

Abstract
Purpose:
To evaluate the efficacy of corneal collagen cross-linking (CXL) for treatment of corneal ulcers not responding to antimicrobial therapy.
Methods:
Eight patients with corneal ulcers associated with corneal melting, not responding to conventional antibiotic therapy, were treated with CXL. The procedure was performed according to the standardized protocol for keratoconus. Preoperative medications were continued after CXL in all cases. Microbiological exams revealed Pseudomonas aeruginosa in 3 cases. Follow up continued from 1 to 10 months.
Results:
In 6 of 8 eyes, progression of corneal melting was halted and complete epithelialization occurred. In one eye emergency keratoplasty was needed due to corneal perforation. A conjunctival flap was performed to treat severe localized corneal thinning in one of the patients a few days after CXL. Significant clinical improvement occurred in all cases of Pseudomonas aeruginosa keratitis.
Conclusion:
CXL can be considered as a promising new treatment in the management of refractory non-healing corneal ulcers, including Pseudomonas aeruginosa keratitis.
Keywords: Corneal Collagen Cross-linking, Corneal Ulcer, Riboflavin, Ultraviolet-A
INTRODUCTION
Infectious keratitis, often microbial in origin, is a devastating ocular disorder which can lead to blindness if not treated promptly. This urgent ophthalmic condition needs to be treated with appropriate antimicrobial agents.[1,2,3] However, some ulcers do not respond to conventional antimicrobial treatments.[4] Resistance of microbes to antibiotics is one of the main causes of treatment failure.[4,5,6] Furthermore, severe and refractory corneal ulcers are usually associated with corneal melting. As the enzymes that are released from inflammatory cells (neutrophils), some bacteria and fungi dissolve stromal collagen fibers and lead to corneal melting.[4,7,8]
Cross linking is a method of tissue stabilization.[9] Corneal collagen cross linking (CXL) was first introduced for corneal stiffening and stabilization of progressive keratoconous.[10] The procedure is performed using ultraviolet-A (UVA) irradiation and a photosensentizer (riboflavin, vitamin B2).[10,11]
There is also a known disinfecting effect for UVA light. Traditionally, it has been used for disinfection of drinking water and air/surface disinfection. This procedure has been used to inactivate viruses, bacteria and parasites from the time (1960s) Japanese scientists showed riboflavin exposed to visible or UV light could be used to inactivate the RNA containing tobacco mosaic virus.[12] Several in vitro and in vivo studies have shown that the use of riboflavin and UVA is effective against different pathogens.[13,14,15,16,17,18,19,20] In addition to this capability, cross-linking, using riboflavin and UVA, could stop collagenolysis and corneal melting in severe corneal ulceration.[21]
Herein, we report our experience with CXL for treatment of infectious keratitis resistant to conventional therapy in 8 patients.
METHODS
Eight patients with severe corneal ulcers were treated at the Department of Ophthalmology, Ahvaz Jundishapur University of Medical Sciences. Slit lamp biomicroscopy was performed to evaluate the ulcer details, anterior chamber condition and to measure ulcer size. Ultrasonography was performed to find any posterior segment pathology in cases with severe corneal haze. Samples were taken from the ulcer margins, conjunctiva, lid margins, contact lens and its cases in order to perform appropriate laboratory tests. Symptom duration before CXL was between 7-35 days. Three patients had history of previous ocular surgery. In one patient a therapeutic contact lens had been fitted because of an epithelial defect following DSAEK surgery. Patients’ details are presented in Table 1. Despite intensive topical and systemic antimicrobial therapy, corneal infiltration and melting progressed in all cases. Microbiological evaluation reports were negative in 2 of 8 eyes but positive for Pseudomonas aeruginosa in 3 eyes, and Enterobacter, Streptococcus and filamentary fungi each in one eye.
Table 1.
Demographic characteristics of patients with corneal ulcer treated with corneal collagen cross-linking
The conventional CXL protocol for keratoconous, as described by Wollensak et al, was used in all patients after obtaining informed consent. In one eye with severe localized thinning, conjunctival flap was performed shortly after CXL. Preoperative medications were continued after surgery in all cases. During the postoperative period, fortified antibiotics were tapered gradually and discontinued one week after complete re-epithelization. Cycloplegics, topical tear substitute drops, and systemic doxycycline were used in conjunction with antimicrobial drugs. All eyes were photographed prior to intervention and during each postoperative visit. Follow-up period ranged from 1 to 10 months.
