

Abstract
Background:
Brain tumors, traumatic head injury, and other intracranial processes including infections, can cause increased intracranial pressure and lead to overstimulation of the vagus nerve. As a result, increased secretion of gastric acid may occur which leads to gastro-duodenal ulcer formation known as Cushing's ulcer.
Methods:
A review of original records of Dr. Harvey Cushing's patients suffering from gastro-duodenal ulcers was performed followed by a discussion of the available literature. We also reviewed the clinical records of the patients never reported by Cushing to gain his perspective in describing this phenomenon. Dr. Cushing was intrigued to investigate gastro-duodenal ulcers as he lost patients to acute gastrointestinal perforations following successful brain tumor operations. It is indeed ironic that Harvey Cushing developed a gastro-duodenal ulcer in his later years with failing health.
Results:
Clinically shown by Cushing's Yale Registry, a tumor or lesion can disrupt this circuitry, leading to gastroduodenal ulceration. Cushing said that it was “reasonable to believe that the perforations following posterior fossa cerebellar operations were produced in like fashion by an irritative disturbance either of fiber tracts or vagal centers in the brain stem.”
Conclusion:
Harvey Cushing's pioneering work depicted in his Yale registry serves as a milestone for continuing research that can further discern this pathway.
Keywords: Brain neoplasms, duodenal ulcer, gastric ulcer, intracranial pressure
Introduction
Cushing's ulcer is a gastro-duodenal ulcer produced by elevated intracranial pressure caused by an intracranial tumor, head injury or other space-occupying lesion. The ulcer, usually single and deep, may involve the esophagus, stomach, and duodenum.[1] Increased intracranial pressure may affect different areas of the hypothalamic nuclei or brainstem leading to overstimulation of the vagus nerve or paralysis of the sympathetic system. Both of these circumstances increase secretion of gastric acid and the likelihood of ulceration of gastro-duodenal mucosa.[2] In his later years, Cushing suffered from a gastric ulcer, one that he attributed to his stressful efforts to explain this phenomenon.[3]
Dr. Cushing reported some of his patients suffering from this ulcer. Our review of his original patient records at the Yale Brain Tumor Registry revealed additional previously unreported cases. Therefore, a review of the original records of Cushing's patients suffering from this form of gastro-duodenal ulcer was performed with a discussion of the available literature to potentially elucidate a different perspective on events leading to the introduction of this disorder.
Case Reports
Cushing's original case reports provide accounts of patients presenting with epigastric pain and vomiting coupled with an intracranial brain tumor [Table 1].
Table 1.
Description of Dr. Cushing's gastro-duodenal ulcer patients
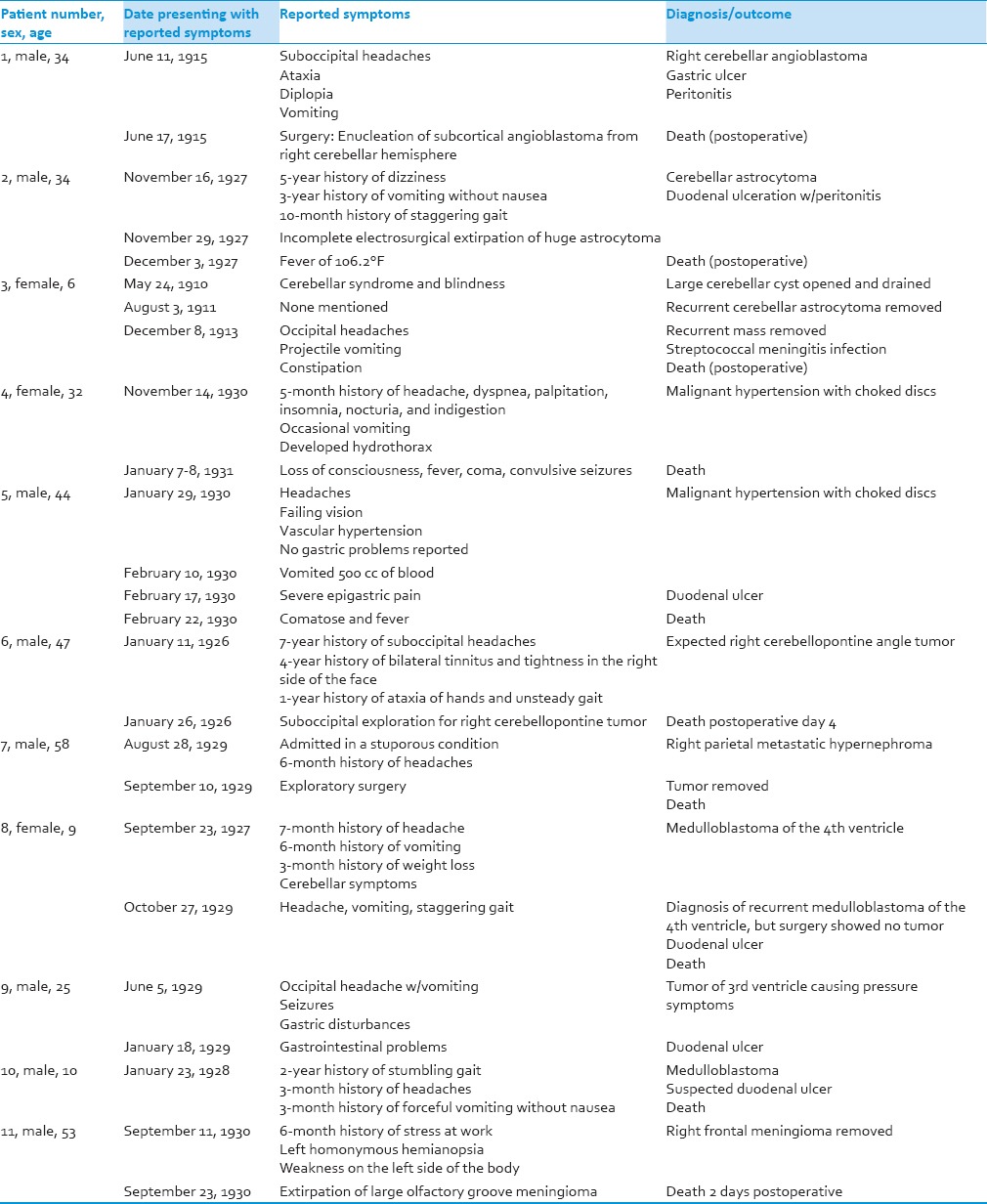
All patients listed below are described in Cushing's article, “Peptic ulcers and the interbrain"[4] unless otherwise specified.
