

Abstract
Purpose
We performed a comparative analysis of the clinicopathologic features and oncologic outcomes of colorectal cancer patients with metachronous versus synchronous metastasis, according to the prognostic factors.
Methods
Ninety-three patients who underwent curative resection for distant metastatic colorectal cancer were included in the study between December 2001 and December 2011. We assessed recurrence-free survival and overall survival in patients with distant metastasis who underwent curative surgery.
Results
The most common site of distant metastasis was lung alone (n = 19, 51.4%) in patients with metachronous metastasis, while liver alone was most common in those with synchronous metastasis (n = 40, 71.4%). Overall survival rate was significantly different between patients with synchronous metastasis and metachronous metastasis (34.0% vs. 53.7%; P = 0.013). Incomplete resection of the metastatic lesion was significantly related to poor overall survival in both, patients with synchronous metastasis, and metachronous metastasis.
Conclusion
Our study indicates that patients developing distant metastasis after initial treatment show a different metastatic pattern and better oncologic outcomes, as compared to those presenting with distant metastasis. Resection with tumor free margins significantly improves survival in patients with metachronous as well as synchronous metastasis.
Keywords: Colorectal neoplasms, Metastasis, Metastasectomy
INTRODUCTION
Colorectal cancer can metastasize to the liver, lung, ovary, peritoneum and other organs systemically. Approximately 20% of patients with colorectal cancer have distant metastasis (DM) at the time of presentation [1]. Additionally, among those patients who undergo curative resection of the primary tumor, nearly a third will develop recurrent disease. DMs in patients with colorectal cancer are the main cause of cancer-related mortality. Although management of metastatic colorectal cancer has been based on systemic chemotherapy, surgical resection in selected patients with metastatic colorectal cancer offers the only possibility for long-term survival. Traditionally, patients with limited hepatic or pulmonary metastases have been considered the only candidates for surgical resection. Recently, with the advances in chemotherapy, surgical technique and curative surgery for selected patients, outcomes of patients with metastatic colorectal cancer have improved. While most studies on oncologic outcomes in patients with DM have included those with synchronous metastasis [2,3,4,5], there are few studies on those who developed metastasis after initial treatment [6,7]. Moreover, the definition of synchronous and metachronous metastasis was not definite in previous studies [2,3,4,5,6,7]. Therefore, it is not clear whether patients with metachronous metastasis represent a different category, as compared to those with synchronous metastasis. Very few studies have compared the clinicopathologic features between patients with metachronous metastasis and synchronous metastasis [6,7].
The aim of this study is to compare the clinicopathologic features and oncologic outcomes between patients with metachronous metastasis and synchronous metastasis.
METHODS
Ninety-three patients who underwent surgical resection for distant metastatic colorectal cancer were included for analysis of oncologic outcome between December 2001 and December 2011.
Presenting with DM at initial diagnosis was defined as DM detected by preoperative screening or during resection of the primary tumor. Developing DM was defined as DM detected after primary operation. However, all patients recurred ≥6 months after primary operation. Therefore, patients presenting with DM were considered as synchronous metastasis and those developing DM, as metachronous metastasis. Patients were divided into 2 groups: synchronous metastasis and metachronous metastasis.
Variables included patient demographic factors (e.g., age, gender), tumor factors (e.g., grade, depth of invasion, regional lymph node metastasis, tumor location, tumor size, number of liver or lung metastasis, and site of DM). We assessed the 5-year RFS and OS in patients with DM who underwent surgical resection. The study was approved by our Institutional Review Board.
Lesions were detected using CT, MRI, and PET. Metastasectomy was indicated when preoperative staging showed that margin negative resections could be achieved among patients fit to undergo major surgery. A complete examination of the abdomen was performed by intraoperative palpation and inspection to rule out other lesions that were missed by preoperative investigations. Hepatic resections were performed by either anatomic or non-anatomic resections. Intraoperative ultrasound was carried out to confirm the findings of preoperative imaging and to assist in surgical planning during hepatic resection. Hepatic resection was performed using the Cavi-Pulse ultrasonic surgical aspirator (CUSA, Model 200T, Valley Lab., Boulder, CO, USA). Pulmonary resections were performed by either anatomic or nonanatomic resections using open thoracotomy or video-assisted thoracoscopic surgery.
