

Prognosis of pediatric acute myeloid leukemia (AML) has improved significantly over the past two decades with survival rates now approaching 70%.1 Therapy consists of a limited number of intensive chemotherapy courses mainly based on cytarabine and anthracycline.2,3 Many pediatric late anthracycline cardiotoxicity studies have concerned heterogeneous diagnostic groups. Moreover, single childhood cancer studies were mainly conducted in acute lymphoblastic leukemia, whereas the highest doses of anthracycline are given in children with AML.4–6 We report here a prospective multi-centric study of late cardiotoxicity in 185 patients surviving childhood AML. All were treated after 1989 in French clinical trials using intensive chemotherapy alone or chemotherapy and allogeneic hematopoietic stem cell transplantation (HSCT).
L.E.A. (Leucémie Enfant & Adolescent) is a French prospective long-term follow-up program involving all childhood acute leukemia survivors treated in the participating centers since 1980. Details of the programm are provided elsewhere.7 As of 31 December 2011, 282 childhood AML survivors fulfilled the L.E.A. inclusion criteria and 218 (77.3%) of them agreed to participate. Among these 218, 185 were treated according to one of the 6 multicenter trial protocols ongoing in France after January 1989. All 185 had serial echocardiographic examination as part of their L.E.A. program, and all were included in the present study. All provided written informed consent. Cardiotoxicity was defined by either clinical symptoms of congestive heart failure or by an abnormal echocardiographic left ventricular function. Left ventricular function was considered abnormal when the shortening fraction (SF) was less than 28% or when the left ventricular ejection fraction (LVEF) was less than 55% on 2D echocardiography.8–10 Cardiotoxicity was classified as late when it started or persisted beyond one year after the completion of first-line treatment.9 Cumulative anthracycline doses used in each trial are described in the Online Supplementary Table S1, as well as the doxorubicin-equivalent doses using conversion factors of 0.83, 4.0 and 5.0 for daunorubicin, mitoxantrone and idarubicin, respectively.10,11 Assessment of health status, long-term late effects on health-related quality of life (QoL), and statistical analysis are described in the Online Supplementary Appendix.
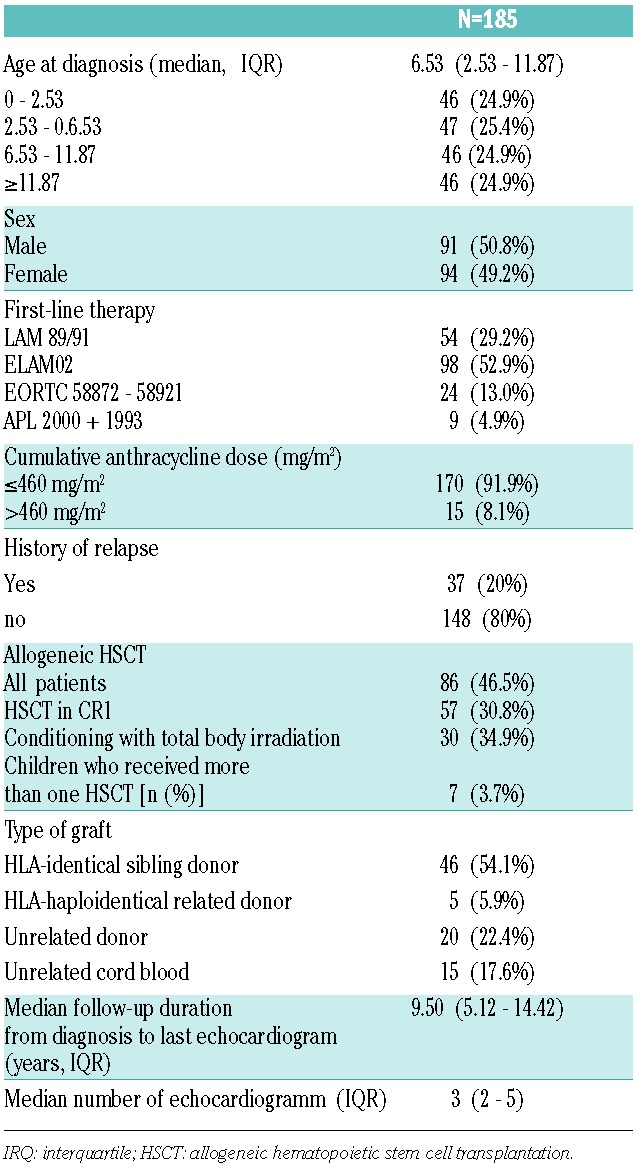
Characteristics of the study cohort are summarized in Table 1. Median age at the time of AML diagnosis and median follow-up duration to last cardiac evaluation were 6.53 and 9.5 years, respectively. Thirty-seven patients had a history of relapse. Median cumulative anthracycline dose was 372 mg/m2 (Online Supplementary Figure S1). Ninety-nine patients were treated by chemotherapy alone, whereas the other 86 patients also received HSCT (57 in first remission, 25 in second remission, and 4 in more advanced disease). Thirty children received total body irradiation (TBI), but only 10 among the 57 transplanted in first remission did so.