Patient 1
This case is described in Cushing's original Yale Registry[5] and Cushing's article, “Peptic ulcers and the interbrain.”[4] Patient 1, a 34-year-old man, presented in June 1915 with a 6-week history of unsteady gait associated with a 4-month history of nausea and vomiting. He also reported having midline suboccipital headaches starting in December 1914. The patient was diagnosed with a subcortical angioblastoma arising from the right cerebellar hemisphere. Cushing employed a bilateral suboccipital exploration that exposed both cerebellar hemispheres. He punctured the left lateral ventricle to lower the tension. Cushing reported “the dorsum and posterior clinoid processes show signs of pressure atrophy with destruction.”[1] Pathologist W. T. Councilman diagnosed the intracranial mass as a “mixed tumor, possibly glioma-hemangioma.” Postoperatively, the patient described abdominal discomfort and vomited a bile-stained fluid. His postoperative abdominal exam showed it to be “somewhat spastic and with quite marked tenderness in the epigastrium.”[1] Dr. Cushing admitted that not much attention was paid to the finding given the patient's “neurotic disposition” emerging from the effects of ether.
During the evening, the patient had more severe cramp-like pain in the stomach with a rectal temperature of 102.4°. Morphine was administered multiple times. By early morning, the patient's temperature rose to 104°. Cushing described the patient as “cyanotic, breathing very rapidly and shallow and pulseless.” The patient died later that morning. Cushing's impression was an acute peritonitis of unknown origin.[5]
It appears that pathologist W. T. Councilman had difficulty explaining the abdominal pathology and described “submucosa [as] hemorrhagic and appears to have been torn by mechanical violence… the muscularis is usually intact, but in many places, this also has ruptured… It is hard to explain the condition of the stomach, both gross and microscopically, except as a result of a mechanical action tending to stretch all layers.”[5] According to the postmortem exam performed by Dr. J. L. Stoddard, the peritoneal cavity showed signs of fibrinous peritonitis in the upper abdomen and three circular gastric perforations between the cardia and pylorus. He reports that the gastric interior appeared to have been affected by corrosive poisoning.[4]
Patient 2
Described in Cushing's original Yale Registry[1] and Cushing's article, “Peptic ulcers and the interbrain,”[4] Patient 2 was a 34-year-old man who presented with cerebellar signs and symptoms in November 1927. This was Dr. Cushing's second case of postoperative duodenal ulceration with perforation, 12 years after patient 1. Patient 2 reported a 5-year history of pain in the posterior neck and dizziness on bending over with diplopia, and said he had experienced weakness, numbness, and loss of control of his right arm and leg for about 10 months. He also reported four seizures, loss of consciousness, and a 3-year history of intermittent vomiting.
