

Abstract
Background:
Dental problems in the preschool children are neglected by their parents as the deciduous teeth are going to shed off, and hence considered to be of no importance and more of economic burden if attended to them.
Aims:
This study was to determine the caries prevalence in preschool children (3-5-year-old) of rural Moradabad district, to analyze the specific pattern of dental caries experience in this population and to assess the treatment needs among them.
Material and Methods:
Children within the age group of 3-5 years attending Anganwadi centers of rural Moradabad district were included in the study. Caries diagnosis was based on decayed, extracted, filled surface (defs) and the treatment needs were recorded using World Health Organization (WHO) oral health assessment form 1997.
Results:
Out of 1,500 children examined, 48.7% males and 52.6% females did not require any treatment. The mean decayed, extracted, filled teeth (deft) value was found to be significantly high in 5-year-old participants when compared to 3-year-old participants (P < 0.01). Majority of the children required one surface filling followed by two surface fillings, caries arresting sealant care, extraction, crown bridge element, pulp care, and space maintainer.
Conclusion:
The most common pattern was pit and fissure, then maxillary anterior pattern, posterior proximal pattern, and posterior buccal lingual smooth surface pattern. The mean deft value was higher in males as compared to females. There is a greater need for oral health education among parents and teachers.
Keywords: Dental caries, preschool children, treatment needs, rural India, Uttrakhand
Introduction
Health is a common theme in most cultures. With the adoption of health as an integral part of socioeconomic development by the United Nations, it has become a major instrument of overall socioeconomic development and the creation of a new social order.[1] Poor oral health has a detrimental effect on children's performance in school and their success in later life.[2]
The two most common oral diseases are dental caries and periodontal disease.[2] There is no universally accepted opinion of the etiology of dental caries and is considered multifactorial in nature.[3]
Due to its high global prevalence; dental caries among children has been described as a ‘pandemic’ disease.[4,5,6] The World Health Organization (WHO) has ranked it as number three among all chronic noncommunicable diseases that require worldwide attention for prevention and treatment.[5] It is the most prevalent unmet healthcare need of children. Decayed teeth are harmful to children's growth and development and can severely jeopardize their health.[7,8]
Voluminous dental literatures exist about caries levels in the urban Indian population, but there is scarcity of any such literature for rural parts of India which indeed requires more attention.[9] The distribution and severity of dental caries vary in different parts of the world and within the same country or region. The overall impression is that dental caries has increased in prevalence and severity in the urban and cosmopolitan population over the last couple of decades.[6] However, there is no picture yet regarding the dental caries status in the rural areas of India, where 72.2% of the population live.[10,11] Although dental caries is known to be a significant problem in preschool populations, comprehensive understanding of its epidemiology is limited due to the difficulty in accessing this age group for data collection purposes. No data are available on caries prevalence or the treatment needs of caries lesions for preschool children under 3-5 years of age in rural Moradabad district; so the present study aims to evaluate the prevalence of dental caries and to estimate the treatment needs in 3-5-year-old preschool children in rural Moradabad district by using WHO dentition status and treatment need index.
Materials and Methods
An epidemiological survey was conducted to assess the prevalence of dental caries and treatment needs among 3-5-year-old preschool children of rural Moradabad district. Permission to conduct the survey in the selected Anganwadi was obtained from the respective authorities. Informed consent was obtained from the Mukhya Sevika of the Anganwadi centers (courtyard in which rural children are provided preschool education) of the respective Anganwadis. This study was reviewed and cleared by the Ethics Committee of Teerthanker Mahaveer Dental College and Research Centre, Moradabad.
There was no prevalence data for caries and treatment needs among preschool children in the region. Hence, a pilot study was conducted among 200 preschool children. The sample size was calculated on the basis of the results acquired from the pilot study. Based on the results of pilot study, the sample size was estimated to be 1,478; but the sample size was chosen as 1,500; this is to account for dropouts or refusal.
Formula for Sample Size Calculation
N = Z2 pq/d2
Where
N = Sample size, Z = point of normal distribution (as per table of area under normal curve for the given confidence level of 95%) = 1.96, P = proportion or prevalence of interest = 19%, q = 100 - P (alternative prevalence), and d = clinically acceptable error = 2%.