CXL Procedure
CXL was performed under sterile conditions in the operating room. Tetracaine drops (0.1%) were used for topical anesthesia. After removal of the loose epithelium around the ulcer, riboflavin drops (Medio-Cross® riboflavin 0.1%/dextran solution 20%, Switzerland) were instilled every 3 min over the surface of cornea for 30 min. Thereafter, the cornea was irradiated for 30 min using a UVX lamp (Peschke Meditrade GmbH, Huenenberg, Switzerland), with 365 nm wavelength, irradiance of 3 mW/cm2 and distance of 5 cm. During the period of UVA irradiation, riboflavin was administered every 3-4 min.
Slit lamp microscopy, determination of visual acuity and slit lamp photography were performed at each postoperative follow up visit.
RESULTS
Eight patients with corneal ulcers associated with corneal melting not responding to intensive topical and systemic antimicrobial therapy were treated with CXL. The age of the patients ranged from 27 to 83 years.
All patients experienced improvement in symptoms, such as epiphora, photophobia and pain within 24-48 h after CXL. Hypopyon was present in 6 eyes but regressed completely within 2-4 days after treatment in all eyes except one. The progression of corneal melting stopped rapidly after CXL in six cases. Re-epithelialization of the cornea started within a few days and complete epithelialization was achieved with residual stromal scarring [Figures 1–3]. Wound healing was completed by 2-5 weeks. Best-corrected visual acuity ranged from light perception to counting fingers before CXL, which improved to hand motions to 20/100 during the postoperative period.
Figure 1.
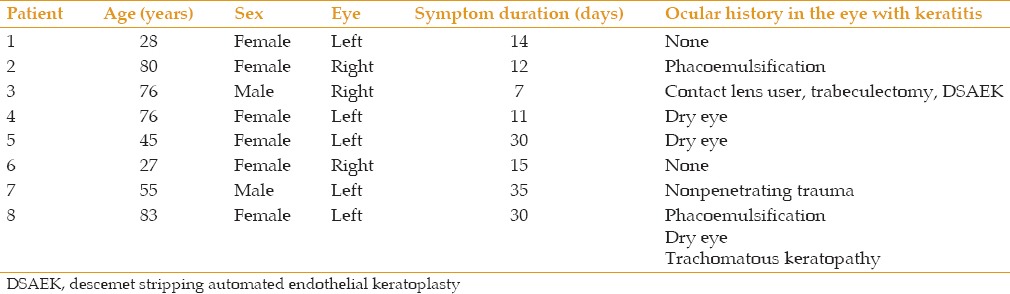
(a) Right eye of patient number 3, with a large Pseudomonas aeruginosa corneal ulcer at presentation, after 1-week medical treatment. (b) The same eye, 2 days after treatment with corneal collagen cross-linking (CXL) showing improvement with a significant decrease in infiltration density.
Figure 3.
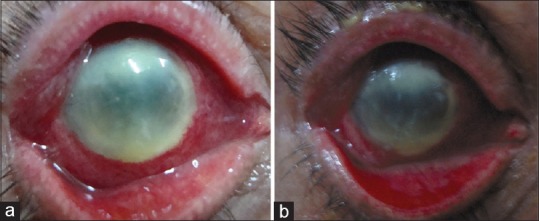
(a) Right eye of case number 6 with large corneal infiltration 15 days after topical antibiotic therapy. (b) The same eye 2 days after CXL showing a decrease in peripheral and central corneal infiltration. (c) The same eye 4 months after CXL showing a small corneal scar.
Figure 2.
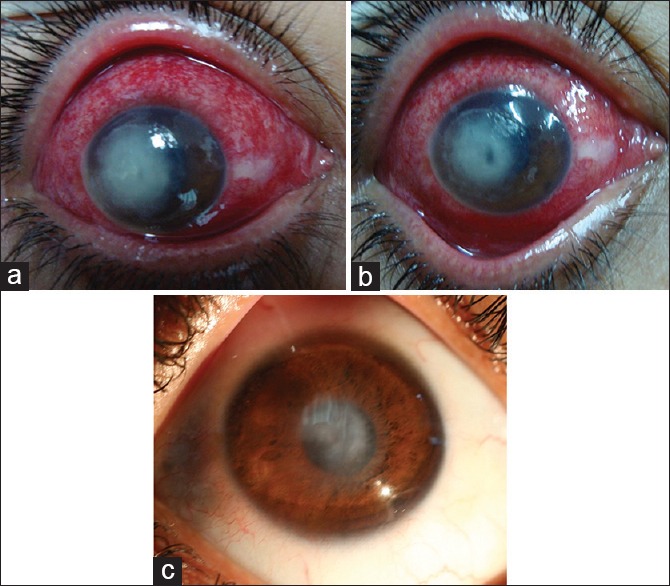
(a) Left eye of patient number 4, 11 days after medical treatment for Pseudomonas aeruginosa corneal ulcer. (b) The same eye shows significant healing with scar formation and corneal vascularization 4 weeks after CXL.