On exam, the patient had bilateral papilledema, ataxia, and sustained nystagmus. The patient was found to have a right partially cystic cerebellar astrocytoma. According to Dr. Cushing's operative note, the tumor could be easily separated from the cerebellar hemispheres via electrosurgery. A few days later, the patient experienced intense epigastric pain, and rectal temperature elevated to 102.4°. By the following morning, his temperature had risen to 106.2°. No vomiting had occurred, and he died 4 days postoperatively.
According to Dr. G. A. Bennett, postmortem exam demonstrated a “residual mass of nonadherent tumor deeply indenting and flattening the medulla.” The peritoneal cavity had 1100 cc of a dark red-brown fluid and two irregularly-shaped perforations in the duodenal wall 3 cm from the pylorus. Microscopic examination of the tissue near the perforated areas demonstrated an acute inflammatory process and “showed a completely destroyed mucosa… replaced by an exudate of fibrin, inflammatory cells, and blood.”[4,5] According to Bennett, these destructive lesions were the result of vascular thrombosis, commonly believed to be the cause of duodenal ulcers.[5]
Patient 3
Patient 3 initially presented in May 1910 with advanced cerebellar syndrome and blindness. He had surgery to open a large cerebellar cyst and was asymptomatic for 1 year. In August 1911, the patient had a large, recurrent cystic tumor partially removed. In December 1913, the patient was admitted and had a recurrence of symptoms, including occipital pain, projectile vomiting, and constipation. A third operation was performed, and the patient died 6 days after surgery due to streptococcal meningitis. Autopsy reported several areas in the stomach where the mucus membrane was absent, the largest being 3 mm in diameter.
Patient 4
Patient 4, a 32-year-old woman, presented in November 1930 with stress, an enlarged heart, moderate arteriosclerosis, papilledema, and a significantly elevated blood pressure of 270/150. On admission, she reported a 5-month history of headache, dyspnea, palpitation, and indigestion. Eventually, the patient developed hydrothorax that was relieved by a tap. On January 7, 1931, she became comatose, febrile, and suffered convulsive seizures. She died on January 8 with a temperature of 104°. The autopsy reported “gastric mucosa was found to be intensely injected and to contain numerous, small stellate-shaped recent ulcerations… The mucosa of the duodenum was injected but without ulceration.”[4] This patient had a hypertensive crisis that caused gastric ulceration, not due to surgical intervention.
Patient 5
Patient 5, a 44-year-old man, presented in January 1930 with headaches and declining vision for the previous year. Blood pressure was 210/145 and on exam, there was evidence of long-standing papilledema. Ventriculograms did not show any evidence of a tumor. On February 10, the patient vomited a total of 1300 cc of blood over the course of 2 days. On February 17, the patient experienced intense epigastric pain warranting exploratory surgery. Dr. John Powers found “a perforation in the posterior wall of the stomach 1 cm in diameter and 8 cm proximal to the pylorus.”[4] This ulcer was surgically closed. The patient died on February 22 with a rectal temperature of 104°. Postmortem exam showed “peritonitis restricted to the lesser peritoneal cavity with terminal septicemia from a gas-producing bacillus… The sutures closing the perforation had been dissolved away, and the stomach was in shreds from autodigestion.”[4] No tumor was found.
Patient 6
Patient 6, a 47-year-old man, presented on January 11, 1926, with a 7-year history of suboccipital headaches, a 4-year history of bilateral tinnitus, a 1-year history of ataxia, and a 2-3 months history of right facial palsy and constipation. Exam showed papilledema, nystagmus, moderate bilateral deafness, cerebellar ataxia, and absent gag reflex. Blood pressure was 140/80. A tumor was suspected, but exploration found none. During the surgery on January 26, the patient experienced vomiting and a fall in blood pressure. Cushing noted the absence of cerebellar tonsillar herniation, and he also noticed evidence of upward herniation of the spinal cord.
