

Abstract
Individuals with chronic conditions face challenges with maintaining lifelong adherence to self-management activities. Although reminders can help support the cognitive demands of managing daily and future health tasks, we understand little of how they fit into people’s daily lives. Utilizing a maximum variation sampling method, we interviewed and compared the experiences of 20 older adults with diabetes and 19 mothers of children with asthma to understand reminder use for at-home chronic disease management. Based on our participants’ experiences, we contend that many self-management failures should be viewed as systems failures, rather than individual failures and non-compliance. Furthermore, we identify key principles from reliability engineering that both explain current behavior and suggest strategies to improve patient reminder systems.
Introduction
People with chronic conditions, or those who care for others with chronic conditions, are expected to manage complex medical regimens. For many, the demands are monthly, weekly, or even daily. For example, patients with well-controlled hypertension, diabetes, and hyperlipidemia must perform more than 3,000 health-management activities a year to be adherent to recommended self-care guidelines1. These activities include making changes to their diet, requesting medication refills, adhering to a medication regimen, monitoring critical health indicators (e.g. blood pressure), getting lab tests done, attending appointments, getting annual screenings and immunizations, and managing symptoms2. As a result of these challenges, many patients are not able to meet their goals for daily self-care activities successfully. In fact, half of individuals diagnosed with a chronic condition—such as asthma, hypertension, and diabetes—do not adequately adhere to their prescribed medication regimens3 and miss as many as 21–34% of their scheduled appointments4. These failures in chronic disease management can lead to adverse patient outcomes, increased care costs, and create challenges to the patient-provider relationship5–7.
To support patients managing a chronic disease, health care systems increasingly send reminders for appointments and chronic and preventive care activities. Successful reminder systems can alert people to scheduled medical visits and screenings, improve adherence, and enhance communication between patients and their provider team8,9. Moreover, many patients already utilize personal reminder systems to remember everyday tasks. The following scenarios help illustrate how people incorporate explicit and implicit reminders into their daily routines:
Bob is a 60-year-old diabetic. His typical morning routine is to wake up, walk into his bathroom to take his medication that he keeps out on the counter, then have breakfast. As he walks into the kitchen, he sees his blood glucose meter sitting on the kitchen table and remembers that he needs to check and record his blood sugar. He then starts up his coffee machine, and glances at his wall calendar to see what is happening that week. While eating breakfast, he receives a call from his clinic reminding him about an appointment the next day. Later on, his wife, who is out of town, calls him to check-in. Realizing he forgot to check his blood sugar while making coffee, he walks back to the kitchen to get his glucose meter.
Cindy is a 34-year-old mother of a 9-year old child with persistent asthma. When she wakes up, she always glances at her smartphone’s calendar to see her agenda for the day. She also takes a minute to enter in a to-do list. Among other things, her son needs his allergy shot at the clinic and she needs to send off her sister’s birthday package. Before heading out, Cindy notices and grabs her son’s inhaler by the door to make sure it gets into his backpack for school that day. In the rush to get her son to school from the appointment, she forgets to stop by the post office. But on her way home later that day, Cindy passes a mailbox that reminds her to send off the package and she makes a turn to the nearest post office.
These vignettes, based on activities and experiences described by our study participants, demonstrate how people rely on a variety of tools and subtle triggers to help remember to perform future actions. In the first scenario, Bob relies mostly on environmental cues that are part of his morning routine. However, his wife will frequently check-in with him, which serves as a backup in case he does forget to do something. In contrast, Cindy makes heavy use of her mobile phone to track what she needs to do for the day. She also makes deliberate use of visual cues like placing the inhaler by the door to make sure her son takes his inhaler. Yet, in both situations, the two people still experienced minor failures in achieving their intended tasks.
In this paper, we examine how individuals responsible for managing their own or others’ chronic conditions integrate reminders and notification systems into their daily routines. By understanding these diverse individual experiences, we hope to gain insight into the optimal design characteristics for future patient reminder and support systems. We further contend that many self-care management failures may be accurately viewed as system failures, as opposed to failures of individuals10. Our work highlights the complex ecosystem of interactions, tasks, and reminders between the clinic and home environment for a person managing a chronic illness. Finally, we apply key principles from reliability engineering to help explain participants’ self-management behavior and offer suggestions for strategies to further improve patient reminder systems in the future.
Background and Related Work
This work draws on several divergent literatures: prospective memory as a basis for task planning and recall, clinical and personal reminder systems, and systems reliability engineering to frame patient self-care tasks and failures.
