

Abstract
The impact of the intensity of graft-versus-host-disease immunoprophylaxis on transplantation outcomes in patients undergoing transplantation following reduced-intensity conditioning is unclear. This study addresses this issue in 228 adult patients above 50 years of age with acute myeloid leukemia in first complete remission given peripheral blood stem cells from HLA-identical siblings after fludarabine and 2 days of intravenous busulfan reduced-intensity conditioning. A total of 152 patients received anti-thymocyte globulin, either in combination with cyclosporine A in 86 patients (group 1), or with cyclosporine A and mycophenolate mofetil or short course methotrexate in 66 patients (group 2). The remaining 76 patients did not receive anti-thymocyte globulin but were given cyclosporine A and methotrexate or mycophenolate mofetil (group 3). Incidences of grade II-IV acute graft-versus-host-disease were comparable in the three groups (16.5%, 29.5% and 19.5% in groups 1, 2 and 3, respectively, P=0.15). In multivariate analysis, the absence of anti-thymocyte globulin was the only factor associated with a higher risk of chronic graft-versus-host-disease (P=0.005), while the use of triple immunosuppression (group 3) was associated with an increased risk of relapse (P=0.003). In comparison to anti-thymocyte globulin and cyclosporine A alone, the other two strategies of graft-versus-host-disease prophylaxis were associated with reduced leukemia-free survival and overall survival (P=0.001 for each parameter), independently of the dose of anti-thymocyte globulin. These data suggest that fine tuning of the intensity of this prophylaxis can affect the outcome of transplantation and that anti-thymocyte globulin and cyclosporine A alone should be the preferred combination with the fludarabine-busulfan reduced-intensity conditioning regimen and sibling donors.
Introduction
Allogeneic hematopoietic stem cell transplantation (HSCT) performed with reduced intensity conditioning (RIC) is a therapeutic option in particular for older patients or patients with co-morbidities.1–4 In this setting, the combination of fludarabine and 2 days of busulfan (Flu-Bu2) is a widely used RIC regimen.1–3,5 Initially described in HLA identical sibling peripheral blood stem cell transplantation, Flu-Bu2 was combined with anti-T-lymphocyte globulin (ATG) (Fresenius 10 mg/kg/day) and cyclosporine A (CsA) alone for the prophylaxis of graft-versus-host-disease (GVHD).1 However, the best GVHD prophylaxis combination in the Flu-Bu2 RIC regimen has not yet been established. In contrast to allogeneic HSCT with myeloablative conditioning, disease control after RIC relies on the development of an immunological graft-versus-leukemia effect (GVL).1,6,7 Since GVHD and GVL are closely linked,8–10 the possibility of discriminating between them by the use of in vivo T-cell depletion remains challenging, particularly in allogeneic HSCT performed after RIC. In this context, ATG can effectively prevent acute and chronic GVHD,5 but can also increase the risk of infectious complications and of relapse.3,11 It is now established that the effects of ATG in RIC are dose-dependent,3 and that intermediate doses of thymoglobulin between 4 and 6 mg/kg seem to prevent GVHD optimally while sparing the GVL effect.12–14 Apart from ATG, the impact of the post-transplant immunosuppression on transplant outcomes in allogeneic HSCT following RIC has been poorly explored. While, the combination of CsA and a short course of methotrexate (MTX) after transplantation is considered as the gold standard for GVHD prophylaxis after conventional myeloablative allogeneic HSCT from HLA-identical siblings,15,16 there is no consensus on the optimal preventive regimen for GVHD prophylaxis after RIC allogeneic HSCT. However, MTX is associated with substantial toxicity, which includes delayed hematopoietic engraftment, worsened mucositis and renal toxicity, and it was thus replaced by mycophenolate mofetil (MMF) specifically in the setting of allogeneic HSCT following RIC.6,17 Piñana et al. compared the transplantation outcome of two non-ATG containing GVHD prophylaxis regimens, CsA + MTX (n=93) and CsA + MMF (n=52), after allogeneic HSCT from HLA-identical siblings following fludarabine-based RIC. Transplantation outcomes were similar in the two groups with the exception of a higher incidence of grade 2–4 mucositis with CsA + MTX.18
In this study, we retrospectively investigated the impact of the intensity of the GVHD prophylaxis on the post-transplant outcomes of a homogeneous cohort of 228 adult patients over 50 years old with de novo acute myeloid leukemia in first complete remission given haematopoietic stem cells from HLA-identical siblings following fludarabine and 2 days of intravenous busulfan (Flu-ivBu2) RIC. We analyzed the impact of the use of ATG with CsA compared to a combination of ATG and CsA + MTX or MMF versus CsA and MTX or MMF with no ATG as post-transplant GVHD prophylaxis.
