

Abstract
Patients with long dialysis vintage have low cardiac output for various reasons. Although kidney transplantation is known to improve cardiac mortality, patients are sometimes evaluated as contraindicated for transplantation because of cardiac risk. We successfully performed kidney transplantation for a patient with a long dialysis vintage and dilated cardiomyopathy. Sequential 123I-metaiodobenzylguanidine (123I-MIBG) scintigraphy suggested that amelioration of uraemia improved cardiac function. Kidney transplantation for patients with severely impaired cardiac function is safe and effective under careful perioperative monitoring irrespective of dialysis vintage. Sequential 123I-MIBG scintigraphy can be used as an evaluation tool for the improvement in cardiac function.
Keywords: dilated cardiomyopathy, 123I-MIBG scintigraphy, kidney transplantation
Introduction
It is well known that patients with long dialysis vintage have low cardiac output for various reasons including dilated cardiomyopathy, which is otherwise known as ‘uraemic cardiomyopathy’. Although the aetiology has still not been clearly defined, uraemic states have been associated with sympathetic overactivity [1] and autonomic neuropathy [2]. Kurata et al. have shown that end-stage renal disease (ESRD) [3] patients manifest abnormal myocardial 123I-metaiodobenzylguanidine (123I-MIBG) uptake that has been used to evaluate cardiac sympathetic innervations. MIBG provides a means to evaluate the cardiac adrenergic nerve activity, because MIBG is subject to the same uptake and storage mechanisms as norepinephrine. ESRD patients with decreased left ventricular ejection fraction (LVEF) have not usually been referred for transplantation, because they are considered at increased risk of perioperative morbidity and mortality, although kidney transplantation significantly decreases those risks. Indeed, it has been reported that expectations are low for patients with longer dialysis vintage to improve their cardiac function after kidney transplantation [4]. We successfully performed living kidney transplantation for a patient with a long dialysis vintage of 17 years and dilated cardiomyopathy.
Case report
A 32-year-old male with ESRD was referred for living donor kidney transplantation. He started haemodialysis 17 years ago. He had repeated episodes of congestive heart failure. His cardiothoracic ratio (CTR; the ratio of the transverse diameter of the heart to the internal diameter of the chest at its widest point) had increased and the symptoms of heart failure gradually exacerbated (NYHA class III). He underwent coronary angiography (CAG) and haemodynamic monitoring. CAG showed no coronary artery disease but diffusely hypokinetic left ventricular wall motion without hypertrophy. Haemodynamic data showed maintained cardiac index and relevant pulmonary capillary wedge pressure (PCWP) but extremely low systolic function (cardiac index 2.81, PCWP 12 mmHg, LVEF 18%) leading to the diagnosis of dilated cardiomyopathy. The laboratory results before the transplantation were as follows: haemoglobin 11.1 g/dl; brain natriuretic peptide (BNP) 1046 pg/ml and CTR 61.4%. Echocardiography showed the left ventricular diastolic diameter (LVDd) of 84 mm, left ventricular systolic diameter (LVDs) of 71 mm and ejection fraction (EF) of 28%. After obtaining informed consent and clearance from cardiology consult, we performed living kidney transplantation. We monitored cardiac function perioperatively. His serum creatinine level decreased to 1.10 mg/dl by the 10th postoperative day. Although his blood pressure (BP) was very low without antihypertensives, it rose postoperatively and renin–angiotensin system inhibitors could be started. One year after the operation, CTR and BNP had decreased from 61% to 54% and 1047 pg/ml to 75 pg/ml, respectively, and the NYHA functional class improved to I–II. His body weight never decreased post-transplant, rather it increased, which suggests that volume overload was not present before transplantation. Despite this clinical improvement (shown in Figure 1), his LVEF improved only modestly from 28% to 31%. To evaluate his cardiac function in more detail, we performed 123I-MIBG scintigraphy. The area showing the 123I-MIBG uptake reduction or absence markedly decreased over time. The late heart-to-mediastinum (H/M) ratio in 123I-MIBG scintigram, indicating the normal myocardial uptake of MIBG, rose to be within the normal range (2.35) compared to before transplantation (1.3), which provides evidence for significant improvement of his cardiac autonomic nerve function. In addition, he underwent thallium (Tl) scintigraphy to evaluate myocardial viability. The post-inferior wall showed moderate radioisotope uptake reduction, indicating the presence of viable myocardium except in this region. 123I-MIBG uptake improved over time (Figure 2).
Fig. 1.

Clinical course of BNP, body weight and cardiothoracic index (CTR). Although after the operation body weight increased, BNP and CTR decreased, indicating that the circulating volume has decreased.
Fig. 2.
