 1516 (32%) | 1434 (30%) |
| 4 (16) | 2850 | 387 (14%) | 1619 (57%) | 886 (31%) | 816 (29%) |
| 5 (32) | 1710 | 236 (14%) | 928 (54%) | 510 (30%) | 481 (28%) |
| 6 (64) | 997 | 144 (14%) | 501 (50%) | 267 (27%) | 278 (28%) |
| 7 (128) | 608 | 82 (13%) | 285 (47%) | 150 (25%) | 164 (27%) |
| 8 (256) | 331 | 38 (11%) | 146 (44%) | 70 (21%) | 91 (27%) |
(%) denotes a percentage of the given case out of # total.
Figures 5 and 6 show the portions of potential off-label candidates from Mayo’s medication-indication pairs when log2(#pts) is 5 when using the exact match and flexible match, respectively. For the exact match, the ratio of potential off-label candidates is 68% (= 54% in mismatch + 14% in match, Figure 5). Whereas for the flexible match, the ratio of potential off-label candidates is 58% (= 30% in mismatch + 28% in match, Figure 6).
Figure 5.
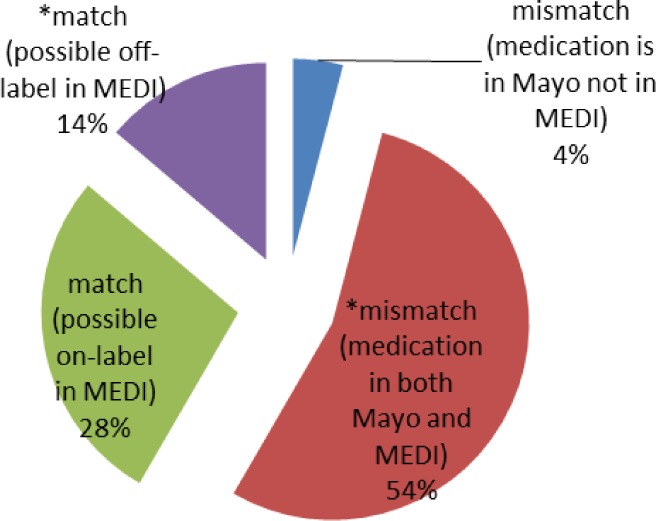
Off-label candidates (starts with *) in Mayo (log2(#pts)=5, Exact match)
Figure 6.
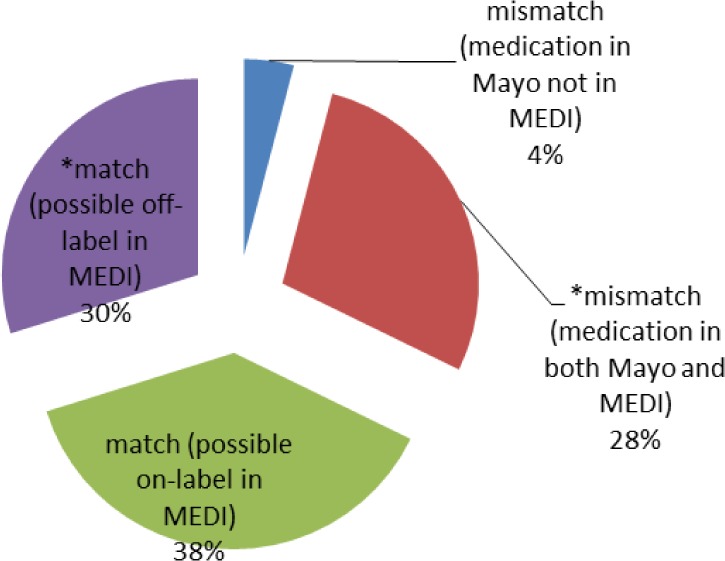
Off-label candidates (starts with *) in Mayo (log2(#pts)=5, Flexible match)
Table 4 shows some examples from the mismatch indications where medications are in both Mayo and MEDI but Mayo’s indications were not found in MEDI in flexible match. We manually examined MEDI’s indications for a given medication to see if there exist any similar indications to those of Mayo in a broad sense. If we found any similar indications, we place them into the column ‘MEDI indication close to Mayo,’ otherwise, we place ‘-’ in this column. As can be seen in Table 4, manually identified MEDI’s indications share common high-level indications with Mayo (eg, ‘back pain’ vs. ‘general pain’; ‘pink eye’ vs. ‘other ill-defined disorders of eye’). However, there are still some indications that were not able to be matched with MEDI in this manual process (ie, the cells with ‘-’). Most of these cases seem to be specific medical problems asserted by clinicians rather than general indications, which more likely appear in the low number of patient frequency. For example, Lidocaine’s general use is ‘numbness or loss of feeling’ but Mayo’s indication is ‘vertebral compression fractures,’ Clobetasol’s general use is ‘itching, redness’ but Mayo’s indication is ‘insect bite.’