Table 1.
Patients characteristics.
Median number of echographic evaluations was 3 per patient. Subclinical cardiotoxicity (SCC) was observed in 23 of 185 patients (12.4%) at least once during their follow-up program. Median time from AML diagnosis to SCC detection was 4.40 years. In these 23 patients, the median value of the worst SF was 27% and the median value of the worst LVEF was 52. Only 3 of 23 patients had a worse SF value of less than 25% (2 had 20%; 1 had 24%). Six of 23 received anti-congestive therapy and none had cardiac transplantation. Five of those receiving anti-congestive therapy were still being treated at time of last evaluation, and 4 had more than 28% SF and more than 55% LVEF. Seventeen patients never received treatment: 11 had spontaneous improvement with more than 28% SF and more than 55% LVEF at last evaluation. Finally, at last cardiac evaluation, only 8 patients had an abnormal left ventricular function. Cumulative incidence (CI) of cardiotoxicity, estimated by the Kaplan-Meier method was 16% and 27% at 10 and 15 years, respectively (Figure 1A). CI of anti-congestive treatment at the same follow-up times was 5% and 7%.
Figure 1.
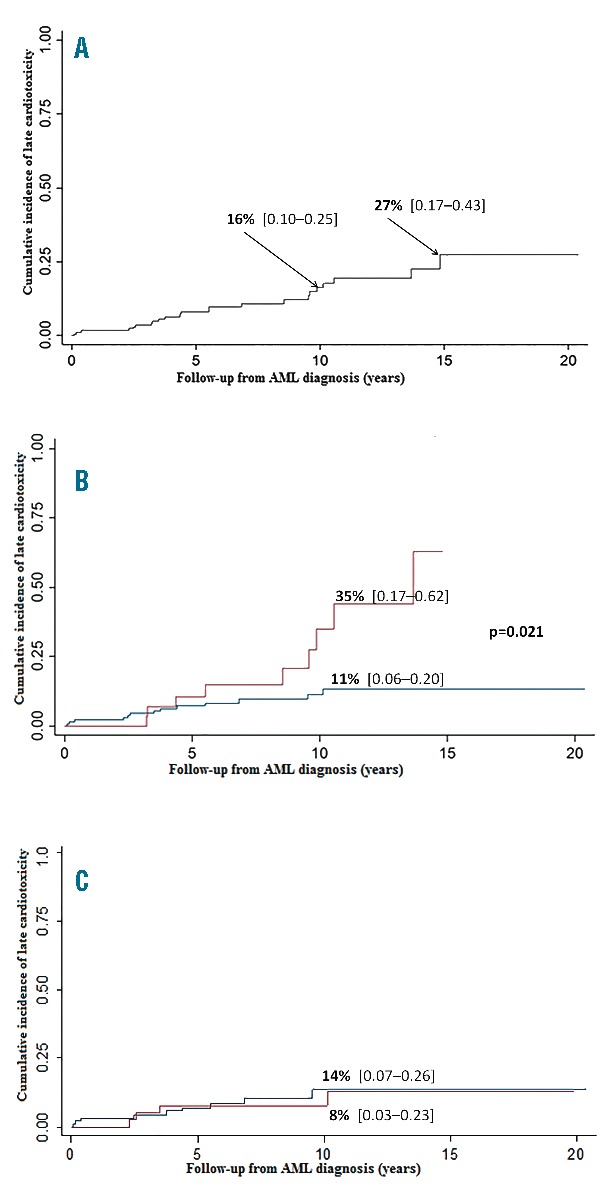
Cumulative incidence subclinical cardiotoxicity over time based on Kaplan-Meier estimates (A), for all patients (n=185); (B) for patients with (red line) or without (blue line) history of relapse (C) among 148 patients without history of relapse, cumulative incidence of SCC in 97 patients treated with chemotherapy alone (blue line) versus 51 patients with chemotherapy and HSCT (red line).