One eye developed corneal perforation 6 days after CXL. Therefore, urgent penetrating keratoplasty was performed. Table 2 presents more details on the cases.
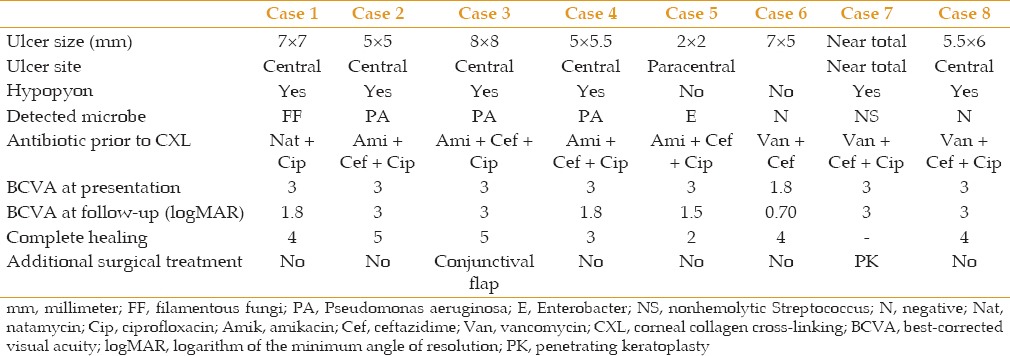
Table 2.
Ocular characteristics and outcomes of treatment with corneal collagen cross-linking in corneal ulcers
DISCUSSION
This series showed promising results from CXL for treating refractory infectious corneal ulcers associated with melting. Except one eye, all patients showed clinical improvement in ulcer characteristics and reported a decrease in pain and other symptoms. These results are compatible with other reports on the beneficial effect of CXL for refractory infectious keratitis.[13,14,15,16,17,18,19,22]
Collagen cross-linking is a new horizon in the treatment of corneal diseases. The corneal stroma is the thickest part of the cornea and is mainly composed of collagen fibrils, charged with stromal maintenance and wound healing.[23,24] Corneal collagen cross-linking by UVA and riboflavin creates more covalent bands between collagen fibers. It has a stiffening effect that stabilizes the corneal stroma and increases its resistance to enzymatic degradation.[24,25,26] Although, this procedure was originally introduced as a treatment for corneal ectasia,[10] there are increasing reports of its effectiveness in the treatment of a variety of other corneal disorders such as symptomatic Fuch's corneal dystrophy,[27] pseudophakic bullous keratopathy,[28] and more recently, infectious keratitis.[13,14,15,16,17,18,19]
Resistance to antibiotics, which happens because of chromosomal changes or the exchange of genetic material via plasmids or transposons, is a major cause of refractory non-healing corneal ulcers.[6] CXL seems to be a valuable adjunctive treatment in such cases because its mechanisms of action are different from antibiotics.
The therapeutic effect of CXL in corneal ulcers could be related to its toxic action against the pathogens and the increase in collagen resistance against enzymatic degradation. UV irradiation has antimicrobial activity and has been traditionally used for disinfection of blood transfusion products, drinking water and air or surfaces.