On postoperative day 3, the patient's temperature rose to 104°. Lumbar puncture revealed mildly blood-tinged fluid. The patient's lungs filled with fluid, and he became cyanotic, eventually leading to his death on postoperative day 4. The autopsy reported an aneurysm of the basilar artery that displaced the brainstem, arteriosclerosis, bronchopneumonia, and gastromalacia. A postmortem exam found “the peritoneal cavity [near] the spleen contained 500 cc of brownish dirty fluid containing small masses of mucus. The fundus of the stomach and lower esophagus was found to be completely disrupted and in shreds.”[4] The gastric perforation was found to be 15 cm in diameter, extending to the cardia of the stomach and entering the esophagus.[4] The presence of brown fluid showed that gastric secretions had been released for some time, allowing for perforation of the stomach.
Patient 7
Patient 7, a 58-year-old man, presented in August 1929 because of a stuporous condition following a 6-month history of headaches. On September 10, Dr. Horrax performed an exploratory procedure and enucleated a metastatic hypernephroma. The patient's condition worsened the next day. His stupor continued with a 104° fever. Dr. Cushing was concerned that a postoperative clot had formed. Despite re-elevation of the flap, the patient remained unconscious, and upon receiving a nasal feeding tube, he regurgitated a large amount of dark brown blood and died. Postmortem exam reported edema of the right cerebral hemispheres. Cushing reported “a bilateral perforation of the esophageal wall communicated with the right and left pleural cavities, each of which contained about 400 cc of brownish mucoid fluid… The margin of the digested area in the thorax showed a border of reddening suggesting that the circulation must have been in… the early stages of the process… [and that] the fundus of the stomach was highly necrotic.”[4] Gastric release must have occurred for a long time before blood was regurgitated with gastric fluid.
Patient 8
This case is described in Cushing's original Yale Registry[5] and Cushing's article, “Peptic ulcers and the interbrain.”[4] Patient 8, a 9-year-old girl, was admitted in September 1927 with an advanced cerebellar tumor syndrome. She had a 7-month history of frontal headaches, a 6-month history of projectile morning vomiting, weight loss, and ataxia. Physical exam also showed weakness of the upper branch of the left facial nerve, bilateral papilledema, and tortuous fundi vessels. Cushing suspected that a cerebellar tumor caused the increased intracranial pressure and papilledema.
Cushing proceeded with a bilateral suboccipital exposure and found the bone and dura covering the cerebellum to be thin. He inserted a needle into the left ventricle and fluid shot out of the manometer. Cushing found the tumor to have an interior cavity that contained “soft yellowish masses of degenerated tissue” and was able to separate the tumor from the fourth ventricle. Pathologist G.W. Bennett reported that the tumor “shows a pseudoadenomatous structure and a few pseudorosettes.”[5] The child was found to have a median cerebellar medulloblastoma. For the next 2 years, the patient continued to vomit 2-3 times/week and experienced weight loss.
The patient was admitted again in July 1929 with complaints of headache, vomiting, and staggering gait, suggestive of increased intracranial pressure caused by a recurrence of the medulloblastoma. Exam showed positive Romberg, unsteady gait, nystagmus, and some forgetfulness. She improved with X-ray therapy and was discharged in August, but was readmitted in September. 10 days before admission, the patient had refused to feed herself, lost interest in her environment, and had urinary and fecal incontinence. She also was drowsy with daily vomiting and right occipital headaches. According to Dr. Oldberg, physical exam showed drowsiness, apathy, bilateral papilledema, right oculomotor palsy with diminution and/or disappearance of other deep reflexes. On October 10, 1929, an exploratory procedure was performed on the cerebellar region. The procedure was unable to show local recurrence. The first specimen showed “a mass of calcified, degenerated tissue.” Fluid from a lateral ventricular tap failed to show any tumor cells, but did show many red blood cells. On October 27, the patient fell into a coma with a temperature of 106.5° and died.
Autopsy report notes “in the first portion of the duodenum approximately 3 cm below the pyloric sphincter, there is a small area which has a definite elevated margin with a depressed center forming more or less of a crater. The crater measures 3 cm × 4 cm in its greatest diameters… One section of the duodenum shows the ulcer… extends down to the muscularis, and its margins are deep… there is a narrow zone of dense hyalinized connective tissue… and some fibrin and red blood cells.”[4,5]
Postmortem examination of the patient's brain showed obstruction of the ventricular system by a recurrent medulloblastoma. Blood culture and brain base culture grew multiple colonies of Staphylococcus aureus which could indicate meningitis. Autopsy showed “very little purulent exudate over… cerebral hemispheres.”[4,5]
Patient 9
Patient 9, a 25-year-old man, presented in June 1929 with suboccipital headaches associated with vomiting. The patient reported that in May 1929, while fatigued from a long car drive, he endured a severe suboccipital headache and vomiting. He also experienced seizures that consisted of neck retraction, dizziness, sweating, eye protrusion, and arm flexure. Cushing wrote that the patient was reportedly taken to the hospital in late May for “gastric symptoms.”[4] On examination, the patient had a rigid neck, bilateral abducens palsy, bilateral Babinski reflex, hyperreflexia, and a choked disc of 4 diopters. Ventriculograms showed some evidence of obstructive hydrocephalus at the foramina of Monro and a filling defect of the third ventricle. He was given four radiation (X-ray) treatments and the pressure symptoms subsided for 1 year.
In 1931, his gastric symptoms returned, and a recurrence of the tumor was suspected. He received three additional radiation treatments, and the symptoms disappeared. However, the symptoms recurred again in January 1932. These symptoms were more indicative of a duodenal ulcer. He received radiation at the third ventricle, and he improved. However, several weeks later on March 3, barium studies confirmed the presence of a healed duodenal ulcer following the radiation therapy.[4]
Patient 10
Patient 10, a 10-year-old boy, presented with a 3-month history of ataxia and clumsiness, a 6-month history of dysarthria, and a 3-month history of suboccipital headaches and vomiting. Physical exam showed secondary optic atrophy, nystagmus, left facial nerve paresis, slurring of speech, and marked ataxia. Cushing suspected a cerebellar tumor. In surgery, there was a “protruding, bleeding, cavernous angioma which burst its way (through) the left cerebellar hemisphere as soon as an incision was made [through] the dura in spite of the ventricular puncture.”[5] The patient's blood pressure fell rapidly. Postmortem examination of the mediastinum was performed on the operating room table following the patient's death. Cushing reported “the whole fatty contents of the mediastinum had been completely digested away leaving the aorta exposed, the plexus of sympathetic nerves free and naked as though they had been dissected out.”[5] Cushing also wrote that a 1-inch slit was found in the esophagus, allowing gastric contents to “leak out.” He reported: “I cannot believe that the perforation in this child was due to anything else than a digestive ulcer of the esophagus… the dissection appearance of the structures in the mediastinum was much more likely to have been produced by a digestive process…”[1] This patient was also mentioned in Cushing's paper, “Peptic ulcers and the interbrain,” in which he discussed 11 patients suffering from both intracranial and gastric lesions.[4]
Patient 11
Patient 11, a 53-year-old man who presented in September 1930, reported working under stress, suffering emotional distress, and vomiting at work over a period of 6 months. Exam showed left hemiparesis, left homonymous hemianopsia, and impaired memory. Dr. Cushing took the patient to surgery to remove nodular meningioma in the right frontal lobe. Surgery was complicated by hemorrhage due to tearing of the anterior cerebral artery segments embedded in the tumor. This resulted in bilateral spastic paralysis. A nasal tube withdrew 50 cc of coffee-ground material with red blood cells evident on microscopy. 2 days after surgery, the patient's temperature dramatically rose to 107°, he “vomited a large amount of bloody fluid,”[4] and died.