The risk of developing cardiotoxicity depended on a previous history of relapse and on the cumulative anthracycline dose. At ten years from diagnosis, CI was 35% versus 11% in patients with or without history of relapse (P=0.02) (Figure 1B). Among 148 patients without any history of relapse, 10-year CI of cardiotoxicity was 14% in 97 patients treated with chemotherapy alone versus 8% in 51 patients who underwent HSCT in first remission (NS, Figure 1C). In transplanted children, the risk was not modified by either a grade 2–4 acute or an extensive chronic graft-versus-host disease. The CI of anti-congestive treatment in these 148 patients who never experienced relapse was 3% at ten and 15 years. The value of 460 mg/m2 was identified as a threshold of cumulative dose of anthracycline with receiver operating characteristics (ROC) curve, with a sensitivity of 26.09%, a specificity of 94.44%, and an accuracy of 85.95%. The 10-year SCC estimated risk was 37% in patients treated with more than 460 mg/m2 and 15% in patients with less (P=0.02). History of relapse and a higher cumulative anthracycline dose were the only risk factors that proved significant in the univariate analysis (Online Supplementary Table S2). Both factors remained significant in the multivariate Cox regression analysis after including the following potential confounding variables: sex, age at AML diagnosis, HSCT in first complete remission and TBI (Tables 2 and 3). When distributing patients according to the cumulative number of long-term late effects, patients with SCC were significantly more severely impaired: 43.5% of them developed more than 2 other sequelae versus 13.8% of patients without SCC (Online Supplementary Figure S2). The mean number of late effects, excluding cardiac dysfunction, was 2.22+−0.29 in the first group versus 1.43+−0.09 in the second group (P=0.004). Among 73 patients who had reached adulthood at time of evaluation, 15 had subclinical cardiotoxicity and 58 did not. We did not detect any difference in the self-reported QoL between the two groups (Online Supplementary Table S3).
Table 2.
Risk factors for the occurrence of subclinical cardiotoxicity. Multivariate Cox model including history of relapse.
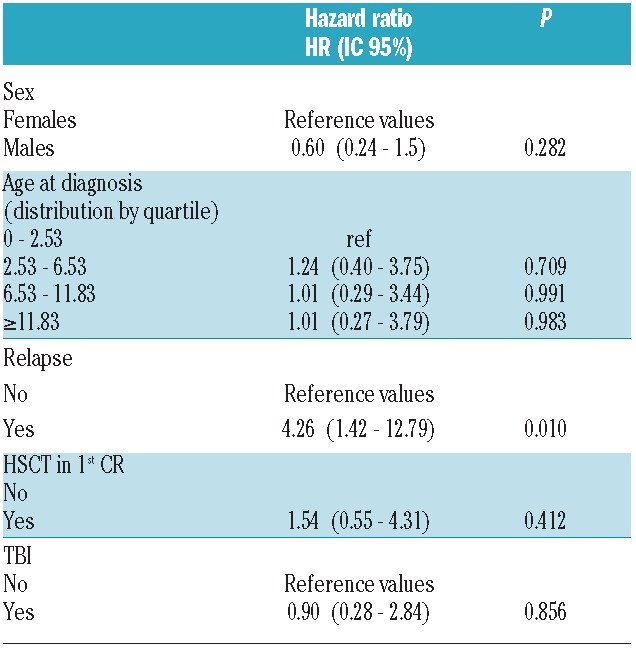
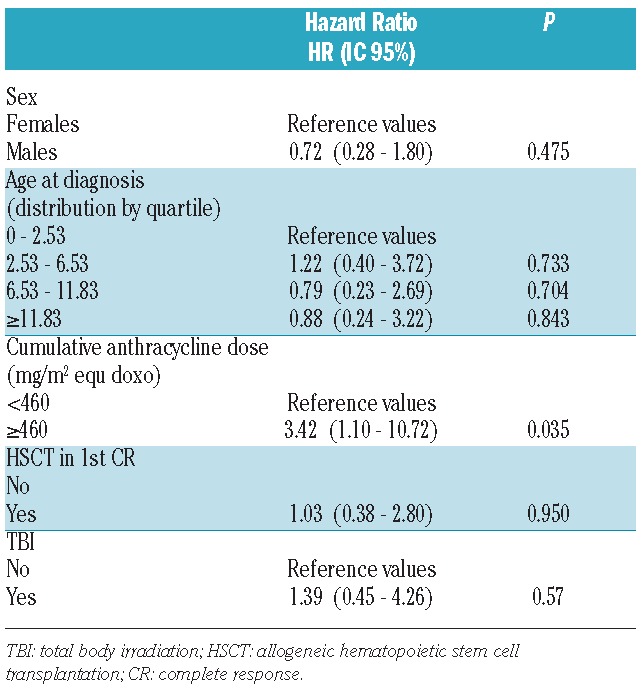
Table 3.
Risk factors for the occurrence of subclinical cardiotoxicity. Cox model including cumulative anthracycline dose.
Online Supplementary Table S4 provides details on the main late cardiotoxicity studies previously conducted in childhood AML survivors. In our study, overall prevalence of late cardiotoxicity was 12.4% resulting in a 16% 10-year CI. Furthermore, the risk was strongly dependent on the total amount of therapy: 10-year CI was 11% in patients who received first-line therapy alone compared to 35% in those who also required salvage therapy for relapsed disease. The same feature has already been published by Temming et al. who reported a 12% prevalence of late cardiotoxicity after first-line treatment only versus 37% after first-line treatment plus salvage therapy for relapse.12 The German group also underlined a high risk of late cardiotoxicity in patients who had been treated twice with anthracycline because of secondary AML, which is consistent with our results.13 In transplanted children, when our study was restricted to patients who never experienced leukemia relapse, we did not detect any difference in late cardiotoxicity between those who received HSCT during their first CR and those treated with chemotherapy only. Similar results have been published by Leung et al.14 Most of the children transplanted for AML in France since 1989 received busulfan and cyclophosphamide as conditioning regimen.15 Although a young age at diagnosis had been identified as a risk factor for cardiotoxicity in previous publications,9 this was not observed in our study, perhaps partly because in French AML trials the anthracycline dose was deceased in infants under one year of age. We also acknowledge that the statistical power of a risk factor analysis is limited by the relatively low number and mild severity of cardiotoxic events.
Because L.E.A. is a prospective cohort with serial health status evaluations, we were able to provide follow-up data after diagnosis of cardiomyopathy. Interestingly, only 6 among 23 patients with late cardiotoxicity required anti-congestive therapy. Fifteen among these 23 (including 4 of 6 who received therapy) had improvement and, at last L.E.A. evaluation, no longer met our echographic criteria for cardiomyopathy. This feature of transient cardiomyopathy occurrence has already been reported in the German as well as in the UK experience of childhood AML survivors’ late cardiotoxicity.12,13 Although potentially reassuring, this concept of possible improvement must be interpreted with caution because long-term persistence of such an improvement cannot be predicted and will require longer follow up. In addition, we cannot exclude the possibility that some apparent improvements were, in fact, due to underestimation of cardiac function in a previous echocardiogram.
Impairment in several domains of QoL has been described in childhood cancer survivors, but to the best of our knowledge, our study is the first to focus on the impact of late cardiac dysfunction. It is worthy of note that we did not detect any difference in QoL domains when comparing patients with or without late cardiac toxicity. This could appear surprising, but we have to consider that the QoL questionnaire assesses patients’ self-perceived health status. None of the patients with echocardiographic abnormality suffered from clinical heart failure and only a few required anti-congestive therapy. Moreover, more than half of patients detected with SCC had further improvement and normal cardiac function at last evaluation, which is when they filled in the QoL questionnaire.
Finally, the relatively low burden of cardiac complications described here should be interpreted in the context of a late complication whose prevalence and severity increase according to the length of post-therapy interval.9 Thus, although the median follow-up time between diagnosis and last evaluation was 9.5 years in this L.E.A study, an even longer follow-up duration is required.
Footnotes
Information on authorship, contributions, and financial & other disclosures was provided by the authors and is available with the online version of this article at www.haematologica.org.