Hiraku et al demonstrated that UVA radiation (365 nm) in the presence of a photosensitizer such as riboflavin and pterin derivatives induces DNA damage.[29] After UVA absorption, the riboflavin molecules cross-over to a triplet state and transfer energy to generate singlet oxygen. Singlet oxygen and superoxide anions then react with available groups nearby.[29,30]
Martins et al studied the in vitro antimicrobial properties of riboflavin/UVA (365) against common pathogens including, Pseudomonas aeruginosa, Staphylococcus aureus and epidermidis, methicillin-resistant S. aureus (MRSA), multidrug-resistant P. aeruginosa (MDRPA), drug-resistant Streptococcus pneumoniae (DRSP), and Candida albicans (CA). They demonstrated that UVA/riboflavin was effective against all of them except Candida albicans.[20]
Among our eight patients, three cases had keratitis due to P. aeruginosa with large progressive corneal ulcers unresponsive to antibiotic therapy. All of these cases were controlled and treated successfully with CXL. Clinically, P. aeruginosa keratitis ulcers usually show severe corneal ulcerations with a rapidly progressive course and stromal necrosis. Treatment of P. aeruginosa keratitis is generally thought to be more difficult, with poorer visual outcomes than other bacterial corneal ulcers.[4,31] There are several reports that have described cases of infectious keratitis due to mycobacteria, S. aureus, S. epidermidis, Enterobacter, fungi, and Acanthameoba corneal infection successfully treated with CXL.[13,14,15,16,17,18,19,32] However, there are not enough reports on treating P. aeruginosa keratitis using CXL. In our small series, three eyes had refractory keratitis secondary to P. aeruginosa. According to this study, CXL may be an effective adjunctive therapy in controlling advanced refractory P. aeruginosa keratitis.
In addition to its antibacterial effect, several studies suggested that CXL could be effective to treat sterile keratitis.[21,33] Gao et al studied the effect of CXL on prevention of melting in rabbit corneas after alkali burn and found that it could prevent and delay corneal melting. They showed that CXL reduced the destruction of corneal collagen fibers and infiltration of inflammatory cells in the cornea.[21]
Ehlers et al performed CXL for treating corneal decompensation and non-healing corneal ulcers including sterile keratitis. They reported that CXL could be effective in some cases of sterile keratitis. One of the probable hypotheses explaining such an effect is that free oxygen radicals produced during CXL may directly inactivate proteolytic enzymes or damage leukocytes thus reducing the production of such enzymes.[34] Spoerl et al showed that CXL markedly increased corneal collagen resistance against enzymatic digestion by trypsin and pepsin.[26]
In another study by Wollensak et al, the authors found that CXL led to an increase in mechanical rigidity of the cornea, which was more prominent in human corneas as compared to porcine corneas.[24] Considering our study, melting was a prominent feature in all ulcers which stopped in 75% of cases after CXL. These findings are compatible with similar studies proposing a positive effect from CXL in treating stromal melting.[13,14,15,16,17,18,19]
The potency of CXL to halt progressive ulceration and melting in infectious keratitis could prevent the need to perform emergency penetrating keratoplasty. In the presence of active corneal infection and anterior chamber inflammation, penetrating keratoplasty is associated with higher rates of rejection and more post-keratoplasty complications such as anterior and posterior synechiae, glaucoma, cataracts, need for resuturing, stromal haze and graft infection.[34,35] In our study, only one case required penetrating keratoplasty because of corneal perforation. It seems that CXL could prevent such complications in severe corneal ulcerations.
