

Abstract
We describe an innovative technique for performing standardized low cost glaucoma filtration surgery using a polytetrafluoroethylene (PTFE) intravenous cannula. The trocar of a 24 gauge (24G) PTFE intravenous cannula was used to create a trabeculectomy ostium and its tube was inserted under a partial thickness scleral flap in 2 patients with advanced glaucomatous optic neuropathy, in whom intraocular pressure (IOP) was not controlled on maximal tolerable hypotensive therapy. Postoperatively, IOP of the operated eyes at 3, 6 and 9 months’ follow-up ranged from 12 to 15 mmHg with a well formed anterior chamber and a diffuse bleb.
Keywords: Cost Effective, ExPress Shunt, Glaucoma Drainage Devices, Intravenous Cannula, Polytetrafluoroethylene, Toxicity, Trabeculectomy
INTRODUCTION
Trabeculectomy remains the surgery of choice in patients with advanced glaucomatous optic neuropathy (GON).[1] In conventional trabeculectomy, a sclerostomy and an iridectomy are mandatory.[2] Efforts have been made to improve the outcomes and reduce the complications of trabeculectomy. In this regard, the Ex-PRESS™ glaucoma implant was introduced as a nonvalved miniature stainless steel device, designed with the intent of offering a simple and safe alternative to classic trabeculectomy, obviating the need for tissue excision or removal. ExPress is easier than but not superior to trabeculectomy;[3] the problem is, that it is a very expensive alternative which the majority of patients in developing countries cannot afford. Therefore, we tried to use a low cost alternative which is universally available and can function as an alternative to classic trabeculectomy without the need for tissue excision or removal.
Herein, we describe an innovative, simple and cost effective technique using a 24 gauge (24G) polytetrafluoroethylene PTFE) intravenous cannula (IVC) as an alternative to the classic trabeculectomy.
Two pseudophakic patients with primary open angle glaucoma and advanced GON were operated. The first patient was a 50-year-old man with intraocular pressure (IOP) of 16 mmHg and 32 mmHg on maximal tolerable medical therapy in his right and left eyes, respectively. Best corrected visual acuity (BCVA) was 20/20 and light perception in his right and left eyes. The second patient was a 72-year-old male subject with IOP of 12 mmHg and 38 mmHg on four topical ocular hypotensive medications, in his right and left eyes, repectively. BCVA of the second patient was 20/20 and no light perception in the right and left eyes, respectively.
Both patients underwent glaucoma filtering surgery using a 24G intravenous cannula (IVC) together with application of 0.1 mg/ml Mitomycin-C subconjunctivally for 3 min under peri-bulbar anaesthesia. We specifically selected these end-stage patients due to unknown long-term results and complications of the surgery.
SURGICAL TECHNIQUE
An 8-0 polyglactin (Vicryl) traction suture on a spatulated needle was placed through the superficial cornea near the superior limbus. Consequently, a standard fornix-based conjunctival incision was made to gain exposure to the scleral bed adjacent to the limbus. Gentle cautery was performed in this area. A limbus-based rectangular scleral flap (4 mm × 4 mm) of about half scleral thickness was dissected. Care was taken to dissect the flap into the clear cornea. Mitomycin-C (MMC) 0.1 mg/ml soaked pledgets were applied subconjunctivally for 3 min after coating the cornea with viscoelastic. A rectangle of deep sclera (deep scleral groove) measuring 1 mm × 4 mm was made perpendicular to the limbus, leaving a thin layer of deep sclera covering the choroids [Figure 1]. A 24G IVC with an internal diameter of 0.7 mm (BD Neoflon™ IV Cannula, Becton Dickinson, Helsingborg, Sweden) with bevel of the trocar facing up, was inserted into the anterior chamber (AC) at the limbal end of the deep scleral groove and at the center of the “blue line,” parallel to the iris plane and directed towards the pupil [Figure 2]. The trocar was completely withdrawn when the cannula was 1 mm inside the AC and the PTFE cannula was cut 4 mm from the site of insertion. The tube was then secured in the preformed deep scleral groove using 10-0 nylon sutures [Figure 3]. The function of the tube was ensured by noting the dilution of trypan blue dye applied over the cut end of the cannula. The scleral flap was sutured using four 10-0 nylon sutures and the conjunctiva was repaired meticulously with 8-0 polyglactin sutures. Postoperative management was similar to a routine trabeculectomy.
Figure 1.
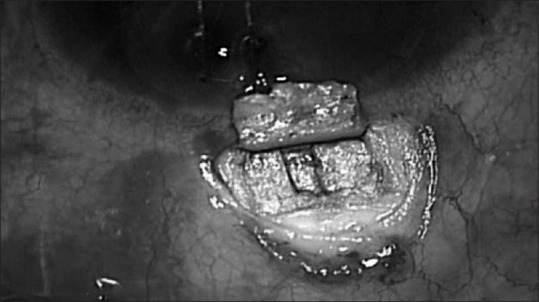
Intraoperative photograph showing the deep scleral groove, measuring 1 mm × 4 mm.
Figure 2.
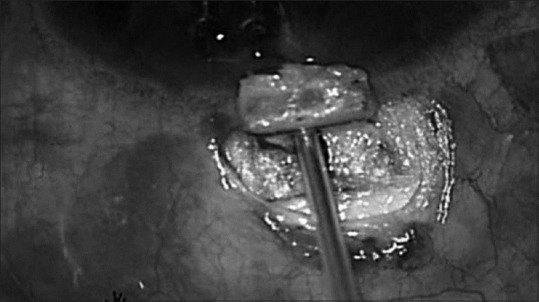
Intra-operative photograph showing the 24G cannula inserted into the anterior chamber (AC) through the centre of the “blue line” at an angle parallel to the iris plane and directed towards the pupil.