Table 4.
Manual match of mismatched indications between Mayo and MEDI in flexible match.
| log2(#pts) | Medication | Mayo indication | MEDI indication (close to Mayo) |
|---|---|---|---|
| 0 ~ 1 | lidocaine | vertebral compression fractures | – |
| clobetasol | insect bite | – | |
| codeine | pain in right breast | chest pain, generalized pain | |
| gabapentin | PTSD | – | |
| hydrocortisone | nose sore | – | |
| 1 ~ 2 | omeprazole | pregnancy nausea | Nausea alone |
| amoxicillin | foot wound | – | |
| hyoscyamine | stomach cramps | unspecified disorder of stomach | |
| insulin lispro | dms | diabetes mellitus | |
| 2 ~ 3 | nabumetone | ankle pain | generalized pain |
| prednisone | facial swelling | – | |
| mupirocin | skin irritation | unspecified disorder of skin | |
| rifaximin | small bowel bacterial overgrowth | irritable bowel syndrome | |
| topiramate | chronic daily headache | cluster headache syndrome | |
| neomycin | conjunctivitis | other ill-defined disorders of eye | |
| 3 ~ 4 | prednisone | urinary tract infection | – |
| etodolac | back pain | acute pain, generalized pain | |
| amlodipine | vasospasm | – | |
| levalbuterol | cough | – | |
| digoxin | heart rate control | congestive heart failure (CHF) | |
| 4 ~ 5 | glyburide | gestational diabetes | type II diabetes mellitus |
| tramadol | arthritis pain | acute pain, chronic pain, generalized pain | |
| lidocaine | blood draw | – | |
| loratadine | asthmatic | – | |
| benzocaine | mouth sores | candidiasis of mouth | |
| clobetasol | scalp dermatitis | contact dermatitis and other eczema | |
| 5 ~ 6 | fluticasone | sinus congestion | – |
| docusate | hard stools | constipation | |
| bupropion | anxiety depression | major depressive disorder | |
| prednisone | poison ivy | – | |
| methylphenidate | idiopathic hypersomnia | ADHD | |
| 6 ~ 7 | oxycodone | knee pain | chest pain, chronic pain, generalized pain |
| fluticasone | vasomotor rhinitis | chronic rhinitis, allergic rhinitis | |
| tacrolimus | psoriasis | Other atopic dermatitis | |
| triamterene | hypertensive | hypertension | |
| 7 ~ 8 | quetiapine | panic attacks | schizophrenia, bipolar |
| ketorolac | headaches | generalized pain | |
| polymyxin b | pink eye | other ill-defined disorders of eye | |
| varenicline | quit smoking | unspecified drug dependence | |
| epinephrine | bee stings | – | |
| 8 ~ | lorazepam | panic attacks | panic disorder without agoraphobia |
| citalopram | anxiety depression | anxiety state unspecified | |
| albuterol | SOB | shortness of breath | |
| diphenhydramine | sleep | persistent disorder of sleep | |
| acetaminophen | cold symptoms | acute nasopharyngitis (common cold) |
Based on the previous comparison between Mayo and MEDI, we investigated actual examples of potential off-label candidates from Mayo’s medication-indication data. Tables 5 and 6 show potential off-label indications (the second column) and actual labeled indications (the third column). Table 5 contains examples of medication indications that appear in Mayo but not in MEDI, which are regarded as potential off-label uses. Table 6 contains examples of medication indications that appear in both Mayo and MEDI but which MEDI indicates not ‘possible label use.’ Since these indications are not marked as a possible label by MEDI, we might also assume them to be potential off-label uses.
Table 5.
Examples of potential off-label indications (exist in Mayo but not in MEDI)
| Medication | Indication in Mayo (off-label) | On-label Indication |
|---|---|---|
| Brimonidine | photophobia | glaucoma |
| Bupropion | smoking cessation assistance | depression |
| Albuterol | cough | asthma |
| Doxepin | allergies, hives | depression, anxiety, sleep disorders |
| Modafinil | wakefulness, alertness | narcolepsy |
| Sertraline | bipolar disorder | depression |
Table 6.