In conclusion, CXL could be considered as a useful adjunct for treating progressive and non-healing corneal infections including P. aeruginosa keratitis. This intervention may decrease the need to perform emergency penetrating keratoplasty. However, more research on a larger number of eyes and more randomized clinical trials comparing the safety of CXL application to routine antibiotics are recommended.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Bennett HG, Hay J, Kirkness CM, Seal DV, Devonshire P. Antimicrobial management of presumed microbial keratitis: Guidelines for treatment of central and peripheral ulcers. Br J Ophthalmol. 1998;82:137–145. doi: 10.1136/bjo.82.2.137. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Jones DB. Decision-making in the management of microbial keratitis. Ophthalmology. 1981;88:814–820. doi: 10.1016/s0161-6420(81)34943-4. [DOI] [PubMed] [Google Scholar]
- 3.Gokhale NS. Medical management approach to infectious keratitis. Indian J Ophthalmol. 2008;56:215–220. doi: 10.4103/0301-4738.40360. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Edelstein SL, Wichiensin P, Huang AJ. Krachmer JH, Mannis MJ, Holland EJ. Cornea. Philadelphia: Mosby, Elsevier; 2011. Bacterial keratitis; pp. 919–944. [Google Scholar]
- 5.Levy SB. Multidrug resistance – A sign of the times. N Engl J Med. 1998;338:1376–1378. doi: 10.1056/NEJM199805073381909. [DOI] [PubMed] [Google Scholar]
- 6.Neu HC. The crisis in antibiotic resistance. Science. 1992;257:1064–1073. doi: 10.1126/science.257.5073.1064. [DOI] [PubMed] [Google Scholar]
- 7.Iakovleva MB, Kozel’tsev VL. Proteolysis of collagen by several species of micromycetes and spore-forming bacteria. Prikl Biokhim Mikrobiol. 1994;30:121–126. [PubMed] [Google Scholar]
- 8.Dong X, Shi W, Zeng Q, Xie L. Roles of adherence and matrix metalloproteinases in growth patterns of fungal pathogens in cornea. Curr Eye Res. 2005;30:613–620. doi: 10.1080/02713680590968196. [DOI] [PubMed] [Google Scholar]
- 9.Simmons DM, Kearney JN. Evaluation of collagen cross-linking techniques for the stabilization of tissue matrices. Biotechnol Appl Biochem. 1993;17(Pt 1):23–29. [PubMed] [Google Scholar]
- 10.Wollensak G, Spoerl E, Seiler T. Riboflavin/ultraviolet-a-induced collagen crosslinking for the treatment of keratoconus. Am J Ophthalmol. 2003;135:620–627. doi: 10.1016/s0002-9394(02)02220-1. [DOI] [PubMed] [Google Scholar]
- 11.Spoerl E, Huhle M, Seiler T. Induction of cross-links in corneal tissue. Exp Eye Res. 1998;66:97–103. doi: 10.1006/exer.1997.0410. [DOI] [PubMed] [Google Scholar]
- 12.Tsugita A, Okada Y, Uehara K. Photosensitized inactivation of ribonucleic acids in the presence of riboflavin. Biochim Biophys Acta. 1965;103:360–363. doi: 10.1016/0005-2787(65)90182-6. [DOI] [PubMed] [Google Scholar]
- 13.Makdoumi K, Mortensen J, Crafoord S. Infectious keratitis treated with corneal crosslinking. Cornea. 2010;29:1353–1358. doi: 10.1097/ICO.0b013e3181d2de91. [DOI] [PubMed] [Google Scholar]
- 14.Iseli HP, Thiel MA, Hafezi F, Kampmeier J, Seiler T. Ultraviolet A/riboflavin corneal cross-linking for infectious keratitis associated with corneal melts. Cornea. 2008;27:590–594. doi: 10.1097/ICO.0b013e318169d698. [DOI] [PubMed] [Google Scholar]
- 15.Panda A, Krishna SN, Kumar S. Photo-activated riboflavin therapy of refractory corneal ulcers. Cornea. 2012;31:1210–1213. doi: 10.1097/ICO.0b013e31823f8f48. [DOI] [PubMed] [Google Scholar]
- 16.Price MO, Tenkman LR, Schrier A, Fairchild KM, Trokel SL, Price FW., Jr Photoactivated riboflavin treatment of infectious keratitis using collagen cross-linking technology. J Refract Surg. 2012;28:706–713. doi: 10.3928/1081597X-20120921-06. [DOI] [PubMed] [Google Scholar]
- 17.Micelli Ferrari T, Leozappa M, Lorusso M, Epifani E, Micelli Ferrari L. Escherichia coli keratitis treated with ultraviolet A/riboflavin corneal cross-linking: A case report. Eur J Ophthalmol. 2009;19:295–297. doi: 10.1177/112067210901900221. [DOI] [PubMed] [Google Scholar]
- 18.Khan YA, Kashiwabuchi RT, Martins SA, Castro-Combs JM, Kalyani S, Stanley P, et al. Riboflavin and ultraviolet light a therapy as an adjuvant treatment for medically refractive Acanthamoeba keratitis: Report of 3 cases. Ophthalmology. 2011;118:324–331. doi: 10.1016/j.ophtha.2010.06.041. [DOI] [PubMed] [Google Scholar]