On postmortem examination, Dr. Schulz reported that in the stomach, there were “numerous flecks of the coffee-ground material suggesting changed blood.” Numerous ulcerations “very superficial and were found scattered… both in fundic and pyloric regions.”[4] Microscopic exam did not show “evidence of the arterial or capillary disease or any noteworthy constriction of or thrombosis of the vessels,” unlike the previous cases.[4]
New Patient Reports
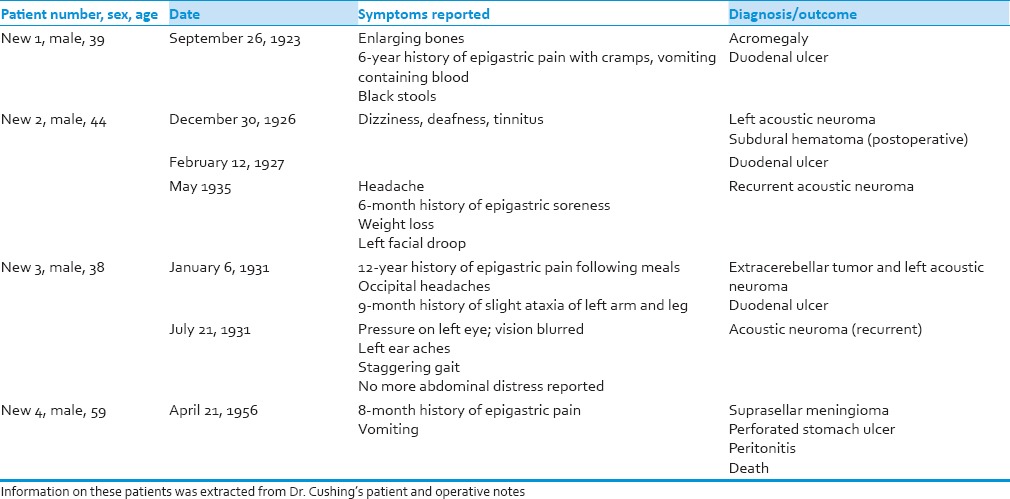
The descriptions of the following patients were never published by Cushing [Table 2]. This information was directly extracted from Dr. Cushing's patient and operative notes. All patients listed below are described in Cushing's original Yale Registry[5] unless otherwise specified.
Table 2.
Description of Dr. Cushing's newly described gastro-duodenal ulcer patients
New patient 1
New patient 1, a 39-year-old man, presented in September 1923 with acromegaly. In 1914, he had a “stroke” that caused right facial droop and loss of sensation. The loss of sensation improved, but the patient reported that his jaw kept “growing out.” He reported that in 1917, he started having “constant dull epigastric pain with exacerbations of cramps… vomiting of both ingested food and large amounts of clear fluid… vomitus contained bright red blood.” Patient also noted that his stools were black in color. In Dr. Cushing's note, he writes that the patient's “bones kept growing larger everywhere… became associated with aches and pains all over his body.” Physical exam showed signs of enlargement of bony prominences, irregular and unequal pupils, and tenderness in the epigastric, left iliac, and umbilical regions. X-ray showed the pituitary fossa to be depressed and irregular, suggestive of a pituitary tumor causing acromegaly.[5] The patient was treated nonsurgically with multiple X-ray exposures.
In October 1923, Cushing's resident, N. C. Stosman, performed gastric studies and found the “stomach to be active in peristalsis, emptying quite rapidly… the patient's duodenal cap was constantly irregular, showing a definite constriction, with more or less a pouch on the inferior curvature.”[5] Stosman reported that the findings suggested a duodenal ulcer. Patient was released from the hospital with dietary instructions and sodium bicarbonate, magnesium oxide, and calcium.[5]
New patient 2
New patient 2, a 44-year-old man, presented on December 30, 1926, with onset of dizziness, deafness, and tinnitus worse in the left ear.[5] He was diagnosed with a left acoustic neuroma. In February 1927, he was diagnosed with a duodenal ulcer, the same year the acoustic neuroma was partially excised by Dr. Cushing. In May 1935, he complained of headache that corresponded to exaggerated hypertension and a 6-month history of epigastric soreness, likely due to the duodenal ulcer diagnosed in 1927. He was referred for possible symptoms of recurrent acoustic neuroma. He was treated with dietary modifications and powder that gave him some relief. Physical exam in May 1935 showed that the patient had lost a significant amount of weight and left facial droop. It appeared that the left acoustic neuroma had recurred.[5]
On May 25, 1935, re-exploration of the left cerebellar region occurred. The recurrent tumor was found to be close to the “midline with obvious extensions of it going out into the cerebellar hemisphere and up towards the opening in the tentorium.” Cushing decided that it would be too risky to pursue complete resection of the mass. The tissue was removed, and muscle graft was used on the closure with appropriate layers. Postoperatively, the patient did well though initially experienced hiccups. A gastric suction tube was inserted without relief. The patient received fluids and sodium bicarbonate via nasogastric tube and improved. Objective findings on postoperative physical exam showed moderate choking of optic discs, complete anesthesia of the left side of the tongue with left deviation, complete left facial paralysis, and complete left deafness, among other findings.[5]
New patient 3
