

Abstract
Title
Comparative evaluation of metered-dose inhaler technique demonstration among community pharmacists in Al Qassim and Al Ahsa regions, Saudi Arabia.
Background
Patients rely on the information about use of proper inhaler technique when dispensed by community pharmacists however; several studies have shown that patients are unable to show correct inhalation technique. The aim of this study is to assess the ability of community pharmacists in Al Qassim region to demonstrate proper inhalation technique of metered dose inhaler and compare the baseline outcomes with a similar study at Al-Ahsa region.
Method
We approach 96 pharmacies in Al Qassim region as mock patient (Investigator). The investigator asks the Pharmacist to guide him about proper inhalation technique of metered dose inhaler. Investigator completes a standardized and validated checklist of 8 steps of inhaler device use immediately after leaving the pharmacy. Baseline data were compared between the two study groups et al. Ahsa and Al-Qassim for variables for effectiveness of pharmacist handling of patient queries.
Result
A total number of 96 community pharmacies were approached in five cities of the Al Qassim province in Saudi Arabia This study has found that majority (93.7%) of community pharmacists failed to demonstrate proper inhalation technique of pMDI inhaler.
Conclusion
The pharmacists demonstrated particularly poor skills involving steps for coordination of the actuation process with the mechanics of inhalation with MDI. The errors detected in this simple assessment session, if translated to patient self-medication errors, are potentially significant.
Keywords: pMDI, Community pharmacists, Inhalation technique, Saudi Arabia, Medication error, Asthma, COPD
1. Introduction
Asthma and chronic obstructive pulmonary disease are highly prevalent in the recent years (Gershon et al., 2010; Hamdan et al., 2013). About 20–25% prevalence rate of asthma exists in Saudi patients (Hamdan et al., 2013). The use of inhaled medications has advantage in the management of bronchial asthma, because of their greater efficacy and fewer adverse effects when compared with available oral medications (Osman et al., 2012; Hamdan et al., 2013). The most important advantage of inhaled therapy is the direct, localized delivery of a high concentration of drugs to the airways with minimal systemic side effects (Broeders et al., 2009). Improper use of inhalation device can lead to decrease in drug delivery and poor asthma control. This in turn, leads to frequent emergency visits (Broeders et al., 2009; Lindgren et al., 1987). The percentage of drug that reaches the lung after proper inhalation technique is only up to fifteen percent (Hanania et al., 1994). It is evident in many studies that pharmacists lack the knowledge of handling inhaler devices (Hamdan et al., 2013; Hanania et al., 1994; Osman et al., 2012). There are various types of inhalation devices available in the market. However, the most common aerosol drug delivery device is pressurized metered dose inhaler.
It is logical that patients get demonstration of proper inhalation technique when dispensed by community pharmacists. A study has been done in the Al Ahsa region of Saudi Arabia shows that pharmacists were found to have a poor recognition with the steps considered while using an inhaler (Khan and Azhar, 2013). In our study we evaluated the demonstration of inhalation technique of a pressurized metered dose inhaler by community pharmacists in the Al Qassim region, Saudi Arabia and compare the baseline status between these two regions.
2. Method
We have done a cross sectional observational study in the Al Qassim region of Saudi Arabia and data were collected from November 2013 till February 2014. Al Qassim province is one of the thirteen administrative provinces of Saudi Arabia. It is located in the center of Saudi Arabia approximately 400 km northwest of Riyadh the capital (Qassim at glance, 2014).
A total number of ninety-six community pharmacies of five cities that are Buraydah, Unayzah, Ar Rass, Al Badai and Bukayriyah were visited. The pressurized metered dose inhaler that we have selected is Ventolin® Inhaler that contains salbutamol. This study was approved by research and ethics board of Buraidah Private Colleges.
The mock patient that is actually investigator has visited these community pharmacies with pressurized metered dose inhaler that is Ventolin®. The investigator asked the community pharmacist to demonstrate the inhaler technique for him. Investigator observed the technique carefully and completed the validated checklist (Bryant et al., 2013) of 8 steps after leaving the pharmacy. Another step has been added after the checklist which states that pharmacist can ask to repeat the steps from patient after demonstration (Giraud and Roche, 2002; Knudsen, 2014). It helps the pharmacist to discover the problems that patient will face while using the product. The asthma management guidelines also recommend checking this step at each patient visit (EPR-3, 2007).
We did a comparative evaluation of metered-dose inhaler technique demonstration among community Pharmacists in Al Qassim and Al Ahsa regions. Al Ahsa is the major urban center in the eastern region of Saudi Arabia (Khan and Azhar, 2013).