- 19.Sorkhabi R, Sedgipoor M, Mahdavifard A. Collagen cross-linking for resistant corneal ulcer. Int Ophthalmol. 2013;33:61–66. doi: 10.1007/s10792-012-9633-2. [DOI] [PubMed] [Google Scholar]
- 20.Martins SA, Combs JC, Noguera G, Camacho W, Wittmann P, Walther R, et al. Antimicrobial efficacy of riboflavin/UVA combination (365 nm) in vitro for bacterial and fungal isolates: A potential new treatment for infectious keratitis. Invest Ophthalmol Vis Sci. 2008;49:3402–3408. doi: 10.1167/iovs.07-1592. [DOI] [PubMed] [Google Scholar]
- 21.Gao XW, Zhao XD, Li WJ, Zhou X, Liu Y. Experimental study on the treatment of rabbit corneal melting after alkali burn with Collagen cross-linking. Int J Ophthalmol. 2012;5:147–150. doi: 10.3980/j.issn.2222-3959.2012.02.06. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Morén H, Malmsjö M, Mortensen J, Ohrström A. Riboflavin and ultraviolet a collagen crosslinking of the cornea for the treatment of keratitis. Cornea. 2010;29:102–104. doi: 10.1097/ICO.0b013e31819c4e43. [DOI] [PubMed] [Google Scholar]
- 23.Dawson DG, Watsky MA, Geroski DH, Edelhauser HF. Cornea and sclera. In: Tasman W, Jaeger EA, editors. Duanés Ophthalmology. Hagerstown, MD: Lippincott Williams and Wilkins; 2007. [Google Scholar]
- 24.Wollensak G, Spoerl E, Seiler T. Stress-strain measurements of human and porcine corneas after riboflavin-ultraviolet-A-induced cross-linking. J Cataract Refract Surg. 2003;29:1780–1785. doi: 10.1016/s0886-3350(03)00407-3. [DOI] [PubMed] [Google Scholar]
- 25.Hafezi F. Cross-linking of corneal collagen with UVA and riboflavin for the treatment of corneal disease. Iran J Ophthalmol. 2009;21:3–12. [Google Scholar]
- 26.Spoerl E, Wollensak G, Seiler T. Increased resistance of crosslinked cornea against enzymatic digestion. Curr Eye Res. 2004;29:35–40. doi: 10.1080/02713680490513182. [DOI] [PubMed] [Google Scholar]
- 27.Hafezi F, Dejica P, Majo F. Modified corneal collagen crosslinking reduces corneal oedema and diurnal visual fluctuations in Fuchs dystrophy. Br J Ophthalmol. 2010;94:660–661. doi: 10.1136/bjo.2009.162479. [DOI] [PubMed] [Google Scholar]
- 28.Ghanem RC, Santhiago MR, Berti TB, Thomaz S, Netto MV. Collagen crosslinking with riboflavin and ultraviolet-A in eyes with pseudophakic bullous keratopathy. J Cataract Refract Surg. 2010;36:273–276. doi: 10.1016/j.jcrs.2009.07.041. [DOI] [PubMed] [Google Scholar]
- 29.Hiraku Y, Ito K, Hirakawa K, Kawanishi S. Photosensitized DNA damage and its protection via a novel mechanism. Photochem Photobiol. 2007;83:205–212. doi: 10.1562/2006-03-09-IR-840. [DOI] [PubMed] [Google Scholar]
- 30.Baier J, Maisch T, Maier M, Engel E, Landthaler M, Bäumler W. Singlet oxygen generation by UVA light exposure of endogenous photosensitizers. Biophys J. 2006;91:1452–1459. doi: 10.1529/biophysj.106.082388. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Sy A, Srinivasan M, Mascarenhas J, Lalitha P, Rajaraman R, Ravindran M, et al. Pseudomonas aeruginosa keratitis: Outcomes and response to corticosteroid treatment. Invest Ophthalmol Vis Sci. 2012;53:267–272. doi: 10.1167/iovs.11-7840. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Sauer A, Letscher-Bru V, Speeg-Schatz C, Touboul D, Colin J, Candolfi E, et al. In vitro efficacy of antifungal treatment using riboflavin/UV-A (365 nm) combination and amphotericin B. Invest Ophthalmol Vis Sci. 2010;51:3950–3953. doi: 10.1167/iovs.09-4013. [DOI] [PubMed] [Google Scholar]
- 33.Ehlers N, Hjortdal J, Nielsen K, Søndergaard A. Riboflavin-UVA treatment in the management of edema and nonhealing ulcers of the cornea. J Refract Surg. 2009;25:S803–806. doi: 10.3928/1081597X-20090813-08. [DOI] [PubMed] [Google Scholar]
- 34.Xie L, Zhai H, Shi W. Penetrating keratoplasty for corneal perforations in fungal keratitis. Cornea. 2007;26:158–162. doi: 10.1097/01.ico.0000248381.24519.0d. [DOI] [PubMed] [Google Scholar]
- 35.Garg P, Rao GN. Theraputic penetrating keratoplasty. In: Brightbill FS, editor. Corneal Surgery: Theory, Technique and Tissue. 4th ed. St.Louis, Missouri: Elsevier, Mosby; 2009. pp. 439–449. [Google Scholar]