Following diagnosis of DMs, chemotherapy was given to 90 patients (96.4%); 3 patients (3.6%) refused chmeotherapy. The regimens of first-line chemotherapy for DM were: oxaliplatin combined with infusion of 5-fluorouracil (5-FU)/leucovorin (LV), n = 62; irinotecan combined with infusion of 5-FU/LV, n = 13; capecitabine, n = 9; and miscellaneous regimen, n = 6.
The follow-up examinations included physical examinations and serum CEA assay. Chest x-ray, abdominopelvic CT, and colonoscopy were performed 6 months postoperatively and annually thereafter, as well as on suspicion of recurrence. Chest CT was performed annually after the operation. PET was performed on suspicion of recurrence.
The primary endpoint was recurrence-free survival (RFS) and overall survival (OS). Patients were followed up every 3 months until death or the cutoff date (July, 2014). Median follow-up time was 43.0 months (range, 11-129 months).
Pearson chi-square or Fisher exact test was used to assess differences in the clinicopathologic features. Continuous data were compared by Student t-test. Kaplan-Meier survival analysis with the log-rank test was used to evaluate the prognosis of colorectal cancer with DM. Variables with a P-value < 0.20 in the univariate analysis were included in the multivariate analysis. Multivariate analysis was performed with the Cox regression analysis for OS. Statistical analysis was performed using the SPSS ver. 13.0 (SPSS Inc., Chicago, IL, USA). A P-value of ≤0.05 was considered statistically significant.
RESULTS
Clinicopathologic characteristics
Table 1 summarizes the characteristics of the patients with colorectal cancer DM who underwent metastasectomy from December 2001 to December 2011. Of the 93 patients with colorectal cancers included in the study, 56 patients presented with DM and 37 patients developed DM after resection of primary tumor. The median age of patients with metachronous metastasis was 57.0 years, as compared to 55.5 years for those with synchronous metastasis (P = 0.626).