New patient 3, a 38-year-old man, presented in January 1931 with a 12-year history of dull epigastric pain after meals, 1-year history of occipital headaches, and a 9-month history of slight ataxia of the left arm and leg. The patient reported being previously admitted to the hospital in September 1930 for epigastric pain. He reported a 7-year history of “falling auditory acuity in the left ear following an episode of otorrhea, otalgia, and tinnitus.”[5] Physical exam revealed slight occipital tenderness, left cerebellar nystagmus, ataxia of left arm and leg, and bilateral papilledema. On October 4, 1930, according to patient notes, Dr. Horrax performed a suboccipital exploration with “intracapsular enucleation of a tough, fibrous low-lying [left] acoustic neuroma.” After this surgery, it was discovered that the patient's left eardrum had been perforated, and a purulent discharge had formed. The patient had 2 cc of surgical pituitrin injected into the lateral horn of the left ventricle. He was discharged in November 1930 with decreased headaches and subjective improvement in vision and ataxia. On physical exam, the papilledema persisted and nystagmus, ataxia, and the left cranial nerve VI weakness matched the preoperative exam. A diagnosis of extra-cerebellar tumor and left acoustic neuroma was made. 6 weeks after his first discharge in January 1931, he suffered occasional occipital headaches, vomiting and dull, uncomfortable pain in the epigastrium occurring before meals and relieved with food.[5] According to the patient notes, the impression was probably a residual acoustic neuroma. However, this was unlikely the case. It is suspected that the patient was suffering from a duodenal ulcer based on clinical history and physical exam. After his second discharge, the patient reverted to a “sippy diet” and powders for 1 week. Eventually, the patient shifted to a regular diet. In July 1931, he denied vomiting and reported that his abdominal pain and appetite had improved with some abdominal tenderness and pain. The ataxia persisted, and his left ear had a “sense of hearing a waterfall in the distance.”
New patient 4
New patient 4, a 59-year-old man, presented in April 1926 with intense epigastric pain and vomiting for 4 days.[5] Patient reported that he had epigastric pain at 30-min intervals for the previous 8-9 months, but the current episode was the most severe. The episodes sometimes involved vomiting but no blood. Cushing's notes report that the patient had not voided or had a bowel movement for 24 h. Physical exam revealed tachypnea, “faint, sustained point of maximal impulse just above the nipple, weak heart sounds, weakened pulses, and a scaphoid abdomen with marked tenderness in the epigastrium.”[5] The impression was a perforated gastric ulcer with acute peritonitis.
If performed, surgery would have resulted in the patient's death. The patient was given morphine and eventually expired. The condition of Dr. Cushing's patient has made it difficult to understand the complete sequence of events. Postmortem examination reported: “[esophagus], stomach, gall bladder, and duodenum were removed together. The mass membrane is normal except for the ulcer situated on the anterior surface of the stomach near the pylorus and toward the lesser curvature. There is very marked induration around the perforation.”[1] The postmortem exam of the brain showed “normal pituitary gland [but] attached to the dura next to it (was) a small tumor… a typical dural endothelioma.”[5]
Increased Intracranial Pressure Causing Vagal Overstimulation
These case reports suggest a clinical correlation between brain tumors and gastro-duodenal ulcers. As previously mentioned, this may be due to the increase in intracranial pressure caused by a tumor, neurosurgery, or brain injury. According to Cushing, experimental lesions in the hypothalamic tracts leading to the vagal center can cause parasympathetic stimulation or sympathetic paralysis.[4] Another theory that Cushing proposed was that patients with postoperative vomiting produce bile and acid causing hemorrhagic ulceration. He also proposed a link between gastric erosions and malignant hypertension. In one particular study, he suggested that posterior fossa cerebellar surgeries produced gastric ulcers due to disturbance of the fiber tracts in the brainstem.[4]
According to Lewis, the two pathways implicated in the onset of duodenal ulceration are parasympathetic stimulation via the vagus nerve or sympathetic paralysis via pituitary-adrenal axis by corticosteroid release. The former is more likely. Stimulation of the vagus nerve increases parietal cell activity in the stomach or by increasing gastrin release. Edema will have a significant impact on the hypothalamus and brainstem. This can cause displacement of the vessels and indirectly affect the vagal nuclei. The vagal area is located mostly in the anterior hypothalamus while the sympathetic responses are controlled mostly by the posterior hypothalamus. Overstimulation of either area will cause disturbances. Further evidence supporting the parasympathetic overstimulation theory is evident by the fact that vagotomy or extra-ventricular drainage resolves the problem of duodenal ulceration.[2]