Methods
Patients and data collection
This was a retrospective study performed by the Acute Leukemia Working Party of the European Group for Blood and Marrow Transplantation (EBMT), and approved by its scientific board. The EBMT registry is a voluntary working group of more than 500 transplant centers, which are required once a year to report all HSCT and their follow-up. The study included patients with de novo acute myeloid leukemia above 50 years old in first complete remission who underwent allogeneic HSCT with hematopoietic stem cells from HLA-identical siblings following Flu-ivBu2, between 2004 and 2014. Patients given ex vivo T-cell-depleted grafts were excluded. GVHD prophylaxis regimens were dependent on centers’ habits and protocols. Acute GVHD was graded using established criteria.19 Chronic GVHD was classified as limited or extensive according to usual criteria.20 For the purpose of this study, all necessary data were collected according to the EBMT guidelines, using the EBMT Minimum Essential Data forms. The list of institutions reporting data included in this study is provided in Online Supplementary Table S1.
Statistical analysis
The starting time for all endpoints was the date of the transplant. To evaluate the probability of relapse, patients dying from either direct toxicity of the procedure or any other cause not related to leukemia were censored. The non-relapse mortality was defined as death while in complete remission. Patients were censored at the time of relapse or of the last follow-up. Cumulative incidence curves were used for relapse incidence and non-relapse mortality in a competing risk setting, as death and relapse were competing events.21 For the estimates of the cumulative incidence of chronic GVHD, death was considered as a competing event. Overall and leukemia-free survival rates (starting from the date of transplant) were calculated using the Kaplan–Meier estimates. Univariate analyses were done using the Gray test for cumulative incidence functions and the log rank test for overall and leukemia-free survival. Associations of patient and graft characteristics with grade II–IV acute GVHD were evaluated using multivariate logistic regression, and with other outcomes (chronic GVHD, relapse, non-relapse mortality, leukemia-free survival, overall survival) by multivariable analyses, using Cox proportional hazards. Factors included in the Cox models included the type of GVHD prophylaxis, patients’ age, year of transplantation, time from diagnosis to transplantation, female donor to male recipient versus other gender combinations, and poor versus intermediate risk cytogenetics. All tests were two-sided. The type I error rate was fixed at 0.05 for determination of factors associated with time to event outcomes. Statistical analyses were performed with SPSS 19 (SPSS Inc, Chicago, IL, USA) and R 2.13.2 (R Development Core Team, Vienna, Austria) software packages.
Results
Patients and graft-versus-host disease prophylaxis
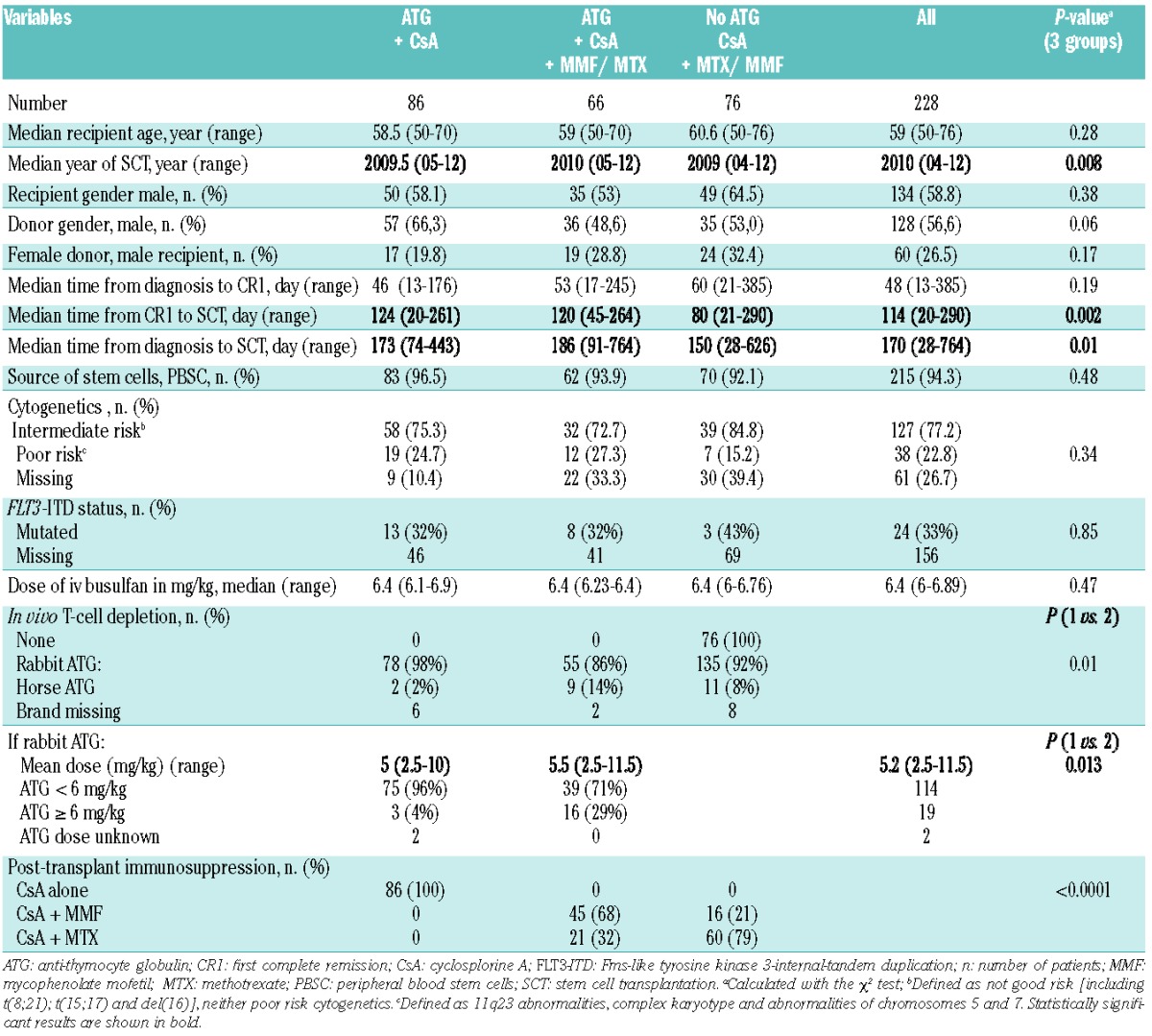
