

Abstract
Purpose
This pilot study tested whether FiberWire provides similar protection to steel wire against repair displacement in patella fractures.
Methods
Thirteen cadaver knees were cyclically loaded with 10 cycles (0–90° flexion) and fracture displacement was recorded. Fixation methods were also tested in load to failure (>3 mm displacement).
Results
There was no difference between wire types in fracture displacement (1.4 mm ± 0.33 mm vs 1.2 mm ± 0.34 mm, respectively; p = 0.418) or in the load to failure (714.7 N ± 110.9 N vs 744.5 N ± 92.8 N, respectively; p = 0.360).
Conclusion
FiberWire provides similar protection to steel wire against repair displacement after fixation of patellar fractures.
Keywords: Knee, Patella, Fracture, Fixation
1. Introduction
The patella is of great importance to the knee extensor mechanism, and serves as a fulcrum over which forces are directed during knee extension. In traumatic injuries to the knee, the patella may be fractured. Patella fractures comprise approximately 1% of all fractures.1 Among the several types of patella fractures, transverse fractures are the most common. Current treatment of displaced transverse patellar fractures consists of open reduction and internal fixation to restore extensor continuity and articular congruity. Two common techniques consist of 316L stainless steel wire in modified anterior tension bands (MATB) placed through cannulated screws or tension bands around Kirschner wires (K-wires). When compared to K-wires, cannulated screws have been shown to provide more resistance to patella fracture displacement particularly in knee extension.2 The tension bands provide resistance to displacement during flexion.2 Over time, however, steel wire fixation can break, can cause painful irritation to the soft tissues of the knee, can migrate and may need to be removed in as many as 53% of patients.3,4 These problems with stainless steel wire have prompted the use of alternative materials such as braided suture for patella fracture fixation in place of steel wire.
There have been several studies that have examined the biomechanical properties of braided suture in patella fracture fixation.5–7 However, there is little biomechanical research of cannulated screws coupled with braided suture for patellar fracture repair. This is unfortunate, because this combination of materials may afford comparable stability of the fracture during loading compared with steel wire techniques. In this study, we have addressed this deficit in the literature by performing an experimental pilot study to compare the fixation strength of # 5 FiberWire (ultra-high molecular weight polyethylene and polyester braided suture) to 18-gage stainless steel wire using an MATB through stainless steel cannulated screws. This study was designed to test the hypothesis that FiberWire fixation through cannulated screws is not inferior in load to failure and cyclic loading fracture displacement compared to stainless steel wire with cannulated screw fixation while conferring the benefit of having fewer intrinsic problems such as breakage requiring operative removal.
2. Materials and methods
2.1. Specimens
This study used a patella fracture cadaver model modified from Carpenter et al2 Thirteen fresh frozen cadaver knees were used. This study was approved by the University of Florida Institutional Review Board and informed consent was not obtained due to the de-identification of the cadaver specimens used in this study.
All knees were thawed before testing and the anterior skin and subcutaneous tissues were removed. Each knee had no history of significant knee joint trauma or knee extensor mechanism injury. Each knee was cut to retain approximately 15 cm of distal femur and proximal tibia. To create transverse patella fractures, an oscillating saw was used to cut the patella outer cortex down to the far cortex subchondral bone. The osteotomy was completed with an osteotome.
2.2. Experimental conditions
Fractures were reduced anatomically with reduction clamps. Once reduced, two parallel 4.0 mm cannulated screws were placed across the fracture site. The two fixation material conditions were then tested: 1) FiberWire, or 2) stainless steel wire in figure-eight formation to create tension bands to secure the fracture. Anatomic reduction was confirmed visually and radiographically as shown in Fig. 1.
Fig. 1.

Lateral X-ray shows patella fracture with FiberWire tension band fixation.