Prospective Memory as a Basis for Task Planning and Recall
Remembering to perform all the tasks expected for proper self-management requires effective recall of what has already happened and a continuous scan of what needs to happen in the near future. The process of remembering is frequently framed as either of two types: (1) retrospective memory that is concerned with the retrieval of past memories of people, events, and words, or (2) prospective memory that is concerned with remembering to perform a planned action or intention in the future11. The latter process includes short-term intentions—such as daily intake of a medication—as well as delayed actions—such as going to an annual checkup appointment—that could occur weeks or months in the future. Outlined in Figure 1, the process for realizing a delayed intention begins with encoding the future action, retaining the intention, and then retrieving the intention at the appropriate time to complete the action. This can occur through either an explicit reminder system or through spontaneous retrieval. Actions such as remembering to take medication at breakfast often rely on spontaneous retrieval of the intention that is triggered through environmental and physiological cues linked to daily routines. However, intermittent actions further out in time often involve a more explicit signaling cue—such as creating an alarm on a phone—to retrieve and execute the action at the right time12. In the case of an individual managing a chronic condition, the capacity to reliably shape and direct future behavior is critical to successfully managing the disease. The role of both explicit and implicit reminder systems within this memory process is the focus of this paper.
Figure 1.
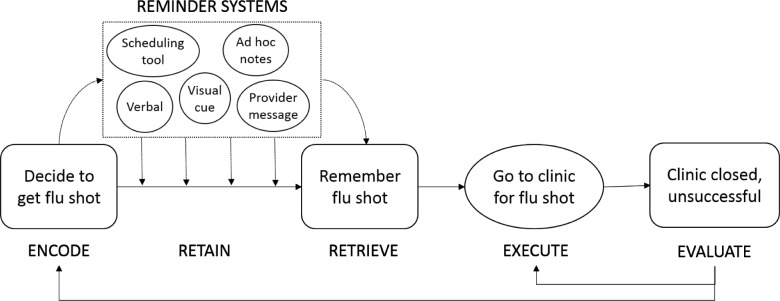
Model for establishing and realizing delayed intentions. Adapted from Ellis, 1996 13. When a person decides to get an annual flu shot (encoding), they need to maintain that intention over a delayed period (retention). At some point the person receives a signal to remember the flu shot (retrieval) and then goes to the clinic (execution). If successful (evaluation), the task is complete. Otherwise, the person attempts the activity again or re-plans the intention. In this model reminder systems provide a way for individuals to externalize the retention process as well as establish a way to cue retrieval of the delayed intention.
Clinic and Personal Reminder Systems to Support Recall
Reminders can be useful mechanisms to support the execution of delayed intentions described by prospective memory. James Reason describes the value of reminders in mitigating errors of omission that can lead to failures in planning and intention formation (encoding), intention storage (retention), action execution, and monitoring14. Research into reminders for health has typically evaluated clinic use of reminder systems. For example, health care organizations use postal mail or telephone calls to help prevent missed appointments and thereby reduce costs associated with disruptions to clinic workflow15. More recent articles have started to explore mobile phone-based strategies, such as text messaging and other types of electronic reminders8,16. Vervloet’s review of electronic reminder systems initiated by providers showed short-term effectiveness of these systems in supporting medication adherence but suggested more investigation of reminder content and timing8. In a cross-sectional survey of patient preferences, Finkelstein et al. found that personalizing the delivery mechanism improved patients’ responsiveness to reminders4. The research into clinic-initiated reminder systems indicates that they support improvements in patient adherence, are effective across diverse technologies, and are more likely to be successful through the personalization of message content based on patient preferences.
Outside of a clinic setting, individuals leverage a variety of tools for personal reminder systems. Grimes and Brush interviewed working parents and identified a number of challenges that they experienced in coordinating and interacting across their personal and professional schedules17. In a separate study, Brush highlighted the value of triggers in the workplace that are created from a mixture of explicit self-reminder systems, tacit “breadcrumbs” from recent activities, or based solely on memory to recall specific tasks18. However, there has been limited research into how these types of personal systems support patients’ multiple chronic and preventive health care needs. For example, a review by Kapur et al. focused on the use of memory aids for neurological rehabilitation of individuals with severe memory impairments due to injury or a disorder19. While reminder systems are prevalent in a variety of contexts, there is an opportunity to explore how personal systems are used for chronic disease management, and importantly, how these tools integrate with clinic reminder activities and the home environment.
Systems Reliability Engineering to Understand Errors and Failures
Within this paper, we frame chronic disease management as a complex system of technical, organizational, economic, environmental, and human components that interact for a common purpose—the maintenance and coordination of an individual’s health. This type of system highlights a growing trend in health care of utilizing human factors and ergonomics (HFE) concepts for designing patient-centered care. The National Research Council conducted a HFE evaluation of home health care that stressed systems engineering for designing technology interventions that facilitate interactions between the complex elements and tasks in the home environment20. Furthermore, Holden, Carayon, and colleagues introduced a popular framework for HFE thinking and reliability in health care with the Systems Engineering Initiative for Patient Safety (SEIPS) model21. The latest version of this model discusses the importance of a person-centered approach to work systems that include organizations, tools & technology, people, tasks, and the internal and external environments where the work takes place. In the context of reminders, the activity of remembering and executing self-management tasks at home involves the interplay between the patient, clinic, home environment, and devices and tools used to coordinate and execute care activities.