Applying the formula for this study
N = 1.96 × 1.96 (19 (100 - 19))/2 × 2 = 1,478
Before starting the evaluation; the examiner was calibrated at Department of Public Health Dentistry, Teerthanker Mahaveer Dental College and Research Centre in order to limit the intraexaminer variability. In order to test the intraexaminer variability, aged-matched samples of 30 children were examined under identical conditions on two occasions, at least a week apart. The agreement for all the assessments was in the range of 85-95% (kappa statistics). These values reflected high degree of conformity in observations. A list of all the Anganwadi centers and the list of children were obtained from the Child Development Project Officer (CDPO), situated in the rural Moradabad district; from this sampling frame 1,500 children were chosen by the simple random sampling technique.
The survey includes caries data among 3-5-year-old preschool children and clinical data encompassing caries and treatment needs. Modified WHO proforma 1997 was used to record the clinical data.
Clinical examination
A type III (using mouth mirror and explorer with proper illumination) examination was carried out under adequate illumination using plane mouth mirror and metallic periodontal probes (community periodontal index (CPI) probe). Clinical conditions recorded were caries in primary dentition of 3-5-year-old by decayed, extracted, filled teeth (deft)/decayed, extracted, filled surfaces (defs) and treatment needs were also assessed.
Deft/defs indices were used to assess the caries status of primary dentition of 3-5-year-old preschool children of rural Moradabad district. deft/defs express the caries burden in deciduous teeth and are obtained by calculating the number of teeth decayed (d), missing/extracted due to caries (e); and filled (f) teeth (t) or surfaces (s), are used for the primary dentition. It is thus used to get an estimation illustrating how much the primary dentition until the day of examination has become affected by dental caries.
Treatment needs: Treatment needs were assessed by Modified WHO proforma 1997.
Participants were made to sit on a chair in a well-ventilated room or in field such that the examination was carried out under natural lighting conditions or in the torch light and the examiner stood behind the subject. The oral conditions were recorded in the boxes provided in the proforma by the recorder, as the examiner said them out loud. Artificial illumination was used at times when required. The recorder was made to sit close to the examiner in front of the subject so that instructions and codes could be easily heard and the examiner could see that the findings were being recorded correctly. This also enabled the recorder to check that the score recorded was related to the region or tooth that had just been examined. The examination was arranged in such a way that children came one at a time without crowding the examiner. The Aganwadi workers also helped the investigator in maintaining this decorum.
Statistical analysis
Data were analyzed by the Statistical Package for Social Sciences (SPSS) version 21 with Student's t-test and analysis of variance at a 0.05 significance level and 95% confidence interval.
Results
Descriptive data analysis
Sample comprised of total 1,500 children (802 males and 698 females); 355 children in the 3-year age group consisted of 178 males and 177 females; 577 children in the 4-year age group comprised of 334 and 243 males and females, respectively; and 290 males and 278 females were included in 5-year age group having total of 568 children.
Caries prevalence in preschool children
Of the total 1,500 children examined, 824 (54.9%) children were caries free and 676 (45.1%) were with caries.
Distribution of study population by age, sex, number of participants with dental caries, and the number of dental caries-free participants
Dental caries prevalence was lowest among 3-year-olds (37.3%) and was same for both 4- and 5-year-old children (47.3%). Among all the participants screened, prevalence of dental caries among boys (46.5%) was higher than the girls (41.7).
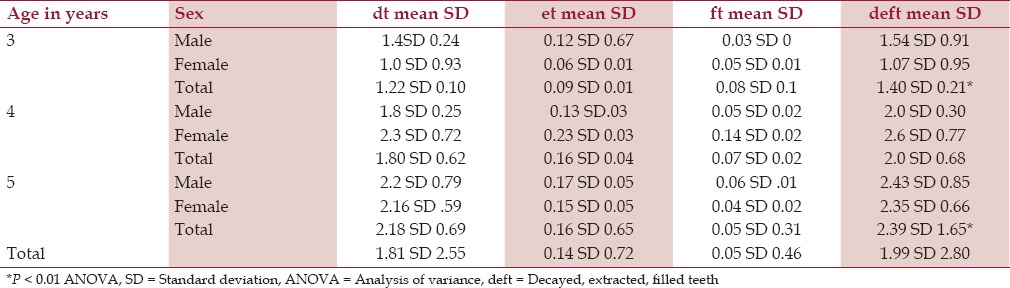
The mean deft values for 3-, 4-, and 5-year-old participants
In the age group of 3 years, the mean deft was 1.54 standard deviation (SD) 0.91 and 1.07 SD 0.95 among males and females, respectively. In the age group of 4 years, the mean deft was 2.0 SD 0.3 and 2.6 SD 1.84 among males and females, respectively. In the age group of 5 years, the mean deft was 2.43 SD 0.85 and 2.35 SD 0.66 among males and females, respectively.