References
- 1.Creutzig U, van den Heuvel-Eibrink MM, Gibson B, et al. Diagnosis and management of acute myeloid leukemia in children and adolescents: recommendations from an international expert panel. Blood. 2012;120(16):3187–3205. [DOI] [PubMed] [Google Scholar]
- 2.Fernandez HF, Sun Z, Yao X, et al. Anthracycline dose intensification in acute myeloid leukemia. N Engl J Med. 2009;361(13):1249–1259. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Kaspers GJ, Zwaan CM. Pediatric acute myeloid leukemia: towards high-quality cure of all patients. Haematologica. 2007;92(11):1519–1532. [DOI] [PubMed] [Google Scholar]
- 4.Lipshultz SE, Colan SD, Gelber RD, et al. Late Cardiac Effects of Doxorubicin Therapy for Acute Lymphoblastic Leukemia in Childhood. N Engl J Med. 1991;324(12):808–815. [DOI] [PubMed] [Google Scholar]
- 5.Nysom K, Holm K, Lipsitz SR, et al. Relationship between cumulative anthracycline dose and late cardiotoxicity in childhood acute lymphoblastic leukemia. J Clin Oncol. 1998;16(2):545–550. [DOI] [PubMed] [Google Scholar]
- 6.Sorensen K, Levitt G, Bull C, Chessells J, et al. Anthracycline dose in childhood acute lymphoblastic leukemia: issues of early survival versus late cardiotoxicity. J Clin Oncol. 1997;15(1):61–68. [DOI] [PubMed] [Google Scholar]
- 7.Berbis J, Michel G, Baruchel A, et al. Cohort Profile: The French Childhood Cancer Survivor Study For Leukaemia (LEA Cohort). Int J Epidemiol. 2014;0(0):1–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Kremer LC, van der Pal HJ, Offringa M, et al. Frequency and risk factors of subclinical cardiotoxicity after anthracycline therapy in children: a systematic review. Ann Oncol. 2002;13(6):819–829. [DOI] [PubMed] [Google Scholar]
- 9.Lipshultz SE, Adams MJ, Colan SD, et al. Long-term cardiovascular toxicity in children, adolescents, and young adults who receive cancer therapy: pathophysiology, course, monitoring, management, prevention, and research directions: a scientific statement from the American Heart Association. Circulation. 2013;128(17):1927–1995. [DOI] [PubMed] [Google Scholar]
- 10.Shankar SM, Marina N, Hudson MM, et al. Monitoring for cardiovascular disease in survivors of childhood cancer: report from the Cardiovascular Disease Task Force of the Children’s Oncology Group. Pediatrics. 2008;121(2):e387–396. [DOI] [PubMed] [Google Scholar]
- 11.Le Deley MC, Leblanc T, Shamsaldin A, Raquin MA, Lacour B, Sommelet D, et al. Risk of secondary leukemia after a solid tumor in childhood according to the dose of epipodophyllotoxins and anthracyclines: a case-control study by the Societe Francaise d’Oncologie Pediatrique. J Clin Oncol. 2003;21(6):1074–1081. [DOI] [PubMed] [Google Scholar]
- 12.Temming P, Qureshi A, Hardt J, et al. Prevalence and predictors of anthracycline cardiotoxicity in children treated for acute myeloid leukaemia: retrospective cohort study in a single centre in the United Kingdom. Pediatr Blood Cancer. 2011;56(4):625–630. [DOI] [PubMed] [Google Scholar]
- 13.Creutzig U, Diekamp S, Zimmermann M, et al. Longitudinal evaluation of early and late anthracycline cardiotoxicity in children with AML. Pediatr Blood Cancer. 2007;48(7):651–662. [DOI] [PubMed] [Google Scholar]
- 14.Leung W, Hudson MM, Strickland DK, et al. Late effects of treatment in survivors of childhood acute myeloid leukemia. J Clin Oncol. 2000;18(18):3273–3279. [DOI] [PubMed] [Google Scholar]
- 15.Michel G, Gluckman E, Esperou-Bourdeau H, et al. Allogeneic bone marrow transplantation for children with acute myeloblastic leukemia in first complete remission: impact of conditioning regimen without total-body irradiation–a report from the Societe Francaise de Greffe de Moelle. J Clin Oncol. 1994;12(6):1217–1222. [DOI] [PubMed] [Google Scholar]