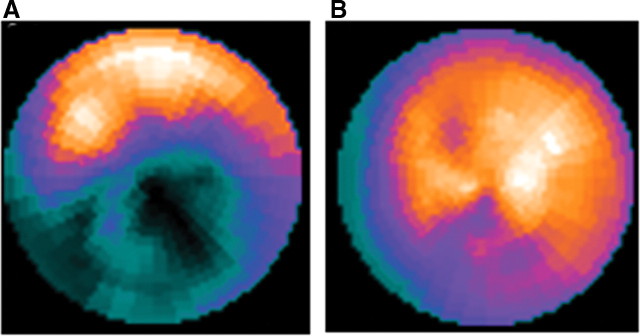
(A) Cardiac 123I-MIBG uptake and (B) 201Tl uptake 1 year after transplantation. The coloured areas indicate isotope uptake and black areas show the absence of isotope uptake. The blue areas indicate a reduction of isotope uptake.
Discussion
There are arguments for and against kidney transplantation in ESRD patients with significantly decreased systolic function, although transplantation generally decreases cardiac mortality. In particular, long dialysis vintage is regarded to be associated with irreversible cardiac damage.
In this report, we wish to emphasize two clinical points. First, sequential 123I-MIBG scintigraphy can be used as an evaluation tool for the improvement of cardiac sympathetic function. Secondly, even in ESRD patients with a long dialysis history, severely impaired systolic function may be at least partially reversible.
123I-MIBG imaging provides a means to evaluate the cardiac adrenergic nerve activity. Uptake reduction in the 123I-MIBG scintigram suggests structural and functional cardiac, microvascular, and neurological anomalies and interstitial fibrosis [5] that is documented in patients with ESRD.
Wali et al. have shown that patients with a long history of dialysis (45.1 ± 19.9 months) were prone to have little or no improvement in LVEF assessed by echocardiography [4]. Although LVEF in this patient has not shown marked improvement during the first year after transplantation, parameters such as CTR and serum BNP levels, together with MIBG parameters, have improved.
In addition, Agarwal et al. demonstrated that significant autonomic nerve dysfunction in patients who developed hypotension during haemodialysis and marked reversal of autonomic dysfunction was observed following kidney transplantation [2]. Kurata et al. reported that kidney transplantation provided the improvement of uraemic cardiac sympathetic neuropathy assessed by 123I-MIBG scintigraphy imaging [6].
In this patient, history of frequent heart failure due to interdialytic weight gain when LVEF was still normal is indicative of volume overload. However, he was not volume overloaded, as a result of intensive dry weight and blood pressure control, after LVEF deteriorated. Furthermore, his body weight increased after the transplantation. This implies that amelioration of uraemia itself, not amelioration of chronic volume overload, improved cardiac function in this patient, which in turn indicates that it was the uraemic condition that caused myocardial depression. Thus, it is considered that the patient had uraemic cardiomyopathy. We additionally examined thallium scintigraphy. The uptake of thallium scintigram means that the cardiac muscle still has a capacity for recovery. Findings from the cardiac scintigram in this patient (i.e. the discrepancy between the patterns of 201Tl and 123I-MIBG distribution) suggest still denervated, but, nonetheless, viable myocardium, supporting the idea that even with long dialysis vintage, cardiac function can improve after removal of uraemia.
Conclusion
Kidney transplantation for ESRD patients with severely impaired cardiac function due to dilated cardiomyopathy or uraemic cardiomyopathy is safe and effective under careful monitoring during and after transplantation, irrespective of dialysis vintage. Sequential 123I-MIBG scintigraphy can be used as an evaluation tool for the improvement of cardiac sympathetic function.
Conflict of interest statement. None declared.
References
- 1.Converse RL, Jr, Jacobsen TN, Toto RD, et al. Sympathetic overactivity in patients with chronic renal failure. N Eng J Med. 1992;327:1912–1918. doi: 10.1056/NEJM199212313272704. [DOI] [PubMed] [Google Scholar]
- 2.Agarwal A, Anand IS, Sakhuja V, et al. Effect of dialysis and renal transplantation on autonomic dysfunction in chronic renal failure. Kidney Int. 1991;40:489–495. doi: 10.1038/ki.1991.236. [DOI] [PubMed] [Google Scholar]
- 3.Kurata C, Uehara A, Ishikawa A. Improvement of cardiac sympathetic innervation by renal transplantation. J Nucl Med. 2004;45:1114–1120. [PubMed] [Google Scholar]
- 4.Wali RK, Wang GS, Gottlieb SS, et al. Effect of kidney transplantation on left ventricular systolic dysfunction and congestive heart failure in patients with end-stage renal disease. J Am Coll Cardiol. 2005;45:1051–1060. doi: 10.1016/j.jacc.2004.11.061. [DOI] [PubMed] [Google Scholar]
- 5.Bialostozky D, Leyva M, Villarreal T, et al. Myocardial perfusion and ventricular function assessed by SPECT and gated-SPECT in end-stage renal disease patients before and after renal transplant. Arch Med Res. 2007;38:227–233. doi: 10.1016/j.arcmed.2006.09.017. [DOI] [PubMed] [Google Scholar]
- 6.Patel RK, Mark PB, Johnston N, et al. Renal transplantation is not associated with regression of left ventricular hypertrophy: a magnetic resonance study. Clin J Am Soc Nephrol. 2008;3:1807–1811. doi: 10.2215/CJN.01400308. [DOI] [PMC free article] [PubMed] [Google Scholar]