Among all the age groups, 3-year-old children showed less mean deft (1.40 SD 0.21) as compared to 4 years (2.0 SD 0.68) and 5 years (2.39 SD 1.65). The mean deft values were found to be significantly high in 5-year-old participants when compared to 3-year-olds (P < 0.01).
In the age group of 3 years; 180 (50.7%), 150 (42.2%), and 25 (7.1%) children had decayed, extracted, and filled teeth, respectively. A total of 259 (44.8%), 189 (32.7%), and 129 (22.3%) children of 4-year-old group had decayed, extracted, and filled teeth, respectively. In 5-year-old group; 270 (47.5%), 199 (35%), and 99 (17.4%) children had decayed, extracted, and filled teeth, respectively [Table 1].
Table 1.
Mean deft value for 3-, 4-, and 5-year-old participants
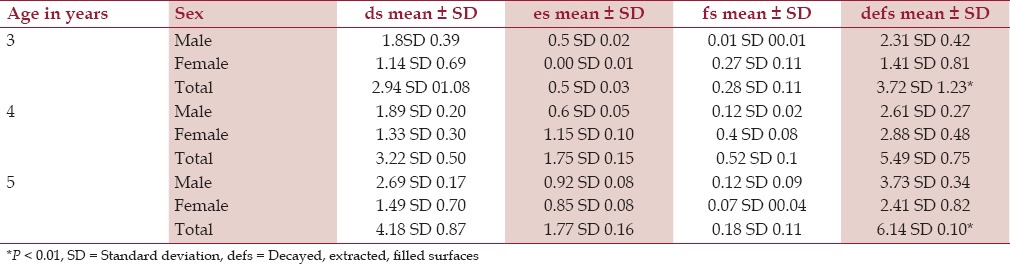
The mean defs values for 3-, 4-, and 5-year-old participants
In the age group of 3 years, the mean defs was 2.4 SD 0.42 and 1.41 SD 0.81 among males and females, respectively. In the age group of 4 years, the mean defs was 3.0 SD 0.27 and 4.37 SD 0.48 among males and females, respectively. In the age group of 5 years, the mean defs was 3.73 SD 0.34 and 3.41 SD 0.82 among males and females, respectively. The mean defs values were found to be significantly high in 5-year-old participants when compared to 3-year-old subjects (P < 0.01) [Table 2].
Table 2.
Mean defs value for 3-, 4-, and 5-year-old participants
Number and percentage distribution of participants by individual caries pattern
Among 1,500 participants; 824 (55%) were caries free. Of the total children who had caries, 491 (72.6%) had pit and fissure pattern, 301 (44.5%) had maxillary anterior pattern, 303 (44.8%) had posterior proximal, and 115 (17%) had buccal/lingual smooth surface pattern.
Distribution of the participants by dental caries pattern, age group, and gender
In the 3-year-old 178 (11.89%) male participants; 101(56.7%) participants were caries free, 61 (34.3%) had pit and fissure caries, 37(20.8%) had maxillary anterior pattern, 33(18.5%) had posterior proximal caries, and 14 (7.9%) has posterior buccal lingual smooth surface caries. In 3-year-old 177 (11.8%) female participants; 120 (67.8%) were caries free, 43 (24.3%) had pit and fissure caries, 22 (12.4%) had maxillary anterior pattern, 15 (8.5%) had posterior proximal pattern, and 10 (5.6%) had posterior buccal/lingual smooth surface pattern.
