

After spontaneous vaginal delivery, a 32-week-gestation female baby presented immediately with respiratory distress, APGAR scores 0 (1 min) and 2 (5 min), generalized skin oedema and bilateral pleural effusion. The prenatal history was unremarkable. The clinical diagnosis was nonimmune hydrops fetalis, and treatment with mechanical ventilation, surfactant, prostaglandin and supportive measures was initiated. Complications included Escherichia coli sepsis and severe liver dysfunction during the fourth week of life with jaundice (total bilirubin 34.2 mg/dL (0.1–1.0), conjugated bilirubin 24.1 mg/dL (0–0.3), SGOT 231 U/L (8–37), SGPT 86 U/L (8–35), serum albumin 2.9 g/dL (3.5–5.0)). Subsequent acute kidney injury (blood urea nitrogen 184 mg/dL and serum creatinine 1.3 mg/dL) and multiple anuric episodes ensued. The baby died 2 weeks later. At autopsy, the finding of primary pulmonary lymphangiectasia was thought to be the cause of hydrops fetalis. The kidneys were green after formalin fixation (Figure 1). Numerous pigmented casts were exclusively present within distal tubules or collecting ducts (Figure 2) and not within proximal tubules. Most casts were brown red and many had additional greenish-yellow discoloration. A Hall's stain highlights bile pigment in green by converting bilirubin to biliverdin, which confirmed the presence of bile in all casts (Figure 2 inset), and supports the diagnosis of jaundice-associated acute kidney injury. Occasional calcium oxalate crystals were also noted within distal nephron segments (not shown) of which some were green tinged.
Fig. 1.

Conversion of bilirubin to biliverdin after formalin fixation accentuates the green discolouration of the kidney.
Fig. 2.
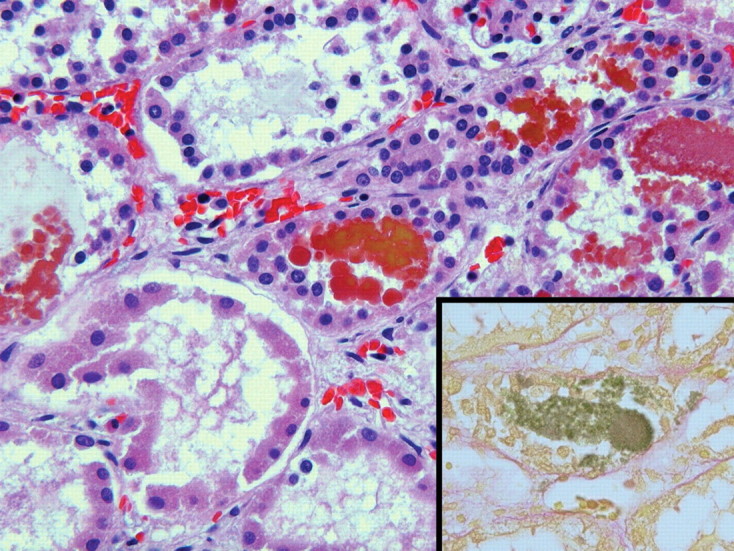
Dark red and yellowish-green intratubular casts in the distal nephron segments consist of bile, as confirmed by the Hall's stain (inset, 400×) (H&E, 400×).
Acute kidney injury associated with liver dysfunction in jaundiced patients (historically termed cholemic nephrosis) is not fully understood, but tubular injury by direct toxicity of bile salts and bilirubin has been proposed [1–3]. The renal function can recover if the jaundice is managed. The extensive intratubular bile casts observed in our case provide evidence that severe jaundice can lead to intratubular accumulation of bilirubin and bile salts, which may impair renal function either by direct tubular toxicity, nephron obstruction, or both.
Conflict of interest statement. None declared.
References
- 1.Betjes MG, Bajema I. The pathology of jaundice-related renal insufficiency: cholemic nephrosis revisited. J Nephrol. 2006;19:229–233. [PubMed] [Google Scholar]
- 2.Sant SM, Purandare NM. Cholemic nephrosis—an autopsy and experimental study. J Postgrad Med. 1965;11:79–89. [PubMed] [Google Scholar]
- 3.Thompson LL, Franzier WD, Ravdin LS. The renal lesion in obstructive jaundice. Am J Med Science. 1940;199:305–312. [Google Scholar]