2.1. Statistical analysis
Baseline data were compared between the two study groups et al. Ahsa and Al-Qassim for variables for effectiveness of pharmacist handling of patient queries.
The recommended checklist of metered dose inhaler is specified in Table 1.
Table 1.
Recommended checklist of metered dose inhaler.
| 1. Remove cap and shake the inhaler vigorously |
| 2. Breath out slowly and completely |
| 3. Hold the inhaler in the upright position |
| 4. Insert the mouthpiece into mouth between closed lips or up to 4 cm in front of the open mouth |
| 5. Depress the canister once and at the same time begin slow deep inhalation continue to total lung capacity |
| 6. Remove the inhaler with closed lips |
| 7. Hold breath for 10–15 s |
| 8. Wait for 20–30 s before starting the second puff |
| 9. Did your pharmacist ask to repeat the steps after demonstration? |
2.2. Ethics approval
This study was approved by research and ethics board of Buraidah Private Colleges, November 2013.
3. Results
A total number of 96 community pharmacies were approached in five cities of the Al Qassim province in Saudi Arabia. Majority of pharmacies are located in Buraydah (n = 67, 67.7%), 8 (8.3%) in Unayzah, 9 (9.3%) in Ar Rass, 7 (7.2%) in Bukayriyah and 5 (5.2%) in Al Badai refer Fig. 1. We observed the age group of these pharmacists. The 20–30 age groups of pharmacists are 50%, 30–40 are 42% and 40–50 are only 8% refer Fig. 2.
Figure 1.
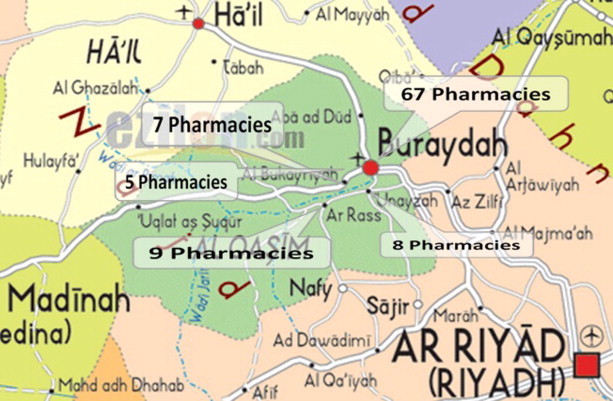
Geographic distribution of community pharmacies approached in the Al Qassim region.
Figure 2.
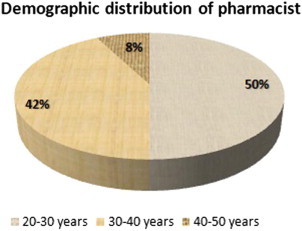
Demographic distribution of pharmacist.
Fig. 3 summarizes the demonstration of pressurize metered dose inhaler technique demonstration by pharmacists. The percentage of pharmacists who performed correct steps are, step 1 (55.4%), step 2 (46.7%), step 3 (71.5%), step 4 (72.8%), step 5 (63%), step 6 (55.4%), step 7 (33.7%), step 8 (10.9%). Only 7.2% of pharmacists demonstrated step 1–8 while just 2.1% of pharmacist demonstrated step 1–9 refer Fig. 4.
Figure 3.
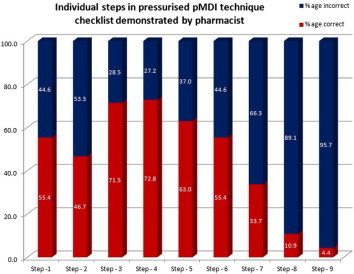
Individual steps in pressurized pMDI technique checklist demonstrated by pharmacist.
Figure 4.
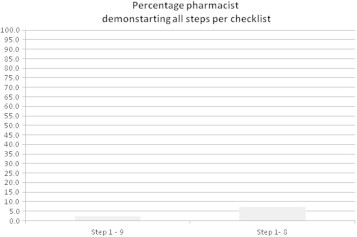
Percentage pharmacist demonstrating all steps per checklist.
Baseline data were compared between the two study groups et al. Ahsa and Al-Qassim for variables for effectiveness of pharmacist handling of patient queries. There was no significant difference between the two studies; refer Fig. 5.
Figure 5.
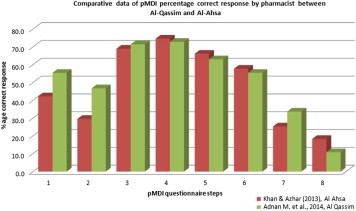
The MDI stepwise comparison of this study with Khan and Azhar (2013) Al Ahsa and our study.
4. Discussion
This study has found that majority (93.7%) of community pharmacists failed to demonstrate proper inhalation technique of pMDI inhaler. In this study only 7.3% of pharmacists have demonstrated the proper standardized technique of using pressurized metered dose inhaler whereas only 2.1% pharmacists correctly demonstrated the modified criteria (include step 9) of MDI. The criteria of grading system (Lenney et al., 2000) have been used to understand the knowledge of pharmacists to demonstrate the technique and its effect on aerosol drug delivery. The optimal delivery represents grade A (explained step 1–8), grade B (explained step 5–7) shows some delivery and Grade C is those pharmacists who are unable to explain most of the steps (step 2–7) indicating little or no delivery of the drug to the target point. In this study it was found that 7.3% of pharmacist’s fall in grade A category, 28.1% in grade B and grade C are15.2%. In grade C most of pharmacists were just told to press the canister and take two puffs. One of the most important steps is neglected by pharmacists while dispensing the inhalers. This study has added an additional step (step 9) according to the guidelines (EPR-3, 2007; GINA, 2009) recommending to ask this step to ensure patient understanding of the inhaler technique.
There are a number of studies that have been done to assess the demonstration of proper inhalation technique by pharmacists. In one study about 105 community pharmacists had been approached, out of which only 1 pharmacist (0.9%) was able to demonstrate the technique properly (Osman et al., 2012). Another study (Mickle et al., 1990) evaluated pharmacist practice in patient education when dispensing a metered-dose inhaler. The result shows that only 1 (1.9%) of the 52 pharmacists demonstrated MDI inhalation technique correctly. (Hounkpati et al., 2007) did an assessment of pharmacist’s understanding of the inhalation technique. It revealed that only 27.4% of pharmacists gave a correct answer for all the steps involved.
Community pharmacists are last health care provider to see the patients so it places them at an ideal position to teach inhaler technique to them. Various studies have been done on asthma education given by community pharmacists. In one study the community pharmacists were provided training and then evaluated the impact of pharmacist teaching on patients; it showed reduced hospitalization and improves inhaler technique (Cordina et al., 2001). Similar results have been found in another study that showed improved inhaler technique as a result of pharmacist counseling (Basheti et al., 2005). Another study has used interactive tele-pharmacy video counseling, using compressed video, connecting adolescents in schools with pharmacists; this study showed an improvement in inhaler technique (Bynum et al., 2001). Moreover, organizing asthma education session by pharmacists, physicians or nurses can serve as best adjunct to routine care of the asthmatic patients (Kohler et al., 1995).
In the light of these experiences, the community pharmacists should be given brief instructional sessions and training that may improve the quality of demonstration by them. Patients must be reeducated about proper inhalation technique at each visit to maintain adequate compliance. Educational approaches, such as the use of multimedia, pamphlets and medication information leaflets should be given to the patients in their local language. Finally, inhalation technique should be assessed by direct observation after expert instruction.
5. Conclusion
This study demonstrates that there is a gradual improvement in providing information by pharmacists about handling of MDI as compared to earlier studies in the region. Although the identified shortcomings can be improved by accepting the responsibility and improving strategies by using video counseling, providing brochures in local language, attending training sessions to achieve best practice or to overcome any barriers.
6. Recommendations
-
I.
The community pharmacists should learn to use interactive video counseling techniques to improve their skills and facilitate the use of these resources in patient counseling.
-
II.
The community pharmacists must ask the patient to repeat the steps after demonstration.
-
III.
Pharmacists should give more time for counseling and give pamphlet in local language to those patients who are going to use the inhalation device for the first time.
Acknowledgment
We would like to thank Mr. Javed for supporting this research by providing logistic support.
Footnotes
Peer review under responsibility of King Saud University.
References
- Basheti I.A., Reddel H.K., Armour C.L., Bosnic-Anticevich S.Z. Counseling about turbuhaler technique: needs assessment and effective strategies for community pharmacists. Respir. Care. 2005;50(5):617–623. [PubMed] [Google Scholar]
- Broeders M.E., Sanchis J., Levy M.L., Crompton G.K., Dekhuijzen P.N. The ADMIT series–issues in inhalation therapy. 2. Improving technique and clinical effectiveness. Prim. Care Respir. J. 2009;18(2):76–82. doi: 10.4104/pcrj.2009.00025. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bryant L., Bang C., Chew C., Balk S., Wisernan D. Adequacy of inhaler technique used by people with asthma or chronic obstructive pulmonary disease. J. Prim. Health Care. 2013;5(3) [PubMed] [Google Scholar]
- Bynum A., Hopkins D., Thomas A., Copeland N., Irwin C. The effect of telepharmacy counselling on metered-dose inhaler technique among adolescents with asthma in rural Arkansas. Telemed. J. E-Health. 2001;7(3):207–217. doi: 10.1089/153056201316970902. [DOI] [PubMed] [Google Scholar]
- Cordina M., McElnay J.C., Hughes C.M. Assessment of a community pharmacy-based program for patients with asthma. Pharmacotherapy. 2001;21(10):1196–1203. doi: 10.1592/phco.21.15.1196.33894. [DOI] [PubMed] [Google Scholar]
- EPR-3, 2007. Expert panel report 3: national asthma education and prevention program. Guidelines for the Diagnosis and Management of Asthma. Available from: http://www.nhlbi.nih.gov/guidelines/asthma/asthgdln.pdf.
- Gershon A.S., Wang C., Wilton A.S., Raut R., To T. Trends in chronic obstructive pulmonary disease prevalence, incidence, and mortality in Ontario, Canada, 1996 to 2007: a population-based study. Arch. Intern. Med. 2010;170(6):560–565. doi: 10.1001/archinternmed.2010.17. [DOI] [PubMed] [Google Scholar]
- Global Initiative for Asthma (GINA), 2009. Global strategy for asthma management and prevention. Available from: http://www.ginasthma.org [updated 2009].
- Giraud V., Roche N. Misuse of corticosteroid metered-dose inhaler is associated with decreased asthma stability. Eur. Respir. J. 2002;19(2):246–251. doi: 10.1183/09031936.02.00218402. [DOI] [PubMed] [Google Scholar]
- Hamdan A.L., Ahmed A., Abdullah A.L., Khan M., Baharoon S., Salih S.B., Al-Muhsen S. Improper inhaler technique is associated with poor asthma control and frequent emergency department visits. Allergy Asthma Clin. Immunol. 2013;9(1):8. doi: 10.1186/1710-1492-9-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hanania N.A., Wittman R., Kesten S., Chapman K.R. Medical personnel’s knowledge of and ability to use inhaling devices: metered-dose inhalers, spacing chambers, and breath-actuated dry powder inhalers. Chest. 1994;105(1):111–116. doi: 10.1378/chest.105.1.111. [DOI] [PubMed] [Google Scholar]
- Hounkpati A., Glakar C.A., Gbadamassi A.G., Adjoh K., Balogou K.A., Tidjani O. Attitudes of private pharmacists in the management of asthma patients in Lomé. Int. J. Tuberc. Lung Dis. 2007;11(3):344–349. [PubMed] [Google Scholar]
- Khan T.M., Azhar S. A study investigating the community pharmacist knowledge about the appropriate use of inhaler, Eastern Region AlAhsa, Saudi Arabia. Saudi Pharm. J. 2013;21(2):153–157. doi: 10.1016/j.jsps.2012.07.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Knudsen, D.S., 2014. Asthma patient counseling: join the pharmacist revolution. [online] Available at: http://www.pharmacytimes.com/publications/issue/2007/2007-04/2007-04-6402 (accessed 11.02.14).
- Kohler C.L., Davies S.L., Bailey W.C. How to implement an asthma education program. Clin. Chest Med. 1995;16(4):557–565. [PubMed] [Google Scholar]
- Lenney J., Innes J.A., Crompton G.K. Inappropriate inhaler use: assessment of use and patient preference of seven inhalation devices. EDICI. Respir. Med. 2000;94(5):496–500. doi: 10.1053/rmed.1999.0767. [DOI] [PubMed] [Google Scholar]
- Lindgren S., Bake B., Larsson S. Clinical consequences of inadequate inhalation technique in asthma therapy. Eur. J. Respir. Dis. 1987;70(2):93–98. [PubMed] [Google Scholar]
- Mickle T.R., Self T.H., Farr G.E., Bess D.T., Tsiu S.J., Caldwell F.L. Evaluation of pharmacists’ practice in patient education when dispensing a metered-dose inhaler. DICP. 1990;24(10):927–930. doi: 10.1177/106002809002401003. [DOI] [PubMed] [Google Scholar]
- Osman, A., Ahmed Hassan, I.S., Ibrahim, M.I.M., 2012. Are Sudanese community pharmacists capable to prescribe and demonstrate asthma inhaler devices to patrons? A mystery patient study. Pharm. Pract. (Internet) 10(2), 110–115. [DOI] [PMC free article] [PubMed]
- “Qassim at Glance”. Qassim University. QU, n.d. Web. 02 Feb. 2014. <www.qu.edu.sa>.