In the 4-year-old 334 (22.3%) males; 176 (52.7%) were caries free, 124 (37.1%) had pit and fissure pattern, 75 (22.4%) had maxillary anterior pattern, 73 (21.8%) had posterior proximal pattern, and 23 (6.9%) had posterior buccal/lingual smooth surface pattern. Among 243 (16.2%) 4-year-old females; 128 (52.7%) were caries free, 71 (29.2%) had pit and fissure pattern, 51 (21.0%) had maxillary anterior pattern, 44 (18.1%) had posterior proximal pattern, and 22 (9.0%) had posterior buccal/lingual smooth surface pattern.
In the 5-year-old 290 (19.3%) male participants; 148 (51.0%) were caries free, 87 (30.0%) had pit and fissure pattern, 76 (26.2%) had maxillary anterior pattern, 74 (25.5%) had posterior proximal pattern, and 24 (8.2%) had posterior buccal/lingual smooth surface pattern. Among 278 (18.5%) 5-year-old female participants; 151 (54.3%) were caries free, 105 (37.8%) had pit and fissure caries, 40 (14.4%) had maxillary anterior pattern, 69 (24.8%) had posterior proximal pattern, and 22 (7.9%) had posterior buccal/lingual pattern.
When the age group of 3-, 4-, and 5-year-olds were assessed in total for pattern of caries, it was found that 37.7, 47.3, and 47.4% had caries; 29.3, 33.8, and 33.0% had pit and fissure caries; 16.9, 22.0, and 20.7% had maxillary anterior pattern; 13.5, 20.2, ad 25.1% had posterior proximal pattern; and 6.7, 7.8, and 8.09% had posterior buccal/lingual pattern; respectively.
Percentage distribution of the participants according to caries severity
In the 3-year-old participants; 23.3% surfaces had pit and fissure caries, 20.5% of the surfaces had maxillary anterior caries, 17.2% surfaces had posterior proximal caries, and 14.2% had posterior buccal/lingual smooth surface caries.
In the 4-year-old participants; 31.4% surfaces had pit and fissure caries, 30.5% surfaces had maxillary anterior caries, 19.8% surfaces had posterior proximal caries, and 19.4% had posterior buccal/lingual smooth surface caries.
In the 5-year-old participants; 26.4% surfaces had pit and fissure caries, 25.7% of the surfaces had maxillary anterior caries, 17.9% surfaces had posterior proximal caries, and 16.8% had posterior buccal/lingual smooth surface caries.
Treatment needs of the study participants
In present study, treatment needs of the study participants were calculated and it was found that; out of total study population, only 742 (49.4%) participants required treatment and 758 (50.5%) participants did not require any treatment. Among all the participants who required treatment; 30.4% participants required caries arresting sealant care, 35% participants required one surface filling, 20.6% participants required two surface fillings, 3.1% participants required pulp care, 7.05% participants required extraction, 1.4% required crown/bridge element, and 2.35% participants required space maintainer.
Discussion
The dental profession has to deal with one of the most widespread of all human maladies; dental caries.[12] It is neither self-limiting, like the common cold, nor amenable to treatment with a simple course of antibiotics, like an ear infection in children.[13,14]
Epidemiological studies from all over the world showed that dental caries is one of the most widely distributed dental diseases.[5] Dental caries in the early childhood has been a challenge to the dental profession as dental caries begins even before the 1st year of life.[15] Although there have been major advances in the field of pathogenesis and prevention of dental caries in the last 2 decades, still there are reports of a high prevalence of caries in preschool children.[16]
In India, the earliest references of dental caries status dates back to 1939, when Taylor and Day reported low prevalence of caries in children of Kangra valley, Punjab.[17] Shourie in 1941 for the first time in India conducted a multicentric epidemiological study in various parts of country in the age group of 5-7 years.[17] The results of that study showed caries prevalence of 46% with an average deft of 1.99 SD 2.80. Thereafter, a number of point prevalence studies have been conducted in different parts of the country and around the globe.
In the present study among total number of children examined for caries, 54% of the total children were caries free and 46% children had caries. Some studies[18,19] are in disagreement with the present study and have shown high prevalence (55 and 61%) of dental caries in preschool children, respectively. Some of the Indian studies by Dash et al.,[20] and Meghashyam et al.,[21] on preschool children have also found high prevalence (51 and 58%, respectively) of dental caries than the present study. Fung et al.,[22] reviewed studies in dental caries ranging from 17 to 94% prevalence rate across the globe.