Between January 2004 and January 2012, 228 patients fulfilled the criteria for this study. Among those, three groups were established according to the GVHD prophylaxis regimen used, which was dependent on centers’ habits and protocols. The patients’ characteristics are summarized in Table 1. Briefly, 86 patients (38%) received ATG and CsA alone (ATG + CsA group), 66 patients (29%) received ATG and a combination of CsA and MMF (n=45) or MTX (n=21) (ATG + CsA + MMF/MTX) and 76 patients (33%) did not receive ATG but were given CsA and MTX (n=60) or MMF (n=16) (No ATG group). The median dose of intravenous busulfan received was 6.4 mg/kg in each group. Information on the brand of ATG was available for 144/152 patients (95%), among whom 92% had received thymoglobulin. Mean doses of thymoglobulin were 5 mg/kg in the ATG + CsA group and 5.5 mg/kg in the ATG + CsA + MMF/MTX group (P=0.013), with 4% and 29% of patients receiving doses >6 mg/kg, respectively (Table 1). Apart from GVHD prophylaxis, the three groups displayed minor differences. The median year of allogeneic HSCT was 2010 for the No ATG group and 2009 for the ATG + CsA + MMF/MTX group (P=0.008). Time from diagnosis to transplant was 150 versus >173 days, respectively (P=0.01) and median time from first complete remission to transplantation was 80 versus >120 days in the No ATG versus other groups, respectively (P=0.002). Other patient and donor characteristics did not differ between the three groups (Table 1). Cytogenetic data were available for 73.3% of the patients and missing in 10%, 33% and 39% of the ATG + CsA, ATG + CsA + MMF/MTX and No ATG groups, respectively. Among those with available data, the proportions of patients with poor cytogenetics were similar in the three groups. Fms-like tyrosine kinase 3-internal-tandem duplication status was available for 31% of the patients with similar proportions of mutated cases in the three groups.
Table 1.
Patients’ characteristics.
Impact of the type of graft-versus-host disease prophylaxis on engraftment and the incidence of acute and chronic graft-versus-host disease
Engraftment data and incidences of GVHD according to GVHD prophylaxis regimens are summarized in Table 2. All patients engrafted. However, time for engraftment was slightly different between the three groups with a median for absolute neutrophil count >0.5×109/L of 16.5 days (range, 1–25), 19 days (range, 4–27), and 17 days (range, 3–26) in the No ATG, ATG + CsA alone and ATG + CsA + MMF/MTX groups, respectively (P=0.03). We did not observe any significant impact of the type of GVHD prophylaxis on the 100-day incidence of grade II to IV acute GVHD, which occurred in 19.4%, 16.5% and 29.2% of the patients in the No ATG, ATG + CsA alone and ATG + CsA + MMF/MTX groups, respectively (P=0.15) (Table 2). Grade III-IV acute GVHD occurred in four (5.6%), nine (10.5%) and three (4.6%) patients in the No ATG, ATG + CsA alone and ATG + CsA + MMF/MTX groups, respectively (P=0.3).
Table 2.
Engraftment, acute GVHD and chronic GVHD according to GVHD prophylaxis.
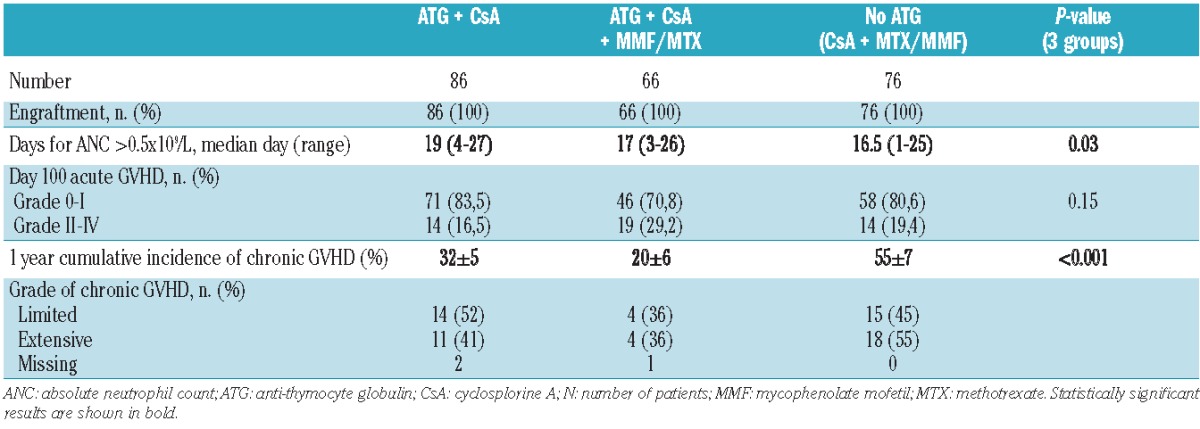
By contrast, the cumulative incidence of chronic GVHD at 1 year after transplantation was significantly higher in the No ATG group than in the ATG + CsA alone and ATG + CsA + MMF/MTX groups (55±7 % versus 32±5 % and 20±6 %, respectively, P<0.001). Grade of chronic GVHD was extensive in 55% of the cases in both No ATG and ATG + CsA + MMF/MTX groups and in 41% of the cases in the ATG + CsA alone goup (Table 2 and Figure 1).