There are also studies showing linkage between brain damage and gastrointestinal problems. Watts and Fulton reported that monkeys with a specific hypothalamic injury were found to have gastrointestinal difficulties. However, their experiments did not confirm a relationship between the injury of any specific hypothalamic nuclei and changes in the gastro-intestinal tract. All but one of the monkeys that had erosions in the alimentary canal had a large lesion in the hypothalamus. The authors believed the erosions were due to local ischemia following “hyperactivity of the sympathetic vasoconstrictor mechanism of the gut.”[6] Building on the progress of Watts and Fulton, Hoff and Sheehan later showed that hypothalamic lesions may lead to the destruction of the sympathetic centers or by stimulation of the parasympathetic pathways in the brain. Destruction of the sympathetic centers would release the vagus nerve from antagonistic control. Hoff and Sheehan report that after hypothalamic injury, 5 monkeys, from a group of 16, had multiple erosions in the body of the stomach. No duodenal erosions were found.[7]
Providing more clinical evidence of the link between gastritis and duodenitis and intracranial injury, Larson et al. reported that patients enduring severe head injury did secrete more gastric acid than other nontrauma patients.[8] However, the difference was statistically insignificant. They found that head injury specifically seems to increase pancreatic polypeptide release and enhancing vago-cholinergic activity. They found statistically significant higher levels of pancreatic polypeptide in patients with severe head injury compared to the control trauma patients.[8]
In the light of these prior studies, it may be assumed that no single area of the brain or hypothalamus controls gastric function that leads to ulceration. However, the pathways involving the cortex, thalamus, and hypothalamus, all play a role in the activation of the parasympathetic and sympathetic nervous systems.[9]
Clinically shown by Cushing's Yale Registry, a tumor or lesion can disrupt this circuitry, leading to gastroduodenal ulceration. Cushing said that it was “reasonable to believe, therefore, that the perforations following posterior fossa cerebellar operations forming the basis of this study were produced in like fashion by an irritative disturbance either of fiber tracts or vagal centers in the brain stem.”[4] Above all, Harvey Cushing's pioneering work depicted in his Yale Registry serves as a milestone for continuing research that can further discern this pathway.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Cheung LY. Thomas G Orr Memorial Lecture. Pathogenesis, prophylaxis, and treatment of stress gastritis. Am J Surg. 1988;156:437–40. doi: 10.1016/s0002-9610(88)80522-1. [DOI] [PubMed] [Google Scholar]
- 2.Lewis EA. Gastroduodenal ulceration and haemorrhage of neurogenic origin. Br J Surg. 1973;60:279–83. [PubMed] [Google Scholar]
- 3.Wijdicks EF. Cushing's ulcer: the eponym and his own. Neurosurgery. 2011;68:1695–8. doi: 10.1227/NEU.0b013e318212babf. [DOI] [PubMed] [Google Scholar]
- 4.Cushing H. Peptic ulcers and the interbrain. Surg Gynecol Obstet. 1932;55:1–34. [Google Scholar]
- 5.Cushing H. New Haven, CT: Yale University; Cushing Brain Tumor Registry. Archived by Yale School of Medicine. [Google Scholar]
- 6.Watts JW, Fulton JF. The effect of lesions of the hypothalamus upon the gastro-intestinal tract and heart in monkeys. Ann Surg. 1935;101:363–72. doi: 10.1097/00000658-193501000-00037. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Hoff EC, Sheehan D. Experimental gastric erosions following hypothalamic lesions in monkeys. Am J Pathol. 1935;11:789–8023. [PMC free article] [PubMed] [Google Scholar]
- 8.Larson GM, Koch S, O’Dorisio TM, Osadchey B, McGraw P, Richardson JD. Gastric response to severe head injury. Am J Surg. 1984;147:97–105. doi: 10.1016/0002-9610(84)90041-2. [DOI] [PubMed] [Google Scholar]
- 9.Long DM, Leonard AS, Chou SN, French LA. Hypothalamus and gastric ulceration. Arch Neurol. 1962;7:167–75. [Google Scholar]