There are differences in the caries status among different populations. The plausible explanation for such discrepancy can be inequality in economic conditions and resources, effective fluoridation policy, efficiency of healthcare system, availability and consumption of refined sugars, standard of oral health awareness among public, dietary and oral hygiene lifestyles, as well as motivational status of parents and children.
In a study conducted on London and Greece children of 5 years age group; the proportion of London children who were caries-free were 56%, and of Athens children 57.5% (Zoitopoulos et al., in 1996).[23] Study by Albert et al.,[24] in Brazil (67%), Skeie et al.,[25] (59.9%) in Norway, and Arora et al.,[26] in Greater Noida (62%), India, do not agree with the present study (54%) and have found higher level of caries-free children; whereas, Paul[27] (44%) in Saudi Arabia, Awooda et al.,[28] (39.3%) in Sudan, and Fernandes et al.,[29] (41.9%) in Brazil observed a lower caries-free children.
Caries prevalence was higher in boys (47%) compared to girls (42.5%), which is in conformity with the study of Saravanan et al.,[30] (51%). The numbers of caries-free children decreased as the age advanced. Similar findings were reported in other Indian studies by Tyagi.[31] The results of the present study indicate that deft increases as the age advances (1.40 SD 0.21 in 3 years, 2.0 SD 0.68 in 4 years, and 2.39 SD 1.65 in 5 years) and preschool children have high restorative need, similar findings were reported by Zoitopoulos et al.,[23] in Athens (2.71 SD 0.77 in 4 years, 3.01 SD 0.78 in 5 years) and Julie et al.,[4] in Arizona (1.79 SD 0.28 in 3 years, 2.27 SD 0.91 in 4 years, 2.78 SD 0.37 in 5 years). In contrast to the present study (1.99 SD 2.80), some studies in the western countries by Davies et al.,[32] in Greater Manchester (1.07 SD 0.89) and Ferro et al.,[33] in Italy (1.17 SD 0.70) on preschool children have reported low mean deft compared to the present study. Similarly, some Indian authors (Jose and King[34]) have also reported less deft in preschool children of Kerala (1.51 SD 0.49) compared to the present study. However, Manal et al.,[35] in 2-5-year-old children found mean high dmft (2.79 SD 1.90) and dmfs (4.08 SD 1.80) compared to the present study. The ‘d’ component (1.81 SD 2.55) in the present study constituted almost the entire deft index, which goes in accordance with studies by Ferro et al.,[33] in Italy (1.99SD.75), and Adekoya et al.,[36] in Nigeria (2.01 SD 0.91) on preschool children.
The percentage of decayed teeth decreased with advancing age, while that of missing and filled teeth increased with advancing age. In contradiction to the present study, a study from Saudi Arabia on preschool children by Hashim et al.,[37] concluded that mean mt and ft values for 3- and 4-year-olds was 0. Similarly, contrary to the present study, the proportion of decayed (d) missing/exfoliated (e) filled (f) components of preschool children reported by Mahejabeen et al.,[6] in Hubli, India (0.91 SD 0.56) were same for all age groups and def components did not show significant difference between both sexes. However, the mean deft scores show an increasing trend with age which is in accordance with the present study.
Decayed teeth formed the major component of total deft score, followed by teeth indicated for exfoliation or are missing due to caries (et component) and the least contribution was of filled teeth. Comparable proportions are evident in majority of studies. The attributed explanation might be that majority of children do not undergo dental restorations primarily because parents cannot afford high treatment cost, lack of affordable dental services, and false perceptions of parents regarding significance of retaining primary teeth; while those who undergo treatment prefer extraction rather than restorations. In the study by Mahejabeen et al.,[6] the caries pattern revealed that about 23% children had caries in the anterior teeth only, 50% had caries in posteriors, and 27% had caries in both anterior and posteriors, which is in disagreement with the present study. However, studies by Adekoya et al.,[36] in Nigeria (20% in anterior teeth region) and Maragakis et al.,[38] in Athens (20.7% in anterior teeth region and 31.9% pit and fissure caries) on preschool children are in concurrence with the present study.
