

Abstract
Endometriosis is a benign gynecological disease that is characterized by the presence of functional endometrial tissue outside the uterus. Although the ovaries and uterine ligaments are the most common locations, urinary tract involvement especially the bladder endometriosis is a rare entity in women of reproductive age with clinical symptoms of cyclical urgency, hematuria and suprapubic pain. We herein present magnetic resonance imaging (MRI) findings of spontaneous bladder endometriosis case with cyclical hematuria symptoms.
Keywords: Magnetic resonance imaging (MRI), endometriosis, bladder
Endometriosis is a benign gynecological disease that is characterized by the presence of functional endometrial tissue outside the uterus. Although the ovaries, uterine ligaments, fallopian tubes, rectum and cervico-vaginal regions are the most common locations involvement of the urinary tract is very rare (1-2%) (1). Amongst urinary tract endometriosis, the bladder is the most frequently involved with the incidence of 84%, however, it is 15-20% for the ureter. Endometriosis usually occurs in women of reproductive age because of the necessity of estrogen peak for endometrial proliferation (2). The pathogenesis of endometriosis has not been clarified however three theories are suggested to explain this condition; metaplastic, embryologic and migratory theories (3). Bladder endometriosis is mostly considered to occur, in consequence of migratory theory, as transporting endometrial tissue to an ectopic focus through the fallopian tubes during menstruation (3,4). However Donnez et al. reported that bladder endometriosis was an adenomyotic nodule similar to a rectovaginal adenomyotic nodule and usually associated with it (4).
A 29-year-old woman applied to the urology clinic with the complaints of cyclical hematuria attacks. After revealing an ovarian cystic mass at the abdominal ultrasonography, she was examined by the pelvic magnetic resonance imaging (MRI). There was a left adnexial cystic mass which was hyperintense on T1 weighted (W) and iso-hypointense on T2W images suggesting endometrioma (Figure 1A,B). Additionally a soft tissue at the bladder wall which was isointense on T1W and hypointense on T2W images compared to the adjacent muscles was noticed. It had milimetric hyperintense focuses on both T1W and T2W images which showed no contrast enhancement on the MRI (Figure 2A,B). With these findings radiologic impression of the mass was bladder anterior wall endometriosis. Transurethral biopsy was performed and finally endometrial tissue was observed in the pathologic specimen which verified the radiological impression.
Figure 1.
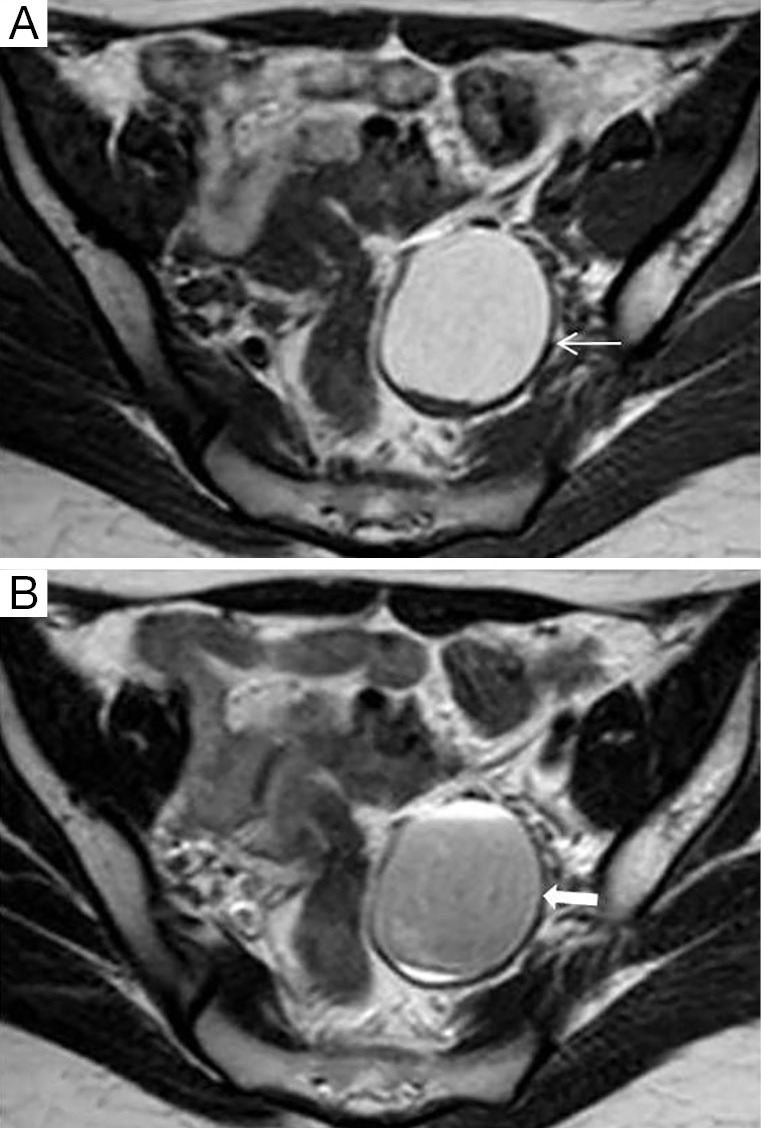