The testing apparatus is shown in Fig. 2. Once fixation was complete, each knee was placed onto a custom made jig. Each femur was clamped in the jig parallel to the ground. The jig allowed the knees to freely move through a range of motion from 90° of flexion to full extension. The quadriceps tendon was clamped and attached to the mechanical testing machine (MiniBionix, MTS Systems, Eden Prairie, MN) via a steel cable routed around a pulley. The mechanical testing machine allowed for controlled application and measurement of known forces. A standard 4.5 kg weight was attached to each knee 14 cm below the joint line, to simulate the weight of an average adult lower leg and foot. Each knee had a measuring guide attached as a distance reference in the proximal fracture fragment. The order chosen for the first mode of fixation for each knee with steel wire or FiberWire was chosen randomly. The knees were then test first in nondestructive cyclic loading.
Fig. 2.
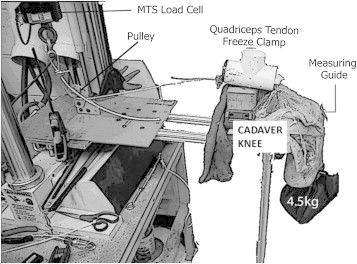
Image of testing apparatus for testing FiberWire and steel wire conditions for patellar fracture repair displacement and load to failure.
2.3. Fracture displacement
All knees were placed through 10 loading cycles to determine fracture repair displacement. During each load cycle, between 30 and 400 N was applied to each specimen via the quadriceps clamp at a fixed rate of 50 N/s. Using ImageJ software,8 the maximum fracture displacement was calculated for each knee cycle using the attached measuring guide. After each knee was cycled, the MATB were removed and replaced with the alternate mode of fixation.
2.4. Load to failure test
The load to failure test was performed for each knee once the final cyclic loading test was complete. It has been shown in previous studies that the maximal three point bending stress occurs around 45° of flexion.9 Thus with the knee locked in 45° of flexion, the quadriceps tendon was tensioned increasingly with the MTS device until failure occurred. The force was recorded from the testing machine at the time of failure. Failure was defined in this study as fracture displacement of greater than 3.0 mm.
2.5. Statistical analysis
Statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS; v.21.0). Equality of variance was tested using Levene's test, and normality of data was tested using the Kolmogorov–Smirnov test. Data were normally distributed and had equal variance. Paired sample T-tests were performed, where the grouping variable was the experimental condition for fracture fixation (FiberWire, steel wire) and the dependent variables were the fracture repair displacement and load to failure. To determine whether the sequence of testing conditions affected the results, a univariate analysis of variance was performed where the condition and order were independent variables and the fracture repair displacement and load to failure were the dependent variables. Data are reported in means and standard deviation (SD). Significance was established at p < 0.05 for all statistical tests.
3. Results
A total of 13 knees were tested with cyclic knee extensions for the steel wire group and 12 knees in the FiberWire group. One of the knees lost screw purchase during removal of the steel wire so it could not be retested with FiberWire.
Fig. 3 illustrates the results of the fracture repair displacement with the cyclic knee extension testing. This test revealed an average displacement of 1.4 mm ± 0.33 mm for the FiberWire condition and 1.2 mm ± 0.34 mm for the steel wire condition (p = 0.418). None of the knees had over 2 mm of displacement in the cyclic loading. Fig. 4 illustrates the results from the load to failure testing. There was no statistically significant difference in the load to failure tests for the two experimental conditions (p = 0.360). The steel wire condition resulted in a load to failure of 744.5 N ± 92.8 N and the FiberWire condition resulted in a load to failure of 714.7 N ± 110.9 N. For each condition, there was no significant difference between specimens depending on sequence tested.
Fig. 3.

Comparison of fracture repair displacement values with FiberWire and steel wire conditions with cyclic knee extensions. Values are means ± SD.
Fig. 4.

Comparison of load to failure values with FiberWire and steel wire conditions. Values are means ± SD.
4. Discussion
In this pilot study, we compared fracture fixation techniques with anterior tension band through cannulated screws using FiberWire and stainless steel wire. Our hypothesis was that stainless steel wire fixation would produce similar responses as the FiberWire fixation for cyclic loading fracture displacement and load to failure tests. The study results demonstrate no significant difference between the groups in load to failure and cyclic loading fracture displacement and the data support our hypothesis. These results are consistent with other studies that show that non-absorbable suture is comparable to metal wire in strength.5–7 Therefore, the FiberWire can provide similar protection as steel wire in protecting against repair displacement and strength during knee extensor loading. Subsequent larger clinical studies can be powered from these data.
Multiple studies have compared different patella fracture fixation constructs. In a cadaver model, Patel et al6 compared fixation of patella fractures with braided polyester suture in tension bands versus steel wire tension bands and found no significant difference in fracture displacement between the groups. Tension band wiring with K-wires or cannulated screws for patella fractures has been recommended by many studies.2,10,11 While there has been successful fracture union with fixation of patella fractures with tension bands, there are often complications with these procedures. One of the most common complications is need for removal of the hardware. For example, Hoshino et al12 studied complications following tension band fixation with screws versus K-wires and demonstrated that patients treated with K-wires were twice as likely to need hardware removal. Because of the small amount subcutaneous tissue over the patella, metal wires can cause anterior knee irritation and subsequent anxiety for patients on postoperative imaging when these wires break. This concern has prompted some surgeons to use non-absorbable suture in place of steel wire.11,12 In a biomechanical study, Hughes et al5 compared suture tension bands to steel wire tension bands. The authors found that the suture tension bands that used modified Wagoner's knots were stronger by 13.6% in the tension tests compared to the steel wire tension bands (8.3 mV versus 7.3 mV with interfragmentary gaps of 0.24 mm and 0.36 mm, respectively). In pilots for our study, we attempted to use Hughes's Wagoner's knot but found the knot difficult to reproduce. Instead, we chose a surgeons knot because this knot is easy to create and would likely be the most translatable and generalizable for use by orthopedic surgeons.
In the clinical setting, suture fixation has shown promise for long-term success. A review of over 400 patients treated for patellar fracture with tension bands by Hoshino et al12 showed no increase in fixation failure with the use of non-absorbable suture through cannulated screws. Gosal et al13 found that knees that were fixed with metal wires were six times more likely to need reoperation and more likely to have painful hardware compared to those treated with suture fixation.
5. Study limitations
This pilot study has some limitations that deserve comment. In our experimental set up, the force applied to the quadriceps tendon required for the knee to completely extend was higher than other studies have reported. Specifically, our pilot testing revealed that 400 N of force was required to extend the knee. Other investigators have found that ∼350 N was required to get the knee into full extension, and there an increase in force was needed to extend the knee over the last 15°.14 The load of 400 N was chosen because we wanted to ensure that all knees would have complete extension/flexion cycles from 0 to 90°. While we were able to perform the full test on each cadaveric specimen, the higher forces may therefore have contributed to our slightly higher fracture displacements with cyclic loading compared to other studies. Another criticism could be that bone mineral density was not measured on the cadavers. Halvorson et al15 studied the axial pullout with screws in the spine and found decreased pullout strength in osteoporotic bone compared to healthy normal bone.
6. Conclusion
Our pilot study results showed that no statistical difference existed for fracture repair displacement or load to failure tests between FiberWire and stainless steel wire when used with cannulated screws for the fixation of patellar fractures. The strength of fixation between the two materials under these conditions was found to be comparable. Hence, we support the use of FiberWire in the treatment of patellar fractures in place of stainless steel to avoid the need for hardware removal or painful irritation of soft tissues of the knee.
Source of funding
The authors gratefully thank Arthrex (Naples, Florida) who kindly donated cadaver knee specimens and supplies to complete this study.
Conflicts of interest
All authors have none to declare.
Acknowledgments
The authors gratefully thank Arthrex (Naples, Florida) who kindly donated cadaver knee specimens, FiberWire and stainless steel screws to complete this study.
References
- 1.Boström A. A study of 422 patellar fractures. Acta Orthop Scand. 1972;143:1–80. doi: 10.3109/ort.1972.43.suppl-143.01. [DOI] [PubMed] [Google Scholar]
- 2.Carpenter J.E., Kasman R.A., Patel N., Lee M.L., Goldstein S.A. Biomechanical evaluation of current patella fracture fixation techniques. J Orthop Trauma. 1997;11:351–356. doi: 10.1097/00005131-199707000-00009. [DOI] [PubMed] [Google Scholar]
- 3.Lebrun C.T., Langford J.R., Claude Sagi H. Functional outcomes after operatively treated patella fractures. J Orthop Trauma. 2012;26:422–426. doi: 10.1097/BOT.0b013e318228c1a1. [DOI] [PubMed] [Google Scholar]
- 4.Smith S.T., Cramer K.E., Karges D.E., Watson J.T., Moed B.R. Early complications in the operative treatment of patella fractures. J Orthop Trauma. 1997;11:183–187. doi: 10.1097/00005131-199704000-00008. [DOI] [PubMed] [Google Scholar]
- 5.Hughes S.C., Stott P.M., Hearnden A.J., Ripley L.G. A new and effective tension-band braided polyester suture technique for transverse patellar fracture fixation. Injury. 2006;38:212–222. doi: 10.1016/j.injury.2006.07.013. [DOI] [PubMed] [Google Scholar]
- 6.Patel V.R., Parks B.G., Wang Y., Ebert F.R., Jinnah R.H. Fixation of patella fractures with braided polyester suture: a biomechanical study. Injury. 2000;31:1–6. doi: 10.1016/s0020-1383(99)00190-4. [DOI] [PubMed] [Google Scholar]
- 7.Wright P.B., Kosmopoulos V., Coté R.E., Tayag T.J., Nana A.D. FiberWire is superior in strength to stainless steel wire for tension band fixation of transverse patellar fractures. Injury. 2009;40:1200–1203. doi: 10.1016/j.injury.2009.04.011. [DOI] [PubMed] [Google Scholar]
- 8.Schneider C.A., Rasband W.S., Eliceiri K.W. NIH Image to Image J: 25 years of image analysis. Nat Methods. 2012;9:671–675. doi: 10.1038/nmeth.2089. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Hungerford D.S., M. B Biomechanics of the patellofemoral joint. Clin Orthop. 1979;144:9–15. [PubMed] [Google Scholar]
- 10.Berg E.E. Open reduction internal fixation of displaced transverse patella fractures with figure-eight wiring through parallel cannulated compression screws. J Orthop Trauma. 1997;11:573–576. doi: 10.1097/00005131-199711000-00005. [DOI] [PubMed] [Google Scholar]
- 11.Weber M.J., Janecki C.J., McLeod P., Nelson C.L., Thompson J.A. Efficacy of various forms of fixation of transverse fractures of the patella. J Bone Jt Surg Am. 1980;62:215–220. [PubMed] [Google Scholar]
- 12.Hoshino C.M., Tran W., Tiberi J.V. Complications following tension-band fixation of patellar fractures with cannulated screws compared with Kirschner wires. J Bone Jt Surg Am. 2013;95:653–659. doi: 10.2106/JBJS.K.01549. [DOI] [PubMed] [Google Scholar]
- 13.Gosal H.S., Singh P., Field R.E. Clinical experience of patellar fracture fixation using metal wire or non-absorbable polyester–a study of 37 cases. Injury. 2001;32:129–135. doi: 10.1016/s0020-1383(00)00170-4. [DOI] [PubMed] [Google Scholar]
- 14.Grood E.S., Suntay W.J., Noyes F.R., Butler D.L. Biomechanics of the knee-extension exercise. Effect of cutting the anterior cruciate ligament. J Bone Jt Surg Am. 1984;66:725–734. [PubMed] [Google Scholar]
- 15.Halvorson T.L., Kelley L.A., Thomas K.A., Whitecloud TSr, Cook S.D. Effects of bone mineral density on pedicle screw fixation. Spine (Phila Pa 1976) 1994;19:2415–2420. doi: 10.1097/00007632-199411000-00008. [DOI] [PubMed] [Google Scholar]