Figure 1.
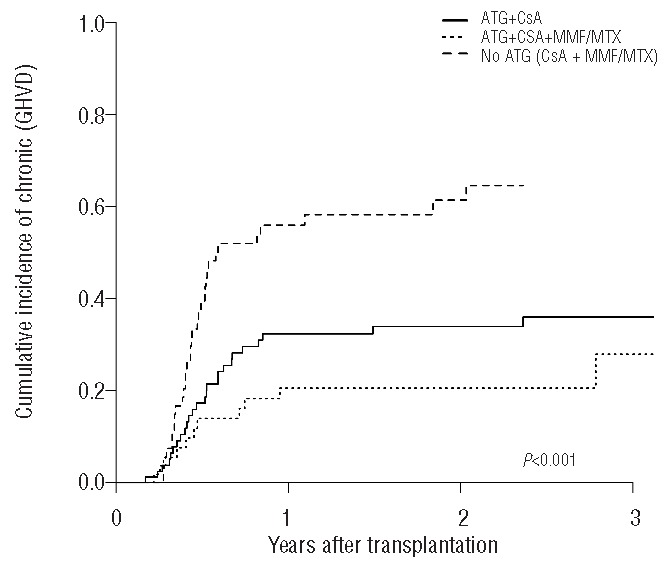
Cumulative incidence of chronic GVHD according to the GVHD prophylaxis in the three groups of patients (global P-value <0.001).
Non-relapse mortality, relapse incidence, leukemia-free survival and overall survival
The median follow up of the cohort was 19 (1–82) months. There was no difference between the groups in terms of non-relapse mortality with 2-year cumulative incidences of 15±4 %, 15 ± 5% and 23±6% in the ATG + CsA alone, ATG + CsA + MMF/MTX and No ATG groups, respectively, (P=0.23) (Table 3 and Figure 2A). The 2-year cumulative incidence of relapse was higher in the ATG + CsA + MMF/MTX group than in either the ATG + CsA alone or the No ATG group (48±7% versus 20±5% and 30±6%, respectively, P=0.01) (Table 3 and Figure 2B). Two-year leukemia-free survival was significantly better in the ATG + CsA alone group in comparison to the ATG + CsA + MMF/MTX group or the No ATG group (64±6%, 37±7 % and 47±7%, respectively (P=0.001) (Table 3 and Figure 2C). Similarly, the 2-year overall survival was better in the ATG + CsA alone group than in the other two groups (67±5% versus 37±7% for the triple immunosuppression group and 50±7% for the No ATG group, P=0.001) (Table 3 and Figure 2D). Causes of death included relapse, GVHD, infection in 16 (59%), three (11%) and four (15%) patients of the ATG + CsA alone group, respectively, 20 (69%), three (10%) and four (14%) patients of the ATG + CsA + MMF/MTX group, respectively, and 19 (54%), two (6%) and 13 (37%) patients of the No ATG group, respectively.
Table 3.
Transplant outcomes at 2 years after allogeneic hematopoietic stem cell transplantation according to the GVHD prophylaxis.

Figure 2.
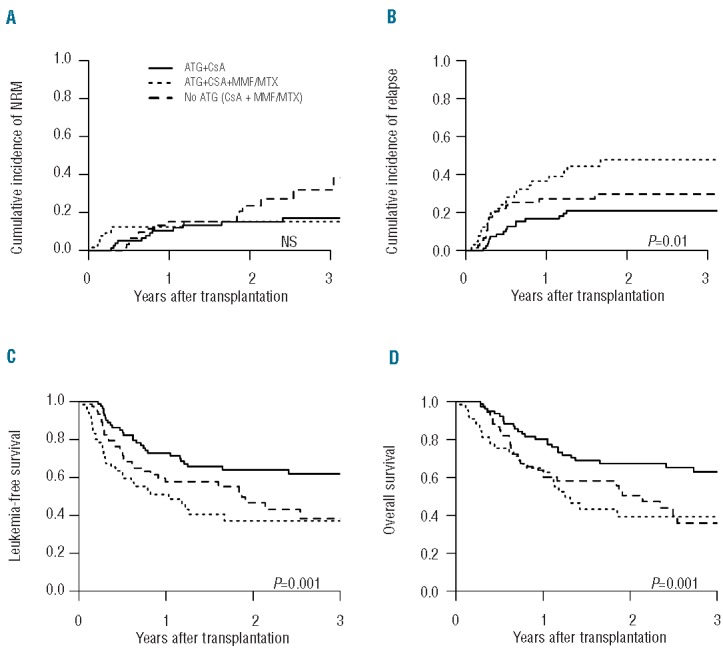
Transplant outcomes according to the GVHD prophylaxis. Cumulative incidence of (A) non-relapse mortality (NRM) (global P-value = 0.23), (B) relapse (global P-value = 0.01), (C) leukemia-free survival (global P-value = 0.001) and (D) overall survival (global P-value = 0.001) in the different GVHD prophylaxis groups as indicated.
Impact of anti-thymocyte globulin dose on transplant outcomes
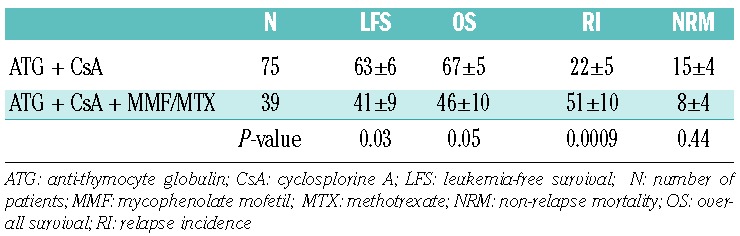
Among the 152 patients given ATG, the vast majority (n=135) received thymoglobulin, while 11 received horse ATG and in eight the brand of ATG was unknown. Among the patients who received thymoglobulin, patients in the ATG + CsA + MMF/MTX group received higher doses of thymoglobulin than those in the ATG + CsA group (mean dose of 5.5 mg/kg versus 5 mg/kg, respectively, P=0.013) (Table 1). Since transplant outcomes were worse in the triple immunosuppression group, we sought to determine whether the thymoglobulin dose could have had a role in this phenomenon. In univariate analysis, patients receiving a thymoglobulin dose below 6 mg/kg in the ATG + CsA group (n=75) had similar non-relapse mortality (P=0.44), reduced relapse incidence (P=0.0009) and improved overall survival (P=0.05) and leukemia-free survival (P=0.03) in comparison to those receiving similar doses of ATG in the ATG + CsA + MMF/MTX group (n=39) (Table 4). In addition, within the triple immunosuppression group, transplant outcomes were not significantly different in those treated with a thymoglobulin dose above or below 6 mg/kg (data not shown).
Table 4.
Transplant outcomes at 2 years after allogeneic hematopoietic stem cell transplantation in the two ATG groups treated with ATG <6 mg/kg.
Risk factors for chronic graft-versus-host disease, non-relapse mortality, relapse incidence, leukemia-free survival and overall survival
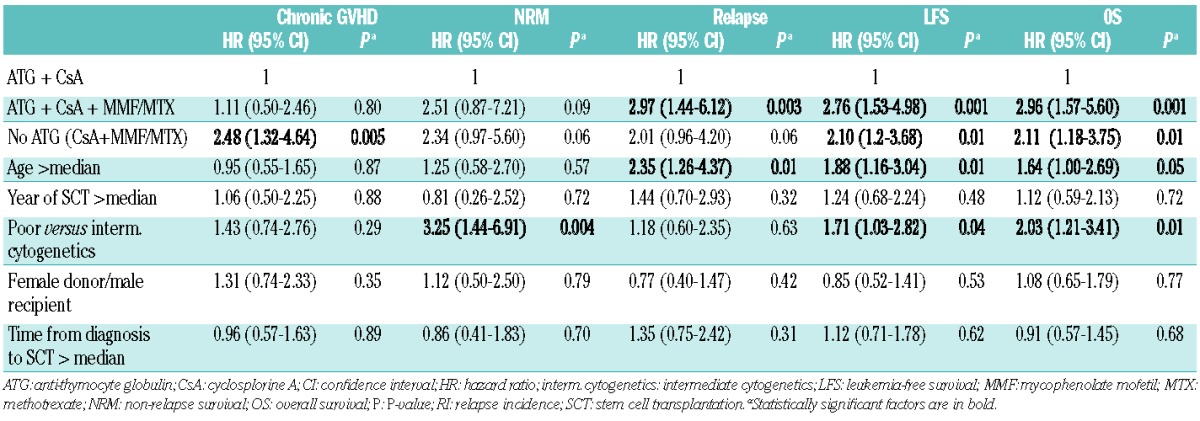
In multivariate analysis, the absence of ATG was the only risk factor associated with an increased risk of chronic GVHD [hazard ratio (HR) = 2.48; 95% confidence interval (CI) = 1.32–4.64] (P=0.005), while the risks of chronic GVHD in the two ATG groups were similar (HR=1.1; in the ATG + CsA + MMF/MTX group as compared to the ATG + CsA alone group, P=0.8) (Table 5). In comparison to ATG + CsA alone, the use of ATG + CsA + MMF/MTX led to a higher risk of relapse (HR=2.97, 95% CI=1.44–6.12, P=0.003). The use of ATG + CsA + MMF/MTX or the absence of ATG were associated with worse leukemia-free survival (HR=2.76, P=0.001 and HR=2.10, P=0.01, respectively) and overall survival (HR=2.96, P=0.001 and HR=2.11, P=0.01, respectively). The other factors that had a bearing on transplant outcomes were older age (above median) resulting in a higher relapse incidence (HR=2.35, P=0.01) and leading to worse leukemia-free survival (HR=1.88, P=0.01) and overall survival (HR=1.64, P=0.05), and poor cytogenetics associated with higher non-relapse mortality (HR=3.25, P=0.004) and, therefore, worse leukemia-free survival (HR=1.71, P=0.04) and overall survival (HR=2.03, P=0.01) (Table 5).
Table 5.
Multivariate analyses of chronic transplant outcomes.
Discussion
The long-lasting challenge of allogeneic HSCT in acute myeloid leukemia and other hematologic malignancies is to avoid toxicity and severe GVHD while maintaining the GVL effect. As the median age of patients with acute myeloid leukemia is >65 years and many of them have comorbidities and are, thus, ineligible for allogeneic HCST with myeloablative conditioning, reduced toxicity conditioning and RIC regimens were developed over the last decade. The Flu-ivBu2 RIC is widely used in this setting, essentially because of its low organ toxicity and non-relapse mortality and preserved anti-leukemia effect.1 The original Flu-ivBu2 RIC protocol used ATG and CsA alone as GVHD prophylaxis. However, the best GVHD prophylaxis remains a subject of debate. The increasing use of matched and mismatched unrelated donors has led to the addition of MMF or MTX to CsA in RIC regimens. Furthermore, the use of in vivo T-cell depletion is debatable, as the efficacy of RIC allogeneic HSCT is based on a powerful GVL effect, which is typically mediated by donor T and NK cells, rather than on high doses of radio-chemotherapy. Indeed, in a study from the CIBMTR, performed in patients with myeloid and lymphoid malignancies who underwent RIC allogeneic HSCT from related or unrelated donors, the use of ATG was associated with a higher risk of relapse and lower leukemia-free survival rate.11 In contrast, a similar recent EBMT study failed to detect either association.12
Because transplant outcomes are also dependent on recipient age, type of donor, disease risk and status at transplant,22,23 in order to evaluate the impact of GVHD prophylaxis on transplant outcomes more accurately, in the present study we limited the analysis to a very homogeneous population of patients above 50 years of age, transplanted for acute myeloid leukemia in first complete remission with an HLA-identical sibling after Flu-ivBu2 RIC. In this particular setting, the comparison of ATG and CsA GVHD prophylaxis to prophylaxis not containing ATG showed that the use of ATG was not linked to a higher risk of relapse in patients with equivalent cytogenetic risks. Most of the patients in this study had received thymoglobulin at a dose <6 mg/kg, and these results are consistent with the previously reported preserved GVL effect in patients treated with relatively reduced doses of ATG,12–14 in contrast with doses >10 mg/kg.3
As previously described,11,12 our study confirms a protective effect of ATG against chronic GVHD. No ATG was actually the only factor associated with an increased risk of chronic GVHD in a multivariate analysis. We did not observe an equivalent protective effect of ATG against acute GVHD. Moreover, the use of ATG is not an all or none phenomenon. The ATG dose also matters. Indeed, two recent studies reported that GVHD prophylaxis with a reduced dose of ATG of 2.5 mg/kg versus 5 mg/kg in Flu-ivBu2 RIC allogeneic HSCT with peripheral blood stem cells from matched related or unrelated donors was associated with an increased risk of acute and chronic GVHD.13,14 Collectively, these data confirm that the optimal dose of thymoglobulin in the Flu-ivBu2 RIC regimen is about 5 mg/kg.
The type and dose of post-transplant immunosuppression in the context of non-ATG-containing, fludarabine-based RIC from HLA-identical sibling donors was recently evaluated by Piñana et al.18 The authors found similar post-transplant outcomes with either a combination of CsA and MTX or of CsA and MMF. In our study, we also observed similar outcomes in the group of patients who received MTX or MMF and CsA without ATG (data not shown), but this group had a higher risk of chronic GVHD leading to worse survivals. In the context of ATG-containing regimens, the addition of MMF or MTX to CsA did not reduce the risk of acute GVHD, but significantly increased the risk of relapse, possibly as a consequence of the relatively reduced risk of chronic GVHD, leading to worse leukemia-free and overall survival. Chronic GVHD was previously reported as a very important process mediating the GVL effect, and with a strong correlation with reduced relapse rates, mainly in the RIC setting, compensating for the lower chemotherapy dose and, thus, the lower anti-leukemic effect.24 Interestingly, despite an increased risk of chronic GVHD due to the absence of ATG, the combination of CsA and MTX or MMF was also associated with a trend towards a higher risk of relapse and lower leukemia-free and overall survival rates, in comparison with the group treated with ATG and CsA. This emphasizes that early post-transplant immunosuppression after RIC in patients with acute myeloid leukemia in first complete remission has an important impact on the equilibrium between GVL and GVHD and, therefore, on final post-transplant outcomes. The use of intermediate doses of ATG (thymoglobulin at 5 mg/kg on average) + CsA alone provided the best outcomes with a 2-year leukemia-free survival rate of 64±6% and 2-year overall survival of 67±5%.
Besides indicating the role of immunosuppression, the results of our study pointed out a negative impact of older age (>60 years old) and poor cytogenetics on leukemia-free survival and overall survival. Older age was associated with a higher risk of relapse, even in this cohort of patients allografted in first complete remission. This is in accordance with previous studies demonstrating poorer results of anti-leukemic therapy in elderly patients with acute myeloid leukemia due to more aggressive biology of the disease, selection for more primitive clones, higher prevalence of multidrug resistance and lower treatment tolerability.25,26 Although the frequency of poor cytogenetics increases with age, this factor was not associated with a higher risk of relapse in this series of patients but was associated with increased non-relapse mortality. An absence of impact of poor cytogenetics on relapse incidence should be considered with caution because of the limited numbers of patients with documented poor cytogenetics.
We recognize that this study has several limitations. First, the study was retrospective and the reason for the choice of GVHD prophylaxis was not known but mainly dependent on the habits and protocols of each center. Second, the study included relatively small numbers of patients per group and cytogenetic data were imperfectly covered over the groups. However, the study was performed on a very homogeneous cohort of patients with acute myeloid leukemia older than 50 years, in first complete remission, receiving peripheral blood stem cells from HLA-identical siblings. Despite its limitations and the need for prospective randomized studies, the results of this study suggest that, in this particular setting, the best GVHD prophylaxis is the combination of an intermediate dose of ATG and CsA. Omission of ATG from the prophylactic regimen is associated with an increased risk of chronic GVHD without limiting the risk of relapse, while addition of MMF or MTX increased the risk of relapse.
Acknowledgments
MM would like to thank Pr Junia V. de Melo (University of Adelaide, Australia) for critical reading of the manuscript.
Footnotes
The online version of this article has a Supplementary Appendix.
Presented in part as an oral presentation at the 40th EBMT meeting in Milan in April 2014.
Authorship and Disclosures
Information on authorship, contributions, and financial & other disclosures was provided by the authors and is available with the online version of this article at www.haematologica.org.
References
- 1.Slavin S, Nagler A, Naparstek E, et al. Nonmyeloablative stem cell transplantation and cell therapy as an alternative to conventional bone marrow transplantation with lethal cytoreduction for the treatment of malignant and nonmalignant hematologic diseases. Blood. 1998;91(3):756–763. [PubMed] [Google Scholar]
- 2.Schetelig J, Thiede C, Bornhauser M, et al. Evidence of a graft-versus-leukemia effect in chronic lymphocytic leukemia after reduced-intensity conditioning and allogeneic stem-cell transplantation: the Cooperative German Transplant Study Group. J Clin Oncol. 2003;21(14):2747–2753. [DOI] [PubMed] [Google Scholar]
- 3.Mohty M, Bay JO, Faucher C, et al. Graft-versus-host disease following allogeneic transplantation from HLA-identical sibling with antithymocyte globulin-based reduced-intensity preparative regimen. Blood. 2003;102(2):470–476. [DOI] [PubMed] [Google Scholar]
- 4.Chevallier P, Szydlo RM, Blaise D, et al. Reduced-intensity conditioning before allogeneic hematopoietic stem cell transplantation in patients over 60 years: a report from the SFGM-TC. Biol Blood Marrow Transplant. 2012;18(2):289–294. [DOI] [PubMed] [Google Scholar]
- 5.Malard F, Cahu X, Clavert A, et al. Fludarabine, antithymocyte globulin, and very low-dose busulfan for reduced-intensity conditioning before allogeneic stem cell transplantation in patients with lymphoid malignancies. Biol Blood Marrow Transplant. 2011;17(11):1698–1703. [DOI] [PubMed] [Google Scholar]
- 6.McSweeney PA, Niederwieser D, Shizuru JA, et al. Hematopoietic cell transplantation in older patients with hematologic malignancies: replacing high-dose cytotoxic therapy with graft-versus-tumor effects. Blood. 2001;97(11):3390–3400. [DOI] [PubMed] [Google Scholar]
- 7.Giralt S, Estey E, Albitar M, et al. Engraftment of allogeneic hematopoietic progenitor cells with purine analog-containing chemotherapy: harnessing graft-versus-leukemia without myeloablative therapy. Blood. 1997;89(12):4531–4536. [PubMed] [Google Scholar]
- 8.Baron F, Labopin M, Niederwieser D, et al. Impact of graft-versus-host disease after reduced-intensity conditioning allogeneic stem cell transplantation for acute myeloid leukemia: a report from the Acute Leukemia Working Party of the European Group for Blood and Marrow Transplantation. Leukemia. 2012;26(12):2462–2468. [DOI] [PubMed] [Google Scholar]