Table 1. Clinicopathologic characteristics.
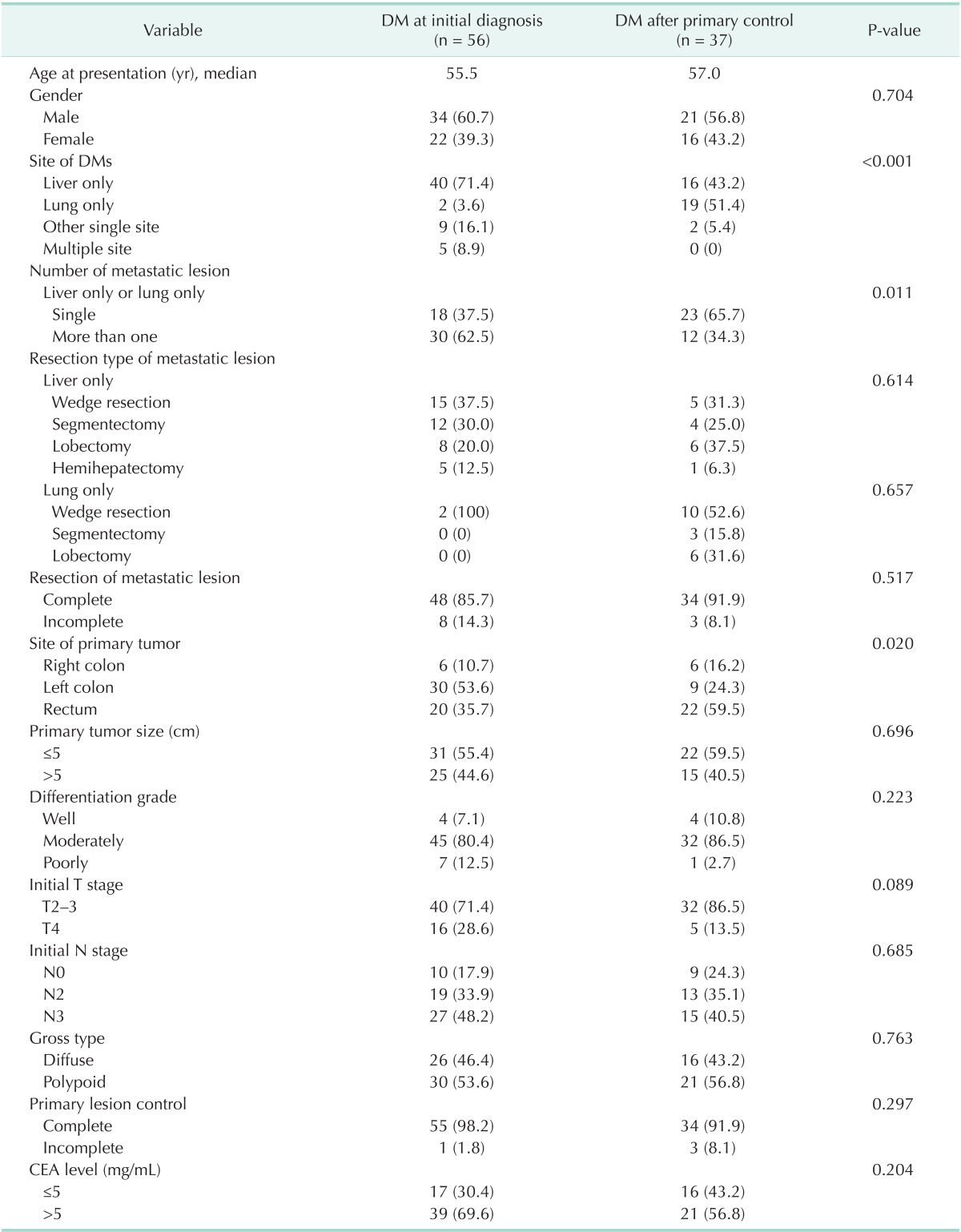
Values are presented as number (%).
DM, distant metastasis.
There were no significant differences between the 2 groups in terms of age, gender, resection margin of metastatic lesion, histological grade, initial T stage, initial N stage, gross type, resection margin of primary lesion, and CEA level. The most common site of DM was lung alone (n = 19, 51.4%) in patients with metachronous metastasis, while liver alone was most common in those with synchronous metastasis (n = 40, 71.4%). The other single site was ovarian metastasis. Multiple site metastases included the metastases to ≥2 sites among ovary, lateral wall, small bowel, liver, lung, and pelvic wall. Eighty-two patients had complete resection of the metastatic lesion and incomplete resection was done in 11 patients. Primary tumor site was different between the 2 groups. Left colon was most common in patients with synchronous metastasis, while rectum was most common in patients with metachronous metastasis.
Survival analysis
Median follow-up time was 43.0 months (range, 11-129 months). There was no postoperative death at 30 days in either group.
Five-year RFS was not significantly different between patients with synchronous metastasis and those metachronous metastasis (28.5% vs. 30.8%, P = 0.291). Five-year OS rate was significantly different between patients with synchronous metastasis and those with metachronous metastasis (34.0% vs. 53.7%, P = 0.013).
Univariate analyses were performed to clarify the prognostic factors in all patients with DM, metachronous metastasis and synchronous metastasis (Table 2).
Table 2. Univariate analysis for recurrence-free and overall survival.