Examples of potential off-label indications (exist in Mayo and MEDI’s possible off-label)
| Medication | Indication in Mayo and MEDI (off-label) | On-label Indication |
|---|---|---|
| Azithromycin | traveler’s diarrhea | certain bacterial infections |
| Gabapentin | hot flashes | certain types of seizures |
| Trazodone | difficulty sleeping | antidepressant |
| Methylphenidate | depression | ADHD, narcolepsy |
| Duloxetine | anxiety | depression |
We have examined these potential off-label indications through Wikipedia and Internet searches and have verified that they are treated as off-label uses. Through this investigation, we also found many psychiatric medications are prescribed for off-label uses.
Discussion
A large volume of medication and indication occurrences from Mayo clinical notes have been analyzed and compared with MEDI that compiled from four public medication resources. Unlike previous studies, we used actual medication-indication pairs asserted by clinicians in real clinical practice. For exact and flexible matches (Table 2), Mayo’s medication-indication pairs match MEDI approximately 15% to 52% and 58% to 68% of the time, depending on the number of patients with the given indication, respectively.
Mayo’s medication-indication pairs demonstrate that they have both off- and on-label medication uses. The ratio of potential off-label candidates when considering the indications that occurs in greater than or equal to 32 patients (log2(#pts)=5) is approximately 68% and 58% for exact and flexible matches, respectively. However, these represent rough ‘potential candidates’ that may be off-label indications which require further validation.
It should also be noted that the overall ratio of potential off-label indications found in our results does not represent the actual ratio of off-label uses in Mayo as a whole, because we only investigated the medication descriptions that include indications, but these are only a small portion of the total medication descriptions. Also, we do not know when the clinicians actually add indications to in the Current Medication section of our clinical notes.
Instead of medication information in clinical narratives, which is often described with intended indications, we used medication information in a specific section—ie, Current Medication—that contains a majority of patient-intake medications in a list format (as shown in Figure 1). This provides us with a relatively straightforward method of extracting medication-indication pairs. Using current medications may provide another benefit. Current medications may infer active diagnoses of patients and therefore support the compilation of the patient’s comprehensive problem list, which is often difficult to maintain and manage in clinical practice. If we were able to obtain missing indications in the Current Medication section through examining other portions of clinical narratives, we would be able to compile comprehensive patient medication-indication lists, which would aid in better clinical care and decision support.
Off-label medication use is common in clinical practice, but most of these off-label uses lack rigorous evidence or studies to support them. However, off-label medication use is legal and often useful. Table 5 and 6 show good examples of potential off-label use as they show that clinicians use them differently from the original pharmaceutical use. Analyzing actual clinical practice of off-label use through a well-managed database would likely prove beneficial to patient treatments, patient safety, and quality improvements. Our study may serve as a foundation for further investigation and the eventual development of such a database.
There are some limitations to this study. Our analysis was based on medication-indication pairs automatically extracted by the system. We believe that most are correct, because medication indication descriptions in our clinical notes are relatively straightforward for extraction purposes. However, there exists the possibility that some medications and their indications could be incorrectly linked. We used normalized Mayo medication-indication pairs to compare with those of MEDI but this normalization has not been thoroughly evaluated in this study. Although we employed flexible matches between Mayo and MEDI, some mismatches may occur because of normalization differences between the two data sets. Also, false matches may occur because of over-generalization (ie, within two steps of navigation in the UMLS network). One-step distance or using certain types of relationship would be alternative ways to investigate. The appropriate medical-concept normalization would be necessary to better match indications between different medication resources.
Acknowledgments
This work was made possible by joint funding from National Institute of Health (R01GM102282A1 and R01LM011369) and National Science Foundation (ABI:0845523).