Present study showed severity of maxillary anterior caries was more among 4-year-old participants (41.1%). The association between maxillary anterior caries and habit of frequent nocturnal bottle or breast feeding is established. This type of caries can be prevented by timely education to the new parents. The prevalence of posterior proximal and posterior buccal/lingual smooth surface caries is very less as compared to pit and fissure and maxillary anterior caries. Regarding treatment needs, 63.6% children required dental treatment for various reasons and is in conformity with the present study; whereas, results of Adekoya et al.,[36] (64%) are in disagreement with the present study.
There was the greatest need for one surface restoration (55.4%) followed by two or more surface restorations. Studies done by Saravanan et al.,[30] (54.7%), and Mahejabeen et al.,[6] (56.3%) are in line with the present study. Further research is suggested in order to explore and identify the prevailing etiological factors responsible for the current status.
Present study states the needs for treatment of dental caries, as of sex, the treatment need was higher for males compared to females as caries experience was more among males. The possible reason for this can be that in the rural parts of India, still the male child is more preferred over the girl child and is well fed and pampered as compared to girl child. In this study, filling component recorded was very less among both males and females of all age groups; this indicates lack of utilization of dental care facilities which could be due to ignorance, poverty, and lack of knowledge/time. Hence, this study focuses the importance of creating awareness among parents/teachers, and provision of dental services to this group. Herbal formulations or herb based mouthwashes can also be advocated to decease the caries risk.[39,40,41,42,43,44,45,46,47,48,49,50]
Conclusion
Health promotion and education programs in Anganwadi should include oral health issues and the risk factors for caries in preschool children, and its consequences should be addressed. The dental profession should be aware of its responsibilities and be prepared to play its part in improving the dental health of preschool children. Doctors, health visitors, teachers, and parents play a vital role in maintenance of good oral health of children.
Dental health programs should be undertaken in these institutions including dental health education, dental health, and healthy environment. In the present study, only prevalence of dental caries and different types of caries pattern and treatment needs was estimated. Hence, further studies among this population should be taken up to correlate socioeconomic status, feeding habits, and oral hygiene habits with dental caries pattern.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Pongpichit B, Sheiham A, Pikhart H, Tsakos G. Time absent from school due to dental conditions and dental care in Thai school children. J Public Health Dent. 2008 Spring;68:76–81. doi: 10.1111/j.1752-7325.2007.00051.x. [DOI] [PubMed] [Google Scholar]
- 2.Agbelusi GA, Jeboda SO. Oral health status of 12 years old Nigerian children. West Afr J Med. 2006;25:195–8. doi: 10.4314/wajm.v25i3.28277. [DOI] [PubMed] [Google Scholar]
- 3.Diehnelt DE, Kiyak HA. Socioeconomic factors that affect international caries levels. Community Dent Oral Epidemiol. 2001;29:226–33. doi: 10.1034/j.1600-0528.2001.290309.x. [DOI] [PubMed] [Google Scholar]
- 4.Tang JM, Altman DS, Robertson DC, O’Sullivan DM, Douglass JM, Tinanoff N. Dental caries prevalence and treatment levels in arizona preschool children. Public Health Rep. 1997;112:319. [PMC free article] [PubMed] [Google Scholar]
- 5.Edelstein BL. The dental caries pandemic and disparities problem. BMC Oral Health. 2006;6:S2. doi: 10.1186/1472-6831-6-S1-S2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Mahejabeen R, Sudha P, Kulkarni SS, Anegundi R. Dental caries prevalence among preschool children of Hubli: Dharwad city. J Indian Soc Pedod Prev Dent. 2006;24:19–22. doi: 10.4103/0970-4388.22829. [DOI] [PubMed] [Google Scholar]
- 7.Tyagi R. The prevalence of nursing caries in Davangere preschool children and its relationship with feeding practices and socioeconomic status of the family. J Indian Soc Pedod Prev Dent. 2008;26:153–7. doi: 10.4103/0970-4388.44030. [DOI] [PubMed] [Google Scholar]
- 8.Waldman HB. Preschool children. Need and use of dental services. Dent Clin North Am. 1995;39:887–96. [PubMed] [Google Scholar]
- 9.Retnakumari N. Prevalence of dental caries and risk assessment among primary school children of 6-12 years in the Varkala municipal area of Kerala. J Indian Soc Pedod Prev Dent. 1999;17:135–42. [PubMed] [Google Scholar]
- 10.Milen A, