

Abstract
Foot drop is defined as the weakness of the foot and ankle dorsiflexion. Acute unilateral foot drop is a well-documented entity, whereas bilateral foot drop is rarely documented. Slowly progressing bilateral foot drop may occur with various metabolic causes, parasagittal intracranial pathologies, and cauda equina syndrome. Acute onset of bilateral foot drop due to disc herniation is extremely rare. Here we present two cases of acute bilateral foot drop due to disc herniation. The first patient was a 45-year-old man presented with acute bilateral foot drop, without any sign of the cauda equina syndrome. Lumbar magnetic resonance imaging of the patient revealed L4-5 disc herniation. To our knowledge, this is the first presented case of acute bilateral foot drop without any signs of cauda equina syndrome caused by L4-5 disc herniation. The second patient was a 50-year-old man who was also presented with acute bilateral foot drop, and had T12-L1 disc herniation with intradural extension. Also this is the first presented case of T12-L1 disc herniation with intradural extension causing acute bilateral foot drop. We performed emergent decompressive laminectomy to both of the patients and extrude disc materials were excised. Both of the patients were recovered with favorable outcome.
Keywords: Bilateral foot drop, lumbar disc herniation, surgery
Introduction
Foot drop is defined as a weak anterior tibialis, extensor hallucis longus and extensor digitorum longus muscles which manifests as significant weakness of the foot and ankle dorsiflexion.[1]
Acute unilateral foot drop is a well-known entity.[2,3] On the other hand, bilateral foot drop in progressive fashion is also known, but rare. In particular, slow progressing bilateral foot drop occurs with various metabolic causes as in anorexia nervosa,[4] hypothyroid myopathy,[5] Chron's disease,[6] and post electroconvulsive therapy.[7] Parasagittal intracranial pathologies[8] and cauda equine[3] may also cause progressive bilateral foot drop.
Acute onset of bilateral foot drop due to disc herniation is extremely rare. Here we present two cases of acute bilateral foot drop caused by L4-5 and T12-L1 disc herniation, without in association with any other condition.
Case Reports
Patient 1
A 45-year-old man presented with sudden onset of severe backache and bilateral foot drop developed while he was lifting a heavy weight. He presented to emergency room 2 h after the onset of symptoms. He had mild, non-specific back pain for 3 years previously.
Clinical examination revealed bilateral positive leg raising test at 30° and bilateral foot drop was documented (muscle strength was 1/5 in both foot dorsiflexion and big toe extension bilaterally). Mild hypoesthesia of both L5 dermatomes was also documented. Perianal sensation was intact with normal bladder function. All deep tendon reflexes were normal and no upper motor neuron signs were documented. All other muscle strengths and neurological tests were normal.
Apart from essential hypertension, his past medical history was otherwise unremarkable. Blood counts, general biochemistry, protein, tumor markers, and level of vitamin B12, and folic acid measured a month ago were either normal or negative. He had neither a history of recent surgery nor exposure to toxins or heavy metals.
Emergent lumbar spinal magnetic resonance imaging (MRI) was obtained and revealed large extrude disc fragment at L4-5 level with evidence of bilateral compression of L5 foramina [Figure 1].
Figure 1.
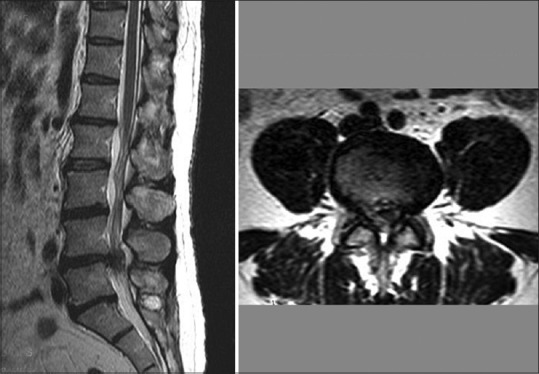
Lumbar spinal MRI shows the L4-5 disc herniation causing bilateral foraminal stenosis
The patient underwent emergent surgery 4 h after the initiation of the foot drop. Bilateral L4 decompressive laminectomy was performed and a large extruded central disc fragment causing bilateral neural foraminal obliteration was excised microsurgically. Postoperatively his bilateral foot drop improved progressively. At the time of discharge (postoperative second day), ankle dorsiflexion and big toe extension both improved to 4/5 bilaterally. His neurological examination at the first postoperative month was completely normal.
Patient 2
A 50-year-old man presented with sudden onset of bilateral foot drop developed while he was playing basketball. He denied any trauma. He had mild, non-specific back pain for a long time. On neurological examination bilateral weakness in foot dorsiflexion (1/5) and big toe extension (1/5) were documented. All other motor functions and muscle tones were normal in both limbs. No sensory deficit was documented and all the deep tendon reflexes were normal. Anal tonus and reflexes were present and no erectile, bladder or bowel dysfunction was reported.
His past medical history was unremarkable and he denied any exposure to toxins or heavy metals. Emergent lumbar spinal MRI revealed a T12-L1 disc herniation and subsequent cord compression [Figure 2]. Therefore, the patient underwent emergent posterior T12-L1 laminectomy 6 h after the beginning of the foot drop. Using operating microscope, a large extrude disc with intradural extension was totally removed with opening of the dura. The dura mater was sealed with a fat graft and fibrin glue.
Figure 2.

Spinal MRI reveals T12-L1 disc herniation and subsequent cord compression
The postoperative period was uneventful and the patient was discharged in the second postoperative day with moderate paresis of ankle dorsiflexion (3/5). The patient was taken to the rehabilitation program. After a month, his muscle strength of ankle dorsiflexion improved to +4/5 bilaterally.
Discussion
Foot drop is defined as the weakness of the anterior tibialis muscle and is frequently accompanied by weakness of the extensor hallucis longus and extensor digitorum longus. Foot drop results from a disruption in the neural pathway starting from parasagittal cortical motor neurons to the spinal cord upper motor neurons and the peripheral spinal cord roots and ending with the peroneal nerve. It is usually caused by lower motor neuron pathologies, commonly disruption of the conduction from deep peroneal nerve (L4-5). L4-5 radiculopathy is the most common cause of foot drop, usually caused by disc herniation of foraminal stenosis.[1] Furthermore, lumbar disc herniation may cause cauda equina syndrome which leads to foot drop. But in this condition, foot drop is mostly unilateral, almost always progressive and associated with loss of function of the bowel, bladder, and sexual functions.[2,3] Other common etiologies include local peroneal nerve damage due to trauma, entrapment, compartment syndrome, and tumor.[9,10,11] Systemic diseases such as diabetes, vasculitis, connective tissue, and autoimmune disease may also be the etiological cause.[12,13,14] In these circumstances, foot drop is almost always unilateral.
An isolated bilateral foot drop is a very rare condition and occurs with various metabolic conditions such as anorexia nervosa,[4] hypothyroid myopathy,[5] Chron's disease,[6] and post electroconvulsive therapy.[7] Also, intracranial pathologies such as parasagittal tumors may also cause bilateral foot drop.[8] However, in these conditions, foot drop is in progressive nature. A sudden onset of bilateral foot drop is an extremely rare condition.[7]
Mahapatra et al.[7] presented the first case with acute bilateral foot drop due to a prolapsed intervertebral disc at L3-4 level. This patient also had other features of cauda equina syndrome such as urinary involvement. This patient underwent emergent L3-4 laminectomy and a large extruded disc material was removed. The patient recovered well in the postoperative period.
Recently, Oluigbo et al.[15] reported a case of acute bilateral foot drop related to lumbar canal stenosis. In this case, there was no evidence of disc herniation either on MRI or at surgery.
The first patient presented in our report had an acute L4-5 disc herniation which was the cause of acute bilateral foot drop. This patient had no signs and the symptoms of the cauda equina syndrome. As to our knowledge, this is the first case of L4-5 disc herniation causing acute bilateral foot drop without in association with cauda equina syndrome. In this condition, acute radiculopathy associated with bilateral L5 root may occur as a result of L4-5 disc herniation causing bilateral foot drop.
In our second presented patient, acute onset of bilateral foot drop was caused by a herniated disk at T12-L1 level. Previous reports showed that thoracic disc herniation may cause progressive bilateral foot drop.[16] Intradural nature and acute onset of the bilateral foot drop makes our case unique. Wall et al.[17] showed that at T12-L1 intervertebral level, the spinal cord begins to taper and is surrounded by L1 to L5 nerve roots. Although the L1 nerve root situated laterally to the cord and the remaining nerve roots are arranged in an appropriate order, respectively, where L5 nerve root is situated at the most medial side around the cord. We can explain with anatomical localization that T12-L1 disc herniation compressed both L5 nerve roots and leaded to bilateral acute foot drop.
A rapid onset of spinal nerve root compression may cause more serious effect on the function than a progressive compression. However, the recovery is also more rapid after early decompression of the acute compression.[17] Both our two patients were recovered well after early decompressive surgery.
In conclusion, acute bilateral foot drop is an extremely rare entity. Both L4-5 and T12-L1 disc herniations may be the cause. In this situation, emergent lumbar spinal MRI with extension to lower thoracic vertebrae is recommended. Early surgery may prevent catastrophic neurological sequels and have favorable outcome.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Iizuka Y, Iizuka H, Tsutsumi S, Nakagawa Y, Nakajima T, Sorimachi Y, et al. Foot drop due to lumbar degenerative conditions: Mechanism and prognostic factors in herniated nucleus pulposus andlumbar spinal stenosis. J Neurosurg Spine. 2009;10:260–4. doi: 10.3171/2008.12.SPINE08500. [DOI] [PubMed] [Google Scholar]
- 2.Bartels RH, de Vries J. Hemi-cauda equina syndrome from herniated lumbar disc: A neurosurgical emergency? Can J Neurol Sci. 1996;23:296–9. doi: 10.1017/s0317167100038257. [DOI] [PubMed] [Google Scholar]
- 3.Chang HS, Nakagawa H, Mizuno J. Lumbar herniated disc presenting with cauda equina syndrome. Long term follow up of four cases. Surg Neurol. 2000;53:100–5. doi: 10.1016/s0090-3019(99)00180-9. [DOI] [PubMed] [Google Scholar]
- 4.Kershenbaum A, Jaffa T, Zeman A, Boniface S. Bilateral foot drop in-patient with anorexia nervosa. Int J Eat Disord. 1997;22:335–7. doi: 10.1002/(sici)1098-108x(199711)22:3<335::aid-eat14>3.0.co;2-x. [DOI] [PubMed] [Google Scholar]
- 5.Bhansali A, Chandran V, Ramesh J, Kashyap A, Dash RJ. Acute myxoedema: An unusual presenting manifestation of hypothyroid myopathy. Postgrad Med J. 2000;76:99–100. doi: 10.1136/pmj.76.892.99. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Gariballa SE, Gunashekhar NP. Bilateral foot drop, weight loss and rectal bleeding as an acute presentation of Crohn's disease. Postgrad Med J. 1994;70:762–3. doi: 10.1136/pgmj.70.828.762. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Mahapatra AK, Gupta PK, Pawar SJ, Sharma RR. Sudden bilateral foot drop: An unusual presentation of lumbar disc prolapse. Neurol India. 2003;51:71–2. [PubMed] [Google Scholar]
- 8.Eskandary H, Hamzei A, Yasamy MT. Foot drop following brain lesion. Surg Neurol. 1995;43:89–90. doi: 10.1016/0090-3019(95)80048-l. [DOI] [PubMed] [Google Scholar]
- 9.Baker JF, Lui DF, Kiely PD, Synnott KA. Foot drop—an unusual presentation of exertional compartment syndrome. Clin J Sport Med. 2009;19:236–7. doi: 10.1097/JSM.0b013e3181a39b04. [DOI] [PubMed] [Google Scholar]
- 10.Kehdi EE, Huynh W, Cordato DJ, Bonura A, Hanna IY. Spontaneous peroneal compartment syndrome causing acute foot drop. Intern Med J. 2008;38:926–30. doi: 10.1111/j.1445-5994.2008.01812.x. [DOI] [PubMed] [Google Scholar]
- 11.Symons JA, Palmer GM. Neuropathic pain and foot drop related to nerve injury after short duration surgery and caudal analgesia. Clin J Pain. 2008;24:647–9. doi: 10.1097/AJP.0b013e3181706ca2. [DOI] [PubMed] [Google Scholar]
- 12.Amini M, Najafi I, Ganji MR, Hakemi MS, Nouri M. Foot-drop: An unusual complaint in Henoch-Schonlein purpura. Pediatr Nephrol. 2009;24:219–20. doi: 10.1007/s00467-008-0952-5. [DOI] [PubMed] [Google Scholar]
- 13.Katirji B. Peroneal neuropathy. Neurol Clin. 1999;17:567–91. doi: 10.1016/s0733-8619(05)70153-5. [DOI] [PubMed] [Google Scholar]
- 14.Stewart JD. Foot drop: Where, why and what to do? Pract Neurol. 2008;8:158–69. doi: 10.1136/jnnp.2008.149393. [DOI] [PubMed] [Google Scholar]
- 15.Oluigbo CO, Qadri SR, Dardis R, Choksey MS. Lumbar canal stenosis presenting with acute bilateral foot drop. Br J Neurosurg. 2006;20:87–9. doi: 10.1080/02688690600682358. [DOI] [PubMed] [Google Scholar]
- 16.Papapostolou A, Tsivgoulis G, Papadopoulou M, Karandreas N, Zambelis T, Spengos K. Bilateral drop foot due to thoracic disc herniation. Eur J Neurol. 2007;14:e5. doi: 10.1111/j.1468-1331.2007.01539.x. [DOI] [PubMed] [Google Scholar]
- 17.Olmarker K. Spinal nerve root compression. Nutrition and function of the porcine cauda equine compressed in vivo. Acta Orthop Scand Suppl. 1991;242:1–27. [PubMed] [Google Scholar]