Axial MR images show a left adnexial endometrioma which is hyperintense on T1 weighted (W) (A) and iso-hypointense on T2W (B) (arrow).
Figure 2.

Axial T1W (A) and sagittal T2W (B) MR images demonstrate bladder wall soft tissue mass with milimetric hyperintense focuses and (arrow). W, weighted.
Endometriosis mostly presents within the ovaries and uterine ligaments which is commonly known as chocolate cyst (endometrioma) because of the recurrent internal hemorrhage. The symptoms of the bladder endometriosis are cyclical urgency, hematuria and suprapubic pain. Cyclical menstrual hematuria is pathognomonic for bladder endometriosis however it is present in only 20% of patients (2,5).
The characteristic imaging criterias for endometriomas are T1W hyperintensity and T2W hypointensity (shading) on MRI. Hypointensity on T2W MRI is defined for the ovarian endometriosis as the shading sign which is due to high levels of protein and iron concentration (6). The ovarian cyst in our case had T2W hypointensity and T1W hyperintensity with characteristic endometrioma imaging findings. The bladder lesion had similar imaging findings with the left ovarian endometrioma. As a result, the lesion was diagnosed as bladder endometriosis with her clinical symptoms and MRI examination findings.
Vesical endometriosis can occur spontaneously or iatrogenically (postoperatively) whereas bladder wall limited involvement is usually described as a result of iatrogenic form (5). Our case did not have surgical history so it was presumed to be the spontaneous form.
Bladder endometriosis is a rare entity in women of reproductive age with cyclical hematuria symptoms. The knowledge and recognition of the rare location of endometriosis can be helpful to diagnose the pathology by MRI examination which is the optimal imaging modality.
Acknowledgments
Disclosure: The authors declare no conflict of interest.
References
- 1.Westney OL, Amundsen CL, McGuire EJ. Bladder endometriosis: conservative management. J Urol 2000;163:1814-7. [DOI] [PubMed] [Google Scholar]
- 2.Kumar S, Tiwari P, Sharma P, Goel A, Singh JP, Vijay MK, et al. Urinary tract endometriosis: Review of 19 cases. Urol Ann 2012;4:6-12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Rıdley JH. The validity of Sampson’s theory of endometriosis. Am J Obstet Gynecol 1961;82:777-82. [DOI] [PubMed] [Google Scholar]
- 4.Donnez J, Spada F, Squifflet J, Nisolle M.Bladder endometriosis must be considered as bladder adenomyosis. Fertil Steril 2000;74:1175-81. [DOI] [PubMed] [Google Scholar]
- 5.Mettler L, Gaikwad V, Riebe B, Schollmeyer T.Bladder endometriosis: possibility of treatment by laparoscopy. JSLS 2008;12:162-5. [PMC free article] [PubMed] [Google Scholar]
- 6.Glastonbury CM. The shading sign. Radiology 2002;224:199-201. [DOI] [PubMed] [Google Scholar]