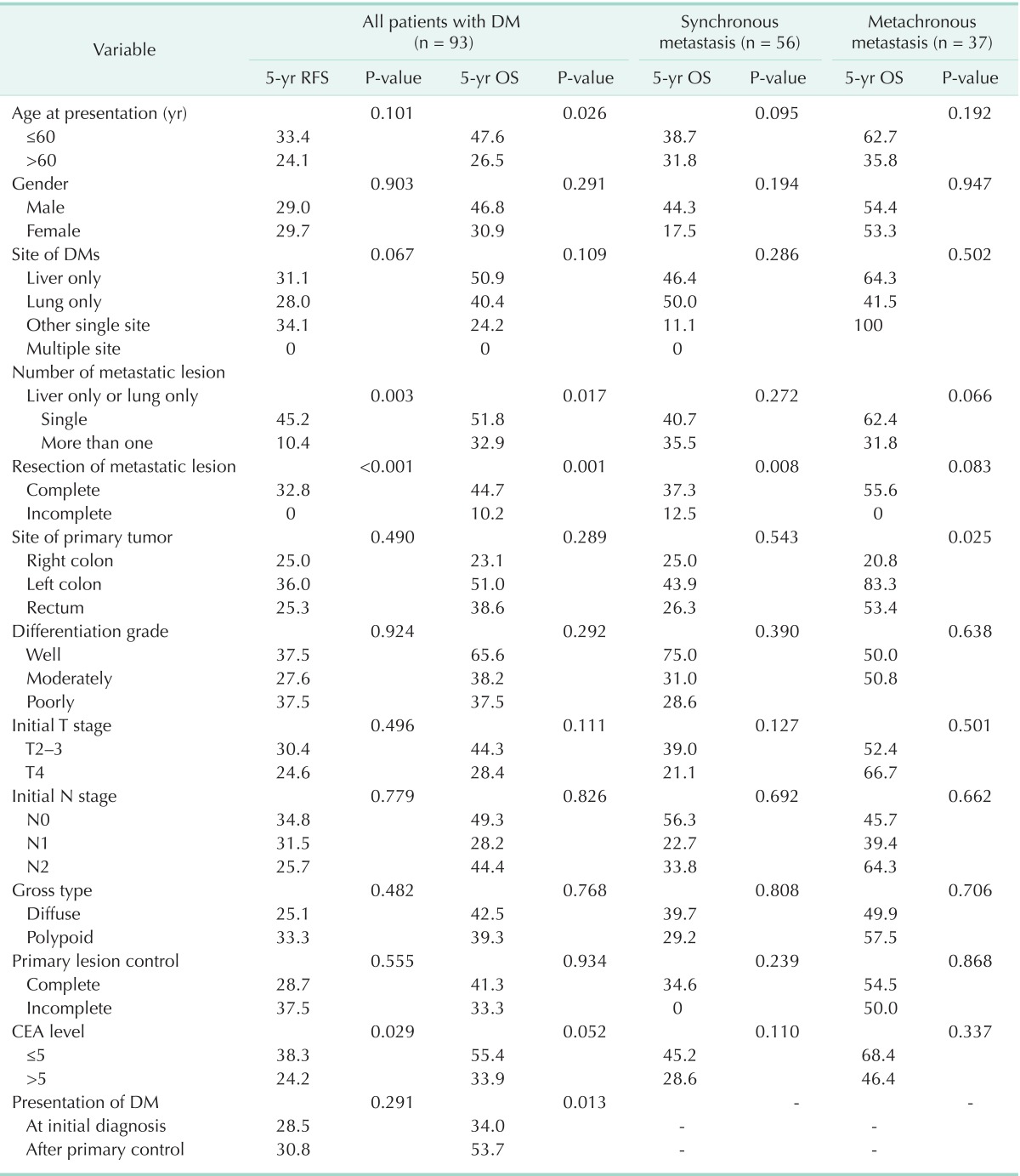
RFS, recurrence-free survival; OS, overall survival; DM, distant metastasis.
