

Abstract
Sodium or calcium polystyrene sulfonate (Kayexalate or analog) is an ion-exchange resin commonly used to treat hyperkalaemia in patients with chronic kidney disease. It is known to cause digestive complications, such as nausea, vomiting and constipation. Although rare, colonic necrosis and perforation are very severe complications associated with the medication. In this case report, we present a case of calcium polystyrene sulfonate-induced colonic necrosis and perforation to remind clinicians of this rare, but dangerous, toxicity associated with this commonly used medication.
Keywords: calcium polystyrene sulfonate, chronic kidney disease, colon perforation, hyperkalaemia
Background
Colonic necrosis has been described as a rare complication after the administration of Kayexalate [1, 2]. In this case study, we present a case of calcium polystyrene sulfonate-induced colonic necrosis and perforation to remind clinicians of this rare, but dangerous, toxicity associated with this commonly used medication.
Case report
A 78-year-old woman with Stage 4 chronic kidney disease (CKD) due to chronic pyelonephritis, and a right hypoplastic kidney was presented to our emergency department with a 2-day history of abdominal pain. Her medical history included epilepsy that was treated with carbamazepine, hypertension and hyperlipidaemia, for which she received carvedilol and atorvastatin. Because of the persistent hyperkalaemia, she was treated with calcium polystyrene sulfonate at 30 g/day (anti-potassium granule; Assos Drug, Istanbul, Turkey). As a result of the CKD, she was prescribed calcitriol for a mineral and bone disorder, darbepoetin alpha for anaemia and sodium hydrogen carbonate for acidosis. Upon initial physical examination, her abdomen was non-distended with normoactive bowel sounds, but there was diffuse tenderness in her abdomen. Significant laboratory values at the time of admission included sodium 138 mEq/L, potassium 4.6 mEq/L, pH 7.20, bicarbonate 13 mEq/L, Blood Urea Nitrogen 71 mg/dL, creatinine 2.6 mg/dL, leukocytes 15 500/mm3, eosinophils 110/mm3, haematocrit 32.7%, platelets 221 000/mm3 and C-reactive protein 10.9 mg/dL. On the second day of hospitalization, the abdominal pain worsened and free air under the diaphragm was found on abdominal radiography. She was taken immediately to the operating room for a laparotomy. Her sigmoid colon was found to be necrotic and perforated. A biopsy was performed and the perforated segment was repaired by primary closure. The full-cut biopsy contained the perforated area and layers of colonic wall. The surface of the deep ulcer contained necroinflammatory debris and various sized fragments of basophilic crystalloid material with angulated margins on microscopic examination (Figure 1a and b). Also, there were no features of chronic colitis, including inflammatory bowel disease or chronic ischaemic colitis. This characteristic finding is consistent with Kayexalate crystals.
Fig. 1.
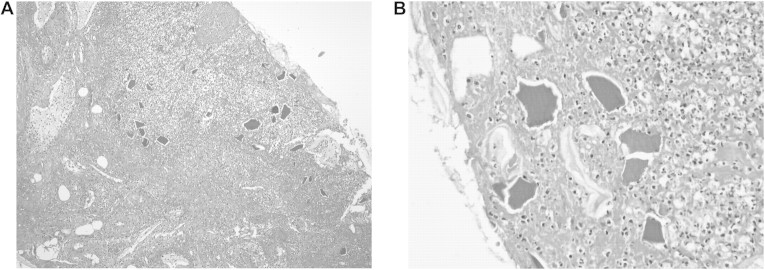
(A) The basophilic crystalloid material in the necroinflammatory background of the ulcer surface (haematoxylin and eosin, original magnification, ×100). (B) The basophilic crystalloid material in the necroinflammatory background of the ulcer surface (haematoxylin and eosin, original magnification, ×400).
Discussion
Sodium polystyrene sulfonate can also bind intraluminal calcium, leading to constipation, fecal impaction and subsequent bowel obstruction or perforation [1]. The real incidence of colonic necrosis after Kayexalate remains unknown. Gerstman et al. [2] reported a 0.27% overall incidence, with a higher incidence (1.8%) during the postoperative period. Lillemoe et al. originally reported colonic necrosis due to Kayexalate–sorbitol enemas, along with experimental evidence suggesting that the necrosis was due to sorbitol rather than the Kayexalate in presence of uraemia. Extensive transmural necrosis was noted in rats receiving enemas of sorbitol or Kayexalate in sorbitol in both the uraemic and non-uraemic groups [3]. As in this case report, renal failure may be an important facilitating factor in the pathogenesis of the necrosis. In contrast to the experimental data, our case was treated with calcium polystyrene sulfonate orally, not rectally. This case report shows that colonic necrosis is caused not only by Kayexalate–sorbitol, but also by a calcium analog. Rashid et al. noted that Kayexalate in sorbitol given as an enema or orally to treat hyperkalaemia has been reported to induce intestinal necrosis in uraemic patients. They studied clinical and pathologic features of 15 patients and observed Kayexalate crystals in tissue specimens from surgical resections and endoscopic biopsies [4]. The mechanism of the necrosis and perforation is unknown. One possibility is elevated renin levels, commonly seen in renal insufficiency, that predispose the patient to non-occlusive mesenteric ischaemia via angiotensin-mediated vasoconstriction [5]. One gram of Kayexalate possesses a theoretical in vitro exchange capacity of 2–3.1 mEq of potassium and in vivo capacity of ∼1 mEq [6]. Emmett et al. [7] reported that in vivo potassium-binding capacity may be lower than previously estimated, more on the order of 0.4–0.8 mEq/g of Kayexalate resin. In contrast to other minor digestive complications associated with Kayexalate treatment, colonic perforation results in significant morbidity and mortality.
As a result, potassium exchange resins may, although rarely, induce a colonic perforation, and this diagnosis should be considered in a patient treated as such in case of acute abdomen. The clinicians must be aware of the possible rare and serious complications of potassium exchange resins.
Acknowledgments
Conflict of interest statement. None declared.
References
- 1.Dardik A, Moesinger RC, Efron G, et al. Acute abdomen with colonic necrosis induced by Kayexalate-sorbitol. South Med J. 2000;93:511–513. [PubMed] [Google Scholar]
- 2.Gerstman BB, Kirkman R, Platt R. Intestinal necrosis associated with postoperative orally administered sodium polystyrene sulfonate in sorbitol. Am J Kidney Dis. 1992;20:159–161. doi: 10.1016/s0272-6386(12)80544-0. [DOI] [PubMed] [Google Scholar]
- 3.Lillemoe KD, Romolo JL, Hamilton SR, et al. Intestinal necrosis due to sodium polystyrene (Kayexalate) in sorbitol enemas: clinical and experimental support fort he hypothesis. Surgery. 1987;101:267–272. [PubMed] [Google Scholar]
- 4.Rashid A, Hamilton SR. Necrosis of the gastrointestinal tract in uremic patients as a result of sodium polystyrene sulfonate (Kayexalate) in sorbitol: an underrecognized condition. Am J Surg Pathol. 1997;21:60–69. doi: 10.1097/00000478-199701000-00007. [DOI] [PubMed] [Google Scholar]
- 5.Rogers FB, Li SC. Acute colonic necrosis associated with sodium polystyrene sulfonate (Kayexalate) enemas in critically ill patient: case report and review of the literature. J Trauma. 2001;51:395–397. doi: 10.1097/00005373-200108000-00031. [DOI] [PubMed] [Google Scholar]
- 6.McGowan CE, Saha S, Chu G, et al. Intestinal necrosis due to sodium polystyrene sulfonate (Kayexalate) in sorbitol. South Med J. 2009;102:493–497. doi: 10.1097/SMJ.0b013e31819e8978. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Emmett M, Hootkins RE, Fine KD, et al. Effect of three laxatives and a cation exchange resin on fecal sodium and potassium excretion. Gastroenterology. 1995;108:752–760. doi: 10.1016/0016-5085(95)90448-4. [DOI] [PubMed] [Google Scholar]