References
- 1.Ghitza UE, Sparenborg S, Tai B. Improving drug abuse treatment delivery through adoption of harmonized electronic health record systems. Substance abuse and rehabilitation. 2011;(2):125. doi: 10.2147/SAR.S23030. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Roth CP, Lim Y-W, Pevnick JM, Asch SM, McGlynn EA. The challenge of measuring quality of care from the electronic health record. American Journal of Medical Quality. 2009;24(5):385–394. doi: 10.1177/1062860609336627. [DOI] [PubMed] [Google Scholar]
- 3.Tracy RP. ‘Deep phenotyping’: characterizing populations in the era of genomics and systems biology. Current opinion in lipidology. 2008;19(2):151–157. doi: 10.1097/MOL.0b013e3282f73893. [DOI] [PubMed] [Google Scholar]
- 4.Wilke R, Xu H, Denny J, Roden D, Krauss R, McCarty C, Davis R, Skaar T, Lamba J, Savova G. The emerging role of electronic medical records in pharmacogenomics. Clinical Pharmacology & Therapeutics. 2011;89(3):379–386. doi: 10.1038/clpt.2010.260. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Radley DC, Finkelstein SN, Stafford RS. Off-label prescribing among office-based physicians. Archives of Internal Medicine. 2006;166(9):1021–1026. doi: 10.1001/archinte.166.9.1021. [DOI] [PubMed] [Google Scholar]
- 6.Bashford JN, Norwood J, Chapman SR. Why are patients prescribed proton pump inhibitors? Retrospective analysis of link between morbidity and prescribing in the General Practice Research Database. Bmj. 1998;317(7156):452–456. doi: 10.1136/bmj.317.7156.452. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Walton S, Galanter W, Rosencranz H, Meltzer D, Stafford R, Tiryaki F, Sarne D. A trial of inpatient indication based prescribing during computerized order entry with medications commonly used off-label. Applied clinical informatics. 2011;2(1):94. doi: 10.4338/ACI-2010-11-RA-0072. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Burton MM, Simonaitis L, Schadow G. Medication and indication linkage: a practical therapy for the problem list?. AMIA Annual Symposium Proceedings; 2008; pp. 86–90. [PMC free article] [PubMed] [Google Scholar]
- 9.Wei W-Q, Cronin RM, Xu H, Lasko TA, Bastarache L, Denny JC. Development and evaluation of an ensemble resource linking medications to their indications. Journal of the American Medical Informatics Association. 2013;20(5):954–961. doi: 10.1136/amiajnl-2012-001431. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Jung K, LePendu P, Shah N. Automated Detection of Systematic Off-label Drug Use In Free Text of Electronic Medical Records. AMIA Summits on Translational Science Proceedings. 2013:94. [PMC free article] [PubMed] [Google Scholar]
- 11.Li Y, Salmasian H, Harpaz R, Chase H, Friedman Carol. Determining the reasons for medication prescriptions in the EHR using knowledge and natural language processing. AMIA Annual Symposium Proceedings; 2011; pp. 768–776. [PMC free article] [PubMed] [Google Scholar]
- 12.First DataBank. http://www.firstdatabank.com/
- 13.Micromedex. http://www.micromedex.com.
- 14.Medi-Span. http:/www.medispan.com/
- 15.Gold Standard Drug Database. http:/www.goldstandard.com/product/gold-standard-drug-database/
- 16.Cerner Multum. http://www.multum.com/
- 17.Brown SH, Elkin PL, Rosenbloom S, Husser C, Bauer B, Lincoln M, Carter J, Erlbaum M, Tuttle M. VA National Drug File Reference Terminology: a cross-institutional content coverage study. Medinfo. 2004;11(Pt 1):477–481. [PubMed] [Google Scholar]
- 18.Bodenreider O, Nguyen DPC, Chuang P, Madden M, Winnenburg R, McClure R, Emrick S, D’Souza I. The NLM value set authority center. Studies in Health Technology and Informatics. 2013;192:1224. [PMC free article] [PubMed] [Google Scholar]
- 19.Ruch P, Gobeill J, Lovis C, Geissbühler A. Automatic medical encoding with SNOMED categories. BMC Medical Informatics and Decision Making. 2008;8(Suppl 1):S6. doi: 10.1186/1472-6947-8-S1-S6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Sohn S, Clark C, Halgrim S, Murphy S, Chute C, Liu H. MedXN: an Open Source Medication Extraction and Normalization Tool for Clinical Text. Journal of the American Medical Informatics Association. 2014 doi: 10.1136/amiajnl-2013-002190. Epub ahead of print. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Torii M, Wagholikar K, Liu H. Using machine learning for concept extraction on clinical documents from multiple data sources. Journal of the American Medical Informatics Association. 2011;18(5):580–587. doi: 10.1136/amiajnl-2011-000155. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Liu H, Bielinski S, Sohn S, Murphy S, Wagholikar K, Jonnalagadda S, KE R, Wu S, Kullo I, Chute C. An information extraction framework for cohort identification using electronic health records. . AMIA Summits Transl Sci Proc; 2013 Mar 2013; San Francisco, CA. pp. 149–153. [PMC free article] [PubMed] [Google Scholar]
- 23.Sohn S, Clark C, Halgrim S, Murphy S, Jonnalagadda S, Wagholikar K, Chute C, Liu H. Analysis of Cross-Institutional Medication Description Patterns in Clinical Narratives. Journal of Biomedical Informatics Insights. 2013 doi: 10.4137/BII.S11634. accepted. [DOI] [PMC free article] [PubMed] [Google Scholar]