Age, site of DM, incomplete resection of metastatic lesion (hazard ration [HR], 3.452; 95% confidence interval [CI], 1.453-8.200; P = 0.005), number of metastatic lesion, and CEA level were independent risk factors for OS in patients with DM. Incomplete resection of metastatic lesion was an independent risk factor for OS in both patients with metachronous metastasis (HR, 16.636; 95% CI, 2.059-134.403; P = 0.008), and synchronous metastasis (HR, 3.530; 95% CI, 1.466-8.501; P = 0.005). Age and site of primary tumor was an independent risk factor for OS in patients with metachronous metastasis, while increased age was an independent risk factor in those with synchronous metastasis (Table 3).
Table 3. Multivariate analysis for overall survival.
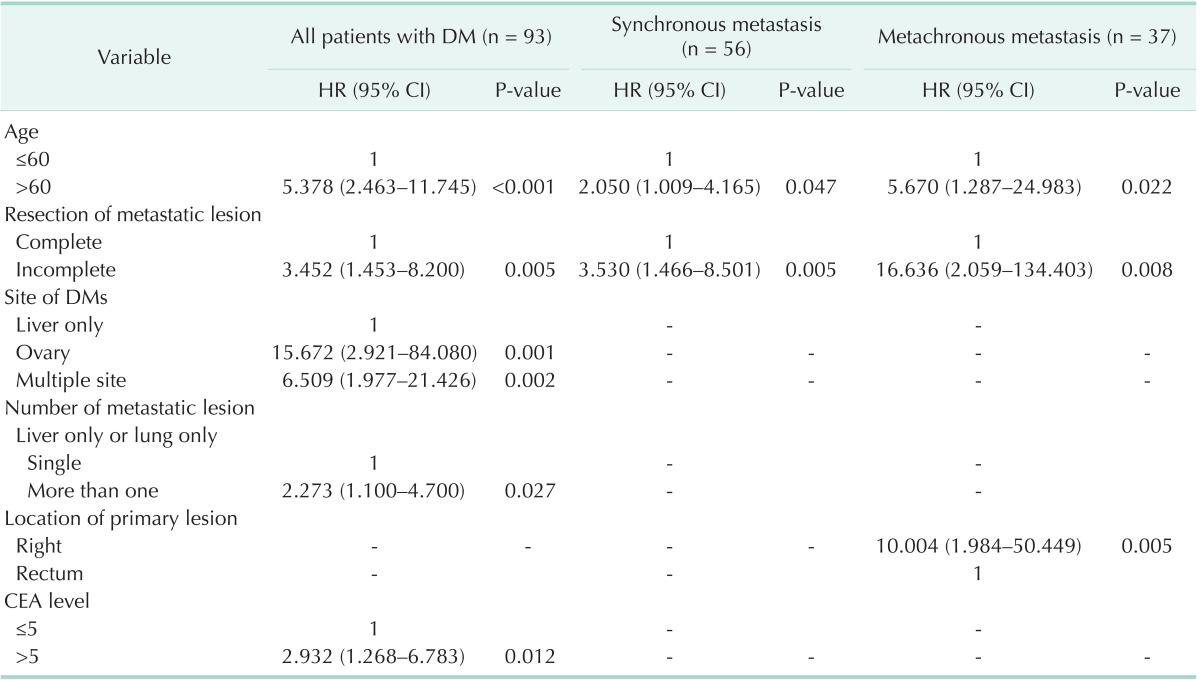
DM, distant metastasis; HR, hazard ratio; CI, confidence interval.
DISCUSSION
We compared clinicopathologic characteristics and oncologic outcomes between patients with metachronous metastasis and those with synchronous metastasis. Although most studies have reported oncologic outcomes in patients who presented with DM, few studies have investigated oncologic outcomes in patients with metachronous metastasis. Firstly, we analyzed a number of clinicopathologic factors, including the presentation timing of DM by univariate analysis to find prognostic factors in all patients with DM. We found that patients with metachronous metastasis had a better OS rate than those with synchronous metastasis by univariate analysis, but RFS was not different. Using a multivariate analysis, we found that the presentation timing of DM was not an independent predictor of poor OS. This is similar to previous studies, which likewise reported that metachronous metastasis is not a poor prognostic factor for survival [4,6]. However, these previous studies differed from ours in terms of inclusion criteria. Ng et al. [6] reported that a higher rate of multiple metastatic lesions led to less curative resection. They suggested that the poor prognostic outcome was overcome by perioperative chemotherapy. Van der Pool et al. [4] reported that although patients with synchronous metastases may have poorer biological characteristics, there was no difference in prognosis, as compared to those with metachronous metastases. They furthermore provided the rationale for significantly greater neoadjuvant chemotherapy in patients with synchronous metastasis.
On the contrary, 2 recent studies reported that patients with metachronous tumors showed a significantly better prognosis than those with synchronous lesions [8,9]. Schule et al. [9] attributed the difference to the lower likelihood of complete resection in synchronous disease.
We investigated the reason for the better OS rate in patients with metachronous metastasis on univariate analysis. We concluded that it is due to difference in patients characteristics between the 2 groups. Among the prognostic factors for DM demonstrated by multivariate analysis, site of DM and the number of metastatic lesions were different between patients with metachronous metastasis and synchronous metastasis. We think that the multiplicity represents more disseminated disease resulting in a poorer prognosis that may contribute to poor OS in patients with DM. These results are compatible with several previous reports that the number of DM is of significant importance to survival, although prognostic factors included are not the same [7,10,11,12,13]. Many authors reported that metastatic lesion can be detected at an earlier stage in patients with metachronous metastasis [14,15]. This difference may contribute to better OS in patients with metachronous metastasis.
We found that hepatic metastasis was more common in patients with synchronous metastasis, while pulmonary metastasis was more common in those with metachronous metastasis. Furthermore, DM other than liver and lung were more common in patients with synchronous metastasis. The study demonstrated that the site of metastatic lesion was an independent risk factor of recurrence-free and OS. Our study suggests that this difference in metastatic sites may contribute to the difference in OS in patients with metachronous metastasis.
Recent advances in chemotherapy, surgical technique and curative surgery for selected patients have led to improved outcomes in patients with metastatic colorectal cancer. Patients with limited hepatic or pulmonary metastases have been considered the sole candidates for surgical resection. The overall 5-year survival rates are in the range of 37%-58% in the previous studies that reported the results of hepatectomy with curative intent [16,17,18]. Like hepatic metastases, complete resection of lung metastases is associated with prolonged survival in selected patients [12,19,20,21]. Ovarian metastases are rare, but easily resected and may benefit from surgical resection.
Although resection of isolated liver or lung or ovarian metastases from colorectal cancer appears to be beneficial, the value of aggressive surgical treatment for patients who develop multiple site DM is not well defined. It has been believed that metastatic involvement of >1 organ represents widespread tumor dissemination and leads to a reluctance in attempting metastasectomy. Our study confirms that metastatic involvement of ovary and >1 organ shows worse OS than hepatic involvement alone.
We also investigated the oncological outcome of patients who developed DM after initial surgical resection for DM.
Our study demonstrates that incomplete resection of the metastatic lesion is the most important factor for predicting the prognosis in patients with metachronous metastasis after treatment, as in those with synchronous metastasis. Positive resection margins were previously reported as an unfavorable prognostic factor [9,10,17,22,23].
This is a retrospective analysis of a small sample from our prospective database; we evaluated the clinicopathologic characteristics and oncologic outcomes of advanced colorectal cancer patients with metachronous metastasis, as compared to those with synchronous metastasis. There was thus a likely selection bias on inclusion criteria for surgical resection. However, our study suggested that the patients with metachronous metastasis can be treated with surgical resection with acceptable oncologic outcomes.
In conclusion, our study indicates that patients with metachronous metastasis show a different metastatic pattern and better oncologic outcome, as compared to those with synchronous metastasis. Resection with negative resection margin significantly improves survival in patients with metachronous metastasis as well as those with synchronous metachronous. We recommend curative surgical resection with negative resection margin in patients with metachronous metastasis. Further clinical trials are needed to identify biologic features in patients with metachronous metastasis.
Footnotes
CONFLICTS OF INTEREST: No potential conflict of interest relevant to this article was reported.
References
- 1.Jemal A, Siegel R, Ward E, Hao Y, Xu J, Murray T, et al. Cancer statistics, 2008. CA Cancer J Clin. 2008;58:71–96. doi: 10.3322/CA.2007.0010. [DOI] [PubMed] [Google Scholar]
- 2.Manfredi S, Lepage C, Hatem C, Coatmeur O, Faivre J, Bouvier AM. Epidemiology and management of liver metastases from colorectal cancer. Ann Surg. 2006;244:254–259. doi: 10.1097/01.sla.0000217629.94941.cf. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Miller G, Biernacki P, Kemeny NE, Gonen M, Downey R, Jarnagin WR, et al. Outcomes after resection of synchronous or metachronous hepatic and pulmonary colorectal metastases. J Am Coll Surg. 2007;205:231–238. doi: 10.1016/j.jamcollsurg.2007.04.039. [DOI] [PubMed] [Google Scholar]
- 4.van der Pool AE, Lalmahomed ZS, Ozbay Y, de Wilt JH, Eggermont AM, Jzermans JN, et al. 'Staged' liver resection in synchronous and metachronous colorectal hepatic metastases: differences in clinicopathological features and outcome. Colorectal Dis. 2010;12(10 Online):e229–e235. doi: 10.1111/j.1463-1318.2009.02135.x. [DOI] [PubMed] [Google Scholar]
- 5.Wang X, Hershman DL, Abrams JA, Feingold D, Grann VR, Jacobson JS, et al. Predictors of survival after hepatic resection among patients with colorectal liver metastasis. Br J Cancer. 2007;97:1606–1612. doi: 10.1038/sj.bjc.6604093. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Ng WW, Cheung YS, Wong J, Lee KF, Lai PB. A preliminary analysis of combined liver resection with new chemotherapy for synchronous and metachronous colorectal liver metastasis. Asian J Surg. 2009;32:189–197. doi: 10.1016/S1015-9584(09)60394-8. [DOI] [PubMed] [Google Scholar]
- 7.Tsai MS, Su YH, Ho MC, Liang JT, Chen TP, Lai HS, et al. Clinicopathological features and prognosis in resectable synchronous and metachronous colorectal liver metastasis. Ann Surg Oncol. 2007;14:786–794. doi: 10.1245/s10434-006-9215-5. [DOI] [PubMed] [Google Scholar]
- 8.Kumar R, Price TJ, Beeke C, Jain K, Patel G, Padbury R, et al. Colorectal cancer survival: An analysis of patients with metastatic disease synchronous and metachronous with the primary tumor. Clin Colorectal Cancer. 2014;13:87–93. doi: 10.1016/j.clcc.2013.11.008. [DOI] [PubMed] [Google Scholar]
- 9.Schule S, Dittmar Y, Knosel T, Krieg P, Albrecht R, Settmacher U, et al. Long-term results and prognostic factors after resection of hepatic and pulmonary metastases of colorectal cancer. Int J Colorectal Dis. 2013;28:537–545. doi: 10.1007/s00384-012-1553-0. [DOI] [PubMed] [Google Scholar]
- 10.Fong Y, Cohen AM, Fortner JG, Enker WE, Turnbull AD, Coit DG, et al. Liver resection for colorectal metastases. J Clin Oncol. 1997;15:938–946. doi: 10.1200/JCO.1997.15.3.938. [DOI] [PubMed] [Google Scholar]
- 11.Ueno H, Mochizuki H, Hatsuse K, Hase K, Yamamoto T. Indicators for treatment strategies of colorectal liver metastases. Ann Surg. 2000;231:59–66. doi: 10.1097/00000658-200001000-00009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Saito Y, Omiya H, Kohno K, Kobayashi T, Itoi K, Teramachi M, et al. Pulmonary metastasectomy for 165 patients with colorectal carcinoma: a prognostic assessment. J Thorac Cardiovasc Surg. 2002;124:1007–1013. doi: 10.1067/mtc.2002.125165. [DOI] [PubMed] [Google Scholar]
- 13.Girard P, Ducreux M, Baldeyrou P, Rougier P, Le Chevalier T, Bougaran J, et al. Surgery for lung metastases from colorectal cancer: analysis of prognostic factors. J Clin Oncol. 1996;14:2047–2053. doi: 10.1200/JCO.1996.14.7.2047. [DOI] [PubMed] [Google Scholar]
- 14.Jenkins LT, Millikan KW, Bines SD, Staren ED, Doolas A. Hepatic resection for metastatic colorectal cancer. Am Surg. 1997;63:605–610. [PubMed] [Google Scholar]
- 15.Scheele J, Stang R, Altendorf-Hofmann A, Paul M. Resection of colorectal liver metastases. World J Surg. 1995;19:59–71. doi: 10.1007/BF00316981. [DOI] [PubMed] [Google Scholar]
- 16.Choti MA, Sitzmann JV, Tiburi MF, Sumetchotimetha W, Rangsin R, Schulick RD, et al. Trends in long-term survival following liver resection for hepatic colorectal metastases. Ann Surg. 2002;235:759–766. doi: 10.1097/00000658-200206000-00002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Fong Y, Fortner J, Sun RL, Brennan MF, Blumgart LH. Clinical score for predicting recurrence after hepatic resection for metastatic colorectal cancer: analysis of 1001 consecutive cases. Ann Surg. 1999;230:309–318. doi: 10.1097/00000658-199909000-00004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Fernandez FG, Drebin JA, Linehan DC, Dehdashti F, Siegel BA, Strasberg SM. Fiveyear survival after resection of hepatic metastases from colorectal cancer in patients screened by positron emission tomography with F-18 fluorodeoxyglucose (FDG-PET) Ann Surg. 2004;240:438–447. doi: 10.1097/01.sla.0000138076.72547.b1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Yedibela S, Klein P, Feuchter K, Hoffmann M, Meyer T, Papadopoulos T, et al. Surgical management of pulmonary metastases from colorectal cancer in 153 patients. Ann Surg Oncol. 2006;13:1538–1544. doi: 10.1245/s10434-006-9100-2. [DOI] [PubMed] [Google Scholar]
- 20.Inoue M, Ohta M, Iuchi K, Matsumura A, Ideguchi K, Yasumitsu T, et al. Benefits of surgery for patients with pulmonary metastases from colorectal carcinoma. Ann Thorac Surg. 2004;78:238–244. doi: 10.1016/j.athoracsur.2004.02.017. [DOI] [PubMed] [Google Scholar]
- 21.Iwasaki A, Shirakusa T, Yamashita Y, Noritomi T, Maekawa T, Hamada T. Characteristic differences between patients who have undergone surgical treatment for lung metastasis or hepatic metastasis from colorectal cancer. Thorac Cardiovasc Surg. 2005;53:358–364. doi: 10.1055/s-2005-865758. [DOI] [PubMed] [Google Scholar]
- 22.Nuzzo G, Giuliante F, Ardito F, Vellone M, Giovannini I, Federico B, et al. Influence of surgical margin on type of recurrence after liver resection for colorectal metastases: a single-center experience. Surgery. 2008;143:384–393. doi: 10.1016/j.surg.2007.09.038. [DOI] [PubMed] [Google Scholar]
- 23.Pawlik TM, Scoggins CR, Zorzi D, Abdalla EK, Andres A, Eng C, et al. Effect of surgical margin status on survival and site of recurrence after hepatic resection for colorectal metastases. Ann Surg. 2005;241:715–722. doi: 10.1097/01.sla.0000160703.75808.7d. [DOI] [PMC free article] [PubMed] [Google Scholar]