Building on HFE concepts, we are concerned with the reliability of the system to support individuals’ ability to use reminders to perform their care coordination tasks successfully. The principles of reliability science and engineering help to describe design strategies for mitigating and responding to failures in complex systems. Reliability refers to the probability that a system will meet its minimum performance requirements, without failure, for a given period of time22. Three activities in particular—engineered redundancy, diverse and independent design, and regular monitoring—can enhance the reliability of a system23. Redundancy describes systems where duplicate processes or components are used to increase availability in case of a single point of failure. For example, many cars are designed with twin hydraulic brake circuits to ensure that the vehicle can still stop if one circuit fails. However, redundant systems do not increase reliability in situations where they are vulnerable to the same defect—referred to as common cause failure. To mitigate this vulnerability, engineers incorporate diversity into their design so that a system uses two or more different, independent techniques or processes for the same functional purpose24. For example, when backing up a car, a driver can visually assess their environment with the car mirrors as well as listen to the beeping sounds produced by proximity sensors built into many modern vehicles. Finally, reliable systems can use monitoring to actively audit the system and mitigate the impact of a breakdown through early detection of failures. Modern automotive anti-lock systems actively monitor wheel deceleration and distance from other objects to adjust the brake speed and prevent uncontrolled skidding. Although researchers have used reliability engineering to frame inpatient safety25, none have used this framework to examine patient adherence to chronic disease management activities.
Study Overview
We conducted a series of semi-structured, in-depth interviews with patients diagnosed with Type 2 diabetes (n = 20) and mothers of children receiving treatment for asthma (n = 19). The choice of the two populations maximized the variation in the perspectives and experiences of individuals managing a chronic disease. Our sampling of parents of children with asthma focused on mothers, rather than fathers, since women in this age group also have a large number of prevention and maintenance activities and are typically the primary health information managers within the household26. The semi-structured interviews focused on reminder tools and systems that patients used for maintenance and care coordination activities such as appointment scheduling, medication adherence, and communication with their providers outside of the clinic. In addition to the interviews, the authors (LK, JE) toured the participants’ homes in order to directly observe the systems and tools used in this context. This study was reviewed and approved by our institution’s human subjects review board.
Sampling
We used purposeful sampling to identify participants that were representative of the general population in the Northwest United States based on gender, ethnicity, technology use (with recorded use of a patient portal as a proxy) and education. All participants were enrollees of an integrated healthcare delivery system that covers more than 300,000 members. Based on the sampling criteria, we contacted 586 individuals identified as either persons with diabetes or parents of a child with asthma. Of these, 402 could not be reached, refused to participate, or were lost to follow-up, and 118 were deemed ineligible based on follow-up screening. Of the remaining 66, we enrolled 39 participants, aged 27 to 88 (median=61). The diabetes cohort was older on average than the mothers of children with asthma and were less likely to use technology such as a patient portal for their health. Other details on our participant population are in Table 1. Each participant received a gratuity of $50 for completing the interview.
Table 1.
Description of study participants.
| Diabetes | Asthma | Combined | ||||
|---|---|---|---|---|---|---|
| N | % | N | % | N | % | |
| Participants | 20 | 100 | 19 | 100 | 39 | 100 |
| Female | 10 | 50 | 19 | 100 | 29 | 74 |
|
| ||||||
| Race/Ethnicity | ||||||
| White | 10 | 50 | 9 | 47 | 19 | 49 |
| Black | 6 | 30 | 6 | 32 | 12 | 31 |
| Asian | 2 | 10 | 1 | 5 | 3 | 8 |
| Hispanic | 1 | 5 | 1 | 5 | 2 | 5 |
| Mixed/Other | 1 | 5 | 2 | 11 | 3 | 8 |
|
| ||||||
| Technology Use | ||||||
| Patient Portal User | 13 | 65 | 18 | 95 | 31 | 79 |
|
| ||||||
| Education | ||||||
| High School or Less | 12 | 60 | 5 | 26 | 17 | 44 |
| More than High School | 8 | 40 | 15 | 79 | 23 | 59 |
Analysis
The interviews lasted from 40 to 90 minutes. The audio recordings from each interview were transcribed and reviewed using Atlas.ti 7 and identified as “A##” and “D##” for the asthma and diabetes cohorts, respectively. To maintain confidentiality, we removed all information that could identify the patient from the transcripts. During the data collection process, the authors periodically reviewed transcripts to identify emerging themes and to assess topic saturation. Using an open coding technique and an affinity diagramming process27, the authors clustered related terms and organized preliminary themes into higher-level categories. A subset of the authors then iterated on the codes through several rounds of transcript review to solidify the coding schema used for this article. One author used this schema to code each interview using Atlas.ti.
Results
Through this content analysis, we focused on two areas. First, we highlighted the reasons for failures in self-management routines as identified by participants during the interviews. Second, we characterized three strategies used by participants to improve the reliability of their reminder systems and overall management of their health. These strategies are summarized in Table 2.
Table 2.
Summary of reliability system design strategies used by participants to enhance self-care reminders.
| Reliability Strategy | Benefits | Drawbacks |
|---|---|---|
| Redundancy: Repeated reminders, back-up systems | • Back-ups ensure availability of reminder for retrieval at the right time. • Repeated alerts enhance retention. |
• Too many back-up systems can create unwanted noise and increase chance of being ignored. |
| Diversity:Independent systems, different communication modes | • Separate clinic and personal systems reduces reliance on single operator. • Multiple modalities improves availability of reminder for retrieval. |
• Additional systems increase complexity and can create new opportunities for failure. |
| Monitoring: Validating reminder capture, double-checking for errors | • Improves retention through repeated exposure. • Increases likelihood of catching errors in the reminder system. |
• Additional work required of system operators • Challenges with maintaining this behavior routinely. |
Sources of Reminder Errors and Task Failures
Throughout the study, the participants provided examples of breakdowns in their self-management routines that included failures in memory, missed environmental signals, and failures in capturing tasks within a reminder system.
Memory failures were a common reason for failure as well as a rationale for using explicit reminder systems. Based on the prospective memory process in Figure 1, these types of errors can be described as retention and retrieval failures. For example, participants described how easy it was to forget because of their hectic schedules. A07 expresses the challenges representative of many busy mothers. “If I don’t have anything immediately reminding me of it, it’s out of my head because I have so much going on. We have kids to pick up, drop off. We have cleaning house, I’ve got selling things, I’ve got to meet people.” [A07]. D02 and many elderly participants with diabetes described concerns with growing memory deficits as they aged. They expressed interest in updating their reminder systems as their memory started to become less reliable. Despite this interest, participants often relied on informal, tacit signals in the environment. For example, it was only after scheduling a separate appointment for herself that A08 remembered her child’s annual well-child visit was overdue. Similarly, other participants remembered to go in for screenings and tests only after scheduling a visit for a separate health need. Reliance on environmental cues was particularly common for medication management. One participant described managing her child’s inhaler by paying attention to when “the propellant in it doesn’t expel quite as well and so he doesn’t feel like he’s getting or receiving the medication as well and so he’ll tell us that he needs a new one” [A11]. Without having an explicit visual cue or timely notification from her child, she relies on trying to remember how much time has passed since the last refill. Tacit signals are dependent on the environmental cue occurring at the right time and place. If the person misses this signal, they can experience a retrieval failure.
In addition to missing cues from informal reminders, participants also described breakdowns with their reminder tools. In some situations the reminder was never captured and therefore never signaled the appropriate behavior. This type of encoding failure often occurs because individuals get distracted from capturing the task or do not have access to their reminder tool when they need it. One participant described how, “I’ll make an appointment and then start doing something else so I didn’t write it down and just hope that I’ll remember it.” [A10]. In this situation, A10 missed an appointment for her baby because the event did not get recorded into her phone and she did not get a reminder call. A14 used a system where she printed out calendars and captured appointments, bills, and other items. However, when she misplaced it, “I was freaking out, because I had actually taken the time to write everything down—they had a trove of information on it. I couldn’t find it and then I was like how the heck am I going to do this if I don’t have a backup?” [A14]. Her situation mirrored many of the participants where, because of a busy schedule, being away from home, or not having access to their normal reminder tool, they failed to set up or retrieve the cue from their system to perform the action in the future. Despite having systems that they often described as being fairly reliable, participants still experienced situations in which some aspect of their reminder process fell apart.
Strategies for Redundancy in Reminder Systems
To compensate for these types of memory and organizational errors, participants employed a number of strategies to improve the reliability of remembering certain tasks for their care management. In particular, to mitigate the chance that one reminder system might fail, participants integrated duplicative or redundant reminder systems in their homes. In many cases, having redundancy was simply a backup. D04 used the calendar on her computer to manage most of her reminders. However, she purchased a smartphone because she recently got a virus on her computer and was concerned about its reliability in the future. Other individuals in the study described how having their spouse or children aware of their health management tasks served as a useful backup. They would regularly discuss upcoming events with the family member or ask them to check-in to make sure the participant took their medication. Even though it was rarely necessary, “they’re there if we do need them” [D08].
Participants expressed that having multiple, redundant systems helped to ensure that reminders get encoded. D02 maintained three calendars so that the intended task was captured regardless of where she was in the home. An added value of having multiple systems was that it helped to retain what she need to do. “It’s like repetition. If you say something to me and say the same thing several times, it rings a bell and I remember it. I think that’s what the calendar does.” [D02]. This system served as both a way to deal with memory deficits as well as ensure that upcoming events are always captured. A09 was worried that her husband would forget to pick up the kids and so “I told him the night before, I told him the morning of, I sent him a text from work, I called him to make sure - don’t forget.” [A09]. While that many reminders were likely unnecessary, it reassured the participant and increased her spouse’s awareness.
Although redundant systems have advantages, they can be a burden as well. Providers are typically very proactive about letting a patient know of an upcoming appointment to reduce the impact of a missed appointment on their clinic workflow. Some participants expressed an interest in streamlining their different reminder systems—from both their providers as well as their personal reminder tools—to remove duplicative work and unnecessary reminders.
“My son, his dentist office annoys the heck out of me because they send reminders two months in advance and then send another one a month in advance and at that time they want you to click confirm on the appointment and then after you confirm it, they send another one a week in advance and then call you. It’s overkill.” [A09]
While repeated reminders increases the chance that the patient is aware of the appointment or task, it also creates more noise. The participants described many redundant reminders as unhelpful in situations where they already were aware of the appointment or task or it was not applicable to their needs. If they felt that it was an unnecessary reminder, they would simply ignore it. This situation is analogous to the alert fatigue that health care providers face with poorly designed EMR and other practice management systems.
Strategies for Diversity in Reminder Systems
The individuals in this study not only performed redundant work as a protection against failures, but also used a diverse set of reminder systems (Figure 2). Diversity provides greater protection against system failures that can affect even redundant systems. For example, a clinic that sends multiple appointment reminder notices in the mail will fail if the patient’s address is incorrect. A phone that runs out of power will not be able to receive a text message about taking a medication. Throughout the interviews, the study participants described an array of modalities used for communication and reminders about upcoming tasks.
Figure 2.

Sample of personal reminder systems used by study participants. From left to right: a whiteboard-style calendar; a sticky note wrapped around the strap of a handbag; pill bottles placed upside down to indicate they have been taken for the day.
All of the study participants emphasized the value of traditional reminders initiated by the provider such as paper mail, phone calls, and secure messaging within a patient portal. However, participants still used a number of additional, personal reminder systems that ranged from technology-centric approaches—such as a mobile phone—to informal mechanisms such as the placement of a pillbox on the kitchen table. A06 would get multiple text messages and phone calls from her dentist leading up to an appointment, but would still enter it into her phone right away. The major tenet of the diversity principle is to ensure independence in redundant systems and subsystems. Thus, by incorporating reminders from clinics as well as their own systems, patients add a layer of reliability—they are able to rely on the provider messages if their personal system fails or rely on their own system if they do not receive a reminder from their clinic. D01 described an incident where she had a scheduled phone consult with her doctor. She recorded the appointment in her personal planner. However, the clinic did not record the phone call information correctly, and the physician didn’t call. D01 ended up having to call and remind the clinic about her phone appointment.
During the interviews, participants also explained how the mode of communication can have a meaningful impact. “The phone call I think it’s an accountability thing for me, if I actually physically speak to a person, it’s easier for me to go okay, I need to write it down and remember it.” [A03]. Synchronous communication modalities, particularly where the patient is interacting with a health professional, make it difficult to ignore the reminder and ensure that the reminder reaches its intended audience. Conversely, other participants discussed how it was easy to overlook or disregard asynchronous, electronic messages like emails because they get overloaded with too many messages in that format. Paper notifications were often valued because they are more tangible and visible around the home. “Well again, because I don’t get a lot of paper notifications, it feels serious and this should be done.” [A01]
Diversity can enhance reliability, but it can also create a chaotic and complex experience as the patient tries to integrate multiple systems. Several of the participants, for example, owned multiple computing devices that each had a different, incompatible operating system. This creates barriers in syncing activities across the platforms and in some situations encouraged participants to rely on a paper method instead. Additionally, participants that received care from multiple physicians described challenges with getting phone calls from some clinics and paper mail or electronic notifications from others. The diversity of communication approaches made it challenging to reliably integrate the reminders into their personal systems.
Strategies for Monitoring Reminder Systems
Study participants incorporated a habit of active monitoring of their reminder systems as an additional method for addressing reminder failures. Monitoring provided a way to identify errors, validate their reminder systems, and involve their friends and family members in supporting self-management. First, routine monitoring helps to identify when failures in self-management occurred.
“I have to be more conscious about did I take my pills…Did I do that? Sometimes I’ll actually get up and look to see whether I took my pills. It’s kind of like turning your headlights off on your car, yeah, I took my pills but when I stop and think about it, I got to go check because I don’t remember doing it.” [D20]
Even if a participant forgets to do something like take a medication, the process of monitoring can lead the person to recognize the error and then be in a position to make changes for the future. Although a clinic can notify a patient when they miss an appointment or test, no feedback process informs patients when they forget activities at home. Having a system in place for monitoring can be helpful to evaluate one’s behavior.
Second, active monitoring serves as a way of double-checking the reminder system and ensuring the right content is captured. The added benefit is that this helped participants retain what they needed to do in the future. Participants described deliberate efforts to consistently review and scan for future activities. “I try to check the next couple days ahead, like I’m thinking today plus two or something so I’m aware what’s coming.” [A09]. This participant also started involving her son this process by setting up a calendar in his room so he could cross off activities as they occurred. “If I get an appointment, then I write it down& I go in [the patient website], because it shows upcoming appointments so then I’ll print off the deal and go in there and check my calendar, so it’s a backup type, so I got a system, my checks and balances.” [D05]. Redundant, diverse reminder systems are helpful in supporting this kind of auditing behavior by helping participants compare the content of a reminder from multiple sources.
Third, participants often shared the responsibility of monitoring activities across family members to help reduce the workload. This demonstrated a distributed process for auditing reminder systems and ensuring completion of self-care behaviors. Informal dialogue between spouses or between parent and child appeared to be a subtle but valuable mechanism for reviewing and validating upcoming appointments, medications, and tasks on a regular basis. A01 spoke about how she had transitioned from administering her child’s inhaler directly to watching him do it himself. While this created other challenges around knowing if he took the inhaler correctly, A01 experience exemplified a transition in self-care responsibility common to many of the mothers of children with asthma.
Active monitoring does require additional work by participants and may be onerous when considering the activities already required for chronic disease management. Moreover, participants mentioned difficulties with making sure this type of monitoring is routine. A wall calendar with appointments listed is only useful as a reminder of upcoming events if the target audience makes the effort to review and validate the content. One participant assumed she had the correct information for an appointment on her wall calendar, but realized she had written the appointment on the wrong week after her husband walked by the calendar and pointed it out [D08]. Wall calendars contrast with systems like email and text messaging that will push information to the target based on a predefined event. However, sometimes these push systems actually discourage any active monitoring of a reminder system. “I guess the hope is that it’ll perform how I’ve asked it to, or that I’ve remembered to ask it to perform how I want it to.” [A08]. Another participant described how he messed up an appointment twice because he did not look back at his email about the appointment and his did not have his smartphone set properly to alert him [D16]. Becoming too dependent on the reminder system’s capacity to create notifications can create a new avenue for failure.
Discussion
Forgetfulness, confusion, external distractors, fatigue and even a person’s health condition can all lead to failures in self-management and perception of non-adherence. These types of errors, referred to as slips in human factors research, describe instances where an individual’s intentions get waylaid en route28. Although slips are often small failures, they are particularly relevant to breakdowns in the automatic, routine behavior that is at the heart of chronic disease management. Solely relying on memory or informal environmental cues may be adequate for a period of time, but if an individual does not retrieve the prospective action accurately or at the right time, no backup will ensure the activity happens. We observed participants adopting a variety of strategies—such as redundancy, diversity, and active monitoring behaviors—to improve the reliability of managing self-care responsibilities. Incorporating different systems, people, and modes of communication ensured multiple, repeated communication paths for reminders in the event of one system failing. Moreover, participants did not just rely on different tools and modalities, but continually audited these systems to ensure that they had the correct information and that activities were completed successfully.
The challenge is that incorporating redundancy and diversity across multiple, separate systems involves tradeoffs between reliability and complexity. Diversity inherently increases complexity, and the need for synchronization among multiple systems could create more opportunities for failure. Furthermore, as participants in this study described, there is a risk of noise fatigue when dealing with multiple reminders from multiple sources. Health care organizations need to be aware of the additional workload placed on patients at home and reduce complexity through more tailored communication and easier integration of clinic-based reminders with patient reminder systems. By evaluating chronic disease self-management through a systems lens, we argue that trying to fix breakdowns in self-management should focus on designing system-level changes that focus on the experience of patients.
Designing for Human Error
Importantly for systems-thinking, our study highlights the variety of ways that failures can occur in remembering to perform self-care management activities. Therefore, the design of reminder systems to support self-management should account for errors by making it easier to detect, evaluate, and respond to failures when they do occur. The concepts of redundancy, diversity, and monitoring represent system design concepts that, integrated with the prospective memory process (Figure 1), can inform approaches to the future design of reminder systems. In addition, well-established systems engineering methodologies and tools can support this design and evaluation process. For example, concurrent engineering and quality functional deployment (QFD) use methods similar to participatory design to explicitly capture all stakeholder needs in a complex system29, including less visible needs—such as the personal reminder work of patients with chronic diseases. The SEIPS system model further reinforces the importance of design that incorporates the needs of patients and caregivers involved in chronic disease management work21.
James Reason suggests that all reminders should meet certain universal criteria so that they are conspicuous at the right time, contiguous or available in time and space, provide the necessary context and content for the intended actions or tasks that need to be done14. While the patient reminder systems in this study incorporated many of these qualities and avoided errors in encoding, retention, and retrieval through redundant and diverse design, they often lacked a feedback loop to track if an activity was performed or to support evaluation of errors that may have occurred. An important aspect of high reliability systems is the practice of assessing failures in order to actively identify, correct, or mitigate the sources of failure in the future. Assessing variation in self-care management and if performance is within acceptable boundaries requires better tools and processes for capturing the metrics and data to calculate the variation. Information technology has the ability to support more robust monitoring and learning through different notification processes, passive data collection on behaviors/activity, and enhanced summary reports and real-time feedback. Participants across both cohorts leveraged mobile phones and other computing devices to support their self-management efforts. Increasingly, mobile phones link with ubiquitous sensing tools to support automated, detailed tracking of health metrics and performance around daily activities. These sensing tools can reduce patient work, integrate diverse metrics, provide feedback on progress towards achieving health goals, and identify deviations that are the result of errors or other failures. However, systems thinking and systems engineering principles should be considered in the design and the use of these tools so that they integrate in the wider context of strategies for more reliable self-care management.
Study Limitations
As with any qualitative study, our findings might not be fully representative of the populations under consideration. Despite making considerable effort to sample for a representative patient population, it is possible that our participants differ from other patients in terms of self-efficacy or their organization with managing their care. Because the diabetic population in this study encompassed a narrow demographic of mostly elderly, retired individuals, it is possible that we did not adequately capture a wide enough array of experiences and strategies for managing diabetes. However, we were able to contrast their experiences with those of young mothers taking care of their children with asthma. These mothers were often working and were more likely to use technology. Finally, the way that the participants used reminder systems in this study could reflect disease-specific needs of our two cohorts.
Conclusion and Future Work
In summary, the experiences of our participants managing chronic disease at home highlights the diverse strategies they employ to manage their schedules and tasks. Moreover, even though many clinics and health systems have implemented reminder systems—such as follow-up phone calls—our study showed that patients must still do extensive work at home to integrate these reminders into their daily lives. These separate reminders enhance reliability through increased diversity, but also add to the overall complexity of the system. Participants often felt confident in relying on their memory for most routine needs, yet still valued redundant reminders as a backup to deal with any memory slips. We also note that in addition to formal systems—such as calendars—many participants in this study relied on subtle systems similar to what Donald Norman refers to as “knowledge in the world”28. These cues that are visible in the environment and trigger prospective memories are less visible but important to be aware of with evaluating reminders and support systems for chronic care management. Technologies that recognize and integrate with these tacit signals have the potential to provide more context-sensitive reminders.
Our findings also support evaluating failures in self-management from a systems perspective, rather than simply attributing a failure to individual’s lack of responsibility. While non-adherence is a legitimate issue, our participants’ experiences make it clear that some self-care failures are unintentional and can best be characterized as breakdowns in the interaction between people, machines, and environments within a system. To mitigate failures, many patients incorporated key characteristics from reliability science into their personal reminder systems—characteristics such as redundancy, diversity, and monitoring behaviors. We are not aware of other studies that have examined these strategies from a system reliability perspective. As future work seeks to support patients’ ability to manage chronic conditions outside of the clinic, it will be important to design self-care and reminder tools that also capitalize on these reliability principles. Healthcare providers, systems, and designers should consider the use of engineering design, evaluation, and control methods to explore this subsystem of patient reminder work that is prevalent among individuals with chronic conditions. Greater understanding of how this patient work integrates with clinic workflows and programs can lead to more reliable care management and ideally improved outcomes.
Acknowledgments
This project was supported by grant # R01HS021590 from the Agency for Healthcare Research and Quality (AHRQ).
References
- 1.Steiner JF. Rethinking adherence. Ann Intern Med. 2012 Oct 16;157(8):580–5. doi: 10.7326/0003-4819-157-8-201210160-00013. [DOI] [PubMed] [Google Scholar]
- 2.Barlow J, Wright C, Sheasby J, Turner A, Hainsworth J. Self-management approaches for people with chronic conditions: a review. Patient Educ Couns. 2002;48(2):177–87. doi: 10.1016/s0738-3991(02)00032-0. [DOI] [PubMed] [Google Scholar]
- 3.Sabaté E. Adherence to long-term therapies: evidence for action. Geneva, Switzerland: World Health Organization; 2003. [Google Scholar]
- 4.Finkelstein SR, Liu N, Jani B, Rosenthal D, Poghosyan L. Appointment reminder systems and patient preferences: Patient technology usage and familiarity with other service providers as predictive variables. Health Informatics J. 2013 Jun;19(2):79–90. doi: 10.1177/1460458212458429. [DOI] [PubMed] [Google Scholar]
- 5.Junod Perron N, Dao MD, Righini NC, Humair J-P, Broers B, Narring F, et al. Text-messaging versus telephone reminders to reduce missed appointments in an academic primary care clinic: a randomized controlled trial. BMC Health Serv Res. 2013 Jan;13:125. doi: 10.1186/1472-6963-13-125. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Schectman JM, Schorling JB, Voss JD. Appointment adherence and disparities in outcomes among patients with diabetes. J Gen Intern Med. 2008 Oct;23(10):1685–7. doi: 10.1007/s11606-008-0747-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Hussain-Gambles M, Neal RD, Dempsey O, Lawlor D a, Hodgson J. Missed appointments in primary care: questionnaire and focus group study of health professionals. Br J Gen Pract. 2004 Feb;54(499):108–13. [PMC free article] [PubMed] [Google Scholar]
- 8.Vervloet M, Linn AJ, van Weert JCM, de Bakker DH, Bouvy ML, van Dijk L. The effectiveness of interventions using electronic reminders to improve adherence to chronic medication: a systematic review of the literature. J Am Med Inform Assoc. 2012;19(5):696–704. doi: 10.1136/amiajnl-2011-000748. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Szilagyi PG, Bordley C, Vann JC, Chelminski A, Kraus RM, Margolis P a, et al. Effect of patient reminder/recall interventions on immunization rates: A review. JAMA. 2000 Oct 11;284(14):1820–7. doi: 10.1001/jama.284.14.1820. [DOI] [PubMed] [Google Scholar]
- 10.Steiner JF. Rethinking adherence. Ann Intern Med. 2012 Oct;157(8):580–5. doi: 10.7326/0003-4819-157-8-201210160-00013. [DOI] [PubMed] [Google Scholar]
- 11.Kliegel M, McDaniel MA, Einstein GO, editors. Prospective Memory: Cognitive, Neuroscience, Developmental, and Applied Perspectives. Taylor & Francis Group; 2008. [Google Scholar]
- 12.Daniel MAMC, Einstein GO. Strategic and Automatic Processes in Prospective Memory Retrieval: A Multiprocess Framework. 2000;144(September):127–44. [Google Scholar]
- 13.Ellis J. Retrieval Cue Specificity and the Realization of Delayed Intentions. Q J Exp Psychol Sect A. 1996 Nov;49(4):862–87. [Google Scholar]
- 14.Reason J. Combating omission errors through task analysis and good reminders. Qual Saf Health Care. 2002 Mar;11(1):40–4. doi: 10.1136/qhc.11.1.40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Hashim MJ, Franks P, Fiscella K. Effectiveness of telephone reminders in improving rate of appointments kept at an outpatient clinic: a randomized controlled trial. J Am Board Fam Pract. 2001;14(3):193–6. [PubMed] [Google Scholar]
- 16.Gurol-Urganci I, de Jongh T, Vodopivec-Jamsek V, Atun R, Car J. Mobile phone messaging reminders for attendance at healthcare appointments. Cochrane database Syst Rev. 2013 Jan;12(12):CD007458. doi: 10.1002/14651858.CD007458.pub3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Grimes A, Brush AJ. Life scheduling to support multiple social roles; Proceeding of the ACM CHI conference 2008; Florence, Italy: ACM Press; 2008. p. 821. [Google Scholar]
- 18.Brush AJB, Meyers BR, Tan DS, Czerwinski M. Understanding memory triggers for task tracking; Proceedings of the AMC CHI conference 2007; San Jose, CA: ACM Press; 2007. p. 947. [Google Scholar]
- 19.Kapur N, Glisky EL, Wilson B a. Technological memory aids for people with memory deficits. Neuropsychol Rehabil. 2004 Mar;14(1–2):41–60. [Google Scholar]
- 20.National Research Council . Health Care Comes Home: The Human Factors. Washington, DC: The National Academies Press; 2011. [Google Scholar]
- 21.Holden RJ, Carayon P, Gurses AP, Hoonakker P, Hundt AS, Ozok AA, et al. SEIPS 2.0: a human factors framework for studying and improving the work of healthcare professionals and patients. Ergonomics. 2013 Jan;56(11):1669–86. doi: 10.1080/00140139.2013.838643. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Zio E. Reliability engineering: Old problems and new challenges. Reliab Eng Syst Saf. 2009 Feb;94(2):125–41. [Google Scholar]
- 23.International Atomic Energy Agency . Protecting against Common Cause Failures in Digital I & C Systems of Nuclear Power Plants. Vienna: International Atomic Energy Agency; 2009. [Google Scholar]
- 24.Littlewood B, Strigini L. Redundancy and Diversity in Security; 9th European Symposium on Research in Computer Security; Sophia Antipolis, France. 2004. pp. 423–38. [Google Scholar]
- 25.Luria JW, Muething SE, Schoettker PJ, Kotagal UR. Reliability science and patient safety. Pediatr Clin North Am. 2006 Dec;53(6):1121–33. doi: 10.1016/j.pcl.2006.09.007. [DOI] [PubMed] [Google Scholar]
- 26.Moen A, Brennan PF. Health@Home: the work of health information management in the household (HIMH): implications for consumer health informatics (CHI) innovations. J Am Med Inform Assoc. 12(6):648–56. doi: 10.1197/jamia.M1758. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Martin B, Hanington BM. Universal methods of design: 100 ways to research complex problems, develop innovative ideas, and design effective solutions. Rockport Publishers; 2012. [Google Scholar]
- 28.Norman DA. The Design of Everyday Things. New York: Basic books; 2002. [Google Scholar]
- 29.Reid PP, Compton WD, Grossman JH, Fanijang G, editors. Building a Better Delivery System: A New Engineering/Health Care Partnership. Washington, DC: The National Academies Press; 2005. [PubMed] [Google Scholar]