- 9.Baron F, Maris MB, Sandmaier BM, et al. Graft-versus-tumor effects after allogeneic hematopoietic cell transplantation with nonmyeloablative conditioning. J Clin Oncol. 2005;23(9):1993–2003. [DOI] [PubMed] [Google Scholar]
- 10.Valcarcel D, Martino R, Caballero D, et al. Sustained remissions of high-risk acute myeloid leukemia and myelodysplastic syndrome after reduced-intensity conditioning allogeneic hematopoietic transplantation: chronic graft-versus-host disease is the strongest factor improving survival. J Clin Oncol. 2008;26(4):577–584. [DOI] [PubMed] [Google Scholar]
- 11.Soiffer RJ, Lerademacher J, Ho V, et al. Impact of immune modulation with anti-T-cell antibodies on the outcome of reduced-intensity allogeneic hematopoietic stem cell transplantation for hematologic malignancies. Blood. 2011;117(25):6963–6970. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Baron F, Labopin M, Blaise D, et al. Impact of in vivo T-cell depletion on outcome of AML patients in first CR given peripheral blood stem cells and reduced-intensity conditioning allo-SCT from a HLA-identical sibling donor: a report from the Acute Leukemia Working Party of the European Group for Blood and Marrow Transplantation. Bone Marrow Transplant. 2014;49(3):389–396. [DOI] [PubMed] [Google Scholar]
- 13.Crocchiolo R, Esterni B, Castagna L, et al. Two days of antithymocyte globulin are associated with a reduced incidence of acute and chronic graft-versus-host disease in reduced-intensity conditioning transplantation for hematologic diseases. Cancer. 2013;119(5):986–992. [DOI] [PubMed] [Google Scholar]
- 14.Devillier R, Crocchiolo R, Castagna L, et al. The increase from 2.5 to 5 mg/kg of rabbit anti-thymocyte-globulin dose in reduced intensity conditioning reduces acute and chronic GVHD for patients with myeloid malignancies undergoing allo-SCT. Bone Marrow Transplant. 2012;47(5):639–645. [DOI] [PubMed] [Google Scholar]
- 15.Storb R, Antin JH, Cutler C. Should methotrexate plus calcineurin inhibitors be considered standard of care for prophylaxis of acute graft-versus-host disease? Biol Blood Marrow Transplant. 2010;16(1 Suppl):S18–27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Storb R, Deeg HJ, Whitehead J, et al. Methotrexate and cyclosporine compared with cyclosporine alone for prophylaxis of acute graft versus host disease after marrow transplantation for leukemia. N Engl J Med. 1986;314(12):729–735. [DOI] [PubMed] [Google Scholar]
- 17.Mielcarek M, Martin PJ, Leisenring W, et al. Graft-versus-host disease after nonmyeloablative versus conventional hematopoietic stem cell transplantation. Blood. 2003;102(2):756–762. [DOI] [PubMed] [Google Scholar]
- 18.Pinana JL, Valcarcel D, Fernandez-Aviles F, et al. MTX or mycophenolate mofetil with CsA as GVHD prophylaxis after reduced-intensity conditioning PBSCT from HLA-identical siblings. Bone Marrow Transplant. 2010;45(9):1449–1456. [DOI] [PubMed] [Google Scholar]
- 19.Glucksberg H, Storb R, Fefer A, et al. Clinical manifestations of graft-versus-host disease in human recipients of marrow from HL-A-matched sibling donors. Transplantation. 1974;18(4):295–304. [DOI] [PubMed] [Google Scholar]
- 20.Shulman HM, Sullivan KM, Weiden PL, et al. Chronic graft-versus-host syndrome in man. A long-term clinicopathologic study of 20 Seattle patients. Am J Med. 1980;69(2):204–217. [DOI] [PubMed] [Google Scholar]
- 21.Gooley TA, Leisenring W, Crowley J, Storer BE. Estimation of failure probabilities in the presence of competing risks: new representations of old estimators. Stat Med. 1999;18(6):695–706. [DOI] [PubMed] [Google Scholar]
- 22.Harris AC, Ferrara JL, Levine JE. Advances in predicting acute GVHD. Br J Haematol. 2013;160(3):288–302. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Nash RA, Storb R. Graft-versus-host effect after allogeneic hematopoietic stem cell transplantation: GVHD and GVL. Curr Opin Immunol. 1996;8(5):674–680. [DOI] [PubMed] [Google Scholar]
- 24.Weisdorf D, Zhang MJ, Arora M, Horowitz MM, Rizzo JD, Eapen M. Graft-versus-host disease induced graft-versus-leukemia effect: greater impact on relapse and disease-free survival after reduced intensity conditioning. Biol Blood Marrow Transplant. 2012;18(11):1727–1733. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Appelbaum FR, Gundacker H, Head DR, et al. Age and acute myeloid leukemia. Blood. 2006;107(9):3481–3485. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Kantarjian H, O’Brien S, Cortes J, et al. Results of intensive chemotherapy in 998 patients age 65 years or older with acute myeloid leukemia or high-risk myelodysplastic syndrome: predictive prognostic models for outcome. Cancer. 2006;106(5): 1090–1098. [DOI] [PubMed] [Google Scholar]