Figure 3.
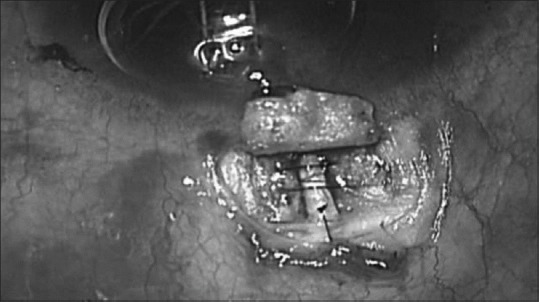
Intra-operative photograph showing the 24G cannula placed in the preformed deep scleral groove, secured to the scleral bed using 10-0 nylon sutures.
RESULTS
Postoperatively, IOP of the first patient at 3, 6 and 9 months ranged from 12 mmHg to 15 mmHg with a well formed anterior chamber and a functioning diffuse bleb. Gonioscopy and anterior segment OCT showed the presence of the tube [Figure 4]. IOP of the second patient at 6 weeks and 3 months ranged from 12 to 14 mmHg.
Figure 4.
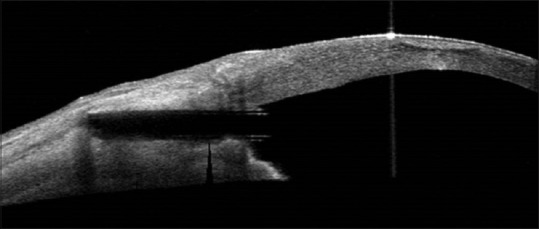
Anterior segment OCT at 9 months follow-up, showing the presence of the tube (24G cannula) in situ.
DISCUSSION
Trabeculectomy remains the surgery of choice in patients with advanced glaucomatous damage.[1] However, some of the problems associated with trabeculectomy are attributed to the need for tissue excision and lack of standardization of filtration.[4,5] New drainage devices such as the ExPRESS shunt are being used in an attempt to standardize the technique.[6] The restricted internal diameter of these devices provides certain consistency and standardization of the filtration procedure and flow regulation is largely governed by the sutures applied to close the scleral flap. Tissue excision or removal is not required, thereby reducing inflammation and complications associated with trabeculectomy. These modifications provide the option of a minimally invasive surgery.[6,3]
The major disadvantage of these devices is the added cost of surgery, especially in developing countries like ours. Therefore, we present the use of an inexpensive and widely available 24G intravenous cannula made of PTFE which is known to entail no toxicity in humans to date. The cannula functions by diverting aqueous humor through the implant from the AC to the intrascleral and subconjunctival spaces, similar to the ExPRESS device, and offers the advantages of standardization of filtration without the need for any tissue excision, unlike in trabeculectomy where a sclerostomy and an iridectomy are mandatory.
Our technique is a simple modification of conventional trabeculectomy aimed at making the surgery simpler and reducing immediate postoperative complications by using a small ostium without any need for iridectomy. We have introduced a low cost innovation which will help standardize surgery, make it easier and also decrease its learning curve; this procedure also avoids the need for a sclerostomy or iridectomy thereby minimizing tissue injury.
In summary, the use of a 24G intravenous cannula is a cost effective and simple alternative to glaucoma drainage devices in developing countries like ours, alongwith decreased learning curve of the procedure. We recommend further studies to evaluate the long-term safety and efficacy of this technique.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Ramulu PY, Corcoran KJ, Corcoran SL, Robin AL. Utilization of various glaucoma surgeries and procedures in Medicare beneficiaries from 1995 to 2004. Ophthalmology. 2007;114:2265–2270. doi: 10.1016/j.ophtha.2007.02.005. [DOI] [PubMed] [Google Scholar]
- 2.Salim S. Ex-PRESS glaucoma filtration device-surgical technique and outcomes. Int Ophthalmol Clin. 2011;51:83–94. doi: 10.1097/IIO.0b013e31821e5b82. [DOI] [PubMed] [Google Scholar]
- 3.de Jong L, Lafuma A, Aguadé AS, Berdeaux G. Five-year extension of a clinical trial comparing the EX-PRESS glaucoma filtration device and trabeculectomy in primary open-angle glaucoma. Clin Ophthalmol. 2011;5:527–533. doi: 10.2147/OPTH.S18565. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Watson PG, Jakeman C, Ozturk M, Barnett MF, Barnett F, Khaw KT. Complications of Trabeculectomy (20yrs follow-up) Eye. 1990;4:425–38. doi: 10.1038/eye.1990.54. [DOI] [PubMed] [Google Scholar]
- 5.Gedde SJ, Singh K, Schiffman JC, Feuer WJ. Tube Versus Trabeculectomy Study Group. The Tube Versus Trabeculectomy Study: Interpretation of results and application to clinical practice. Curr Opin Ophthalmol. 2012;23:118–126. doi: 10.1097/ICU.0b013e32834ff2d1. [DOI] [PubMed] [Google Scholar]
- 6.Wamsley S, Moster MR, Rai S, Alvim H, Fontanarosa J, Steinmann WC. Optonol ExPRESS miniature tube shunt in advanced glaucoma. Invest Ophthalmol Vis Sci. 2004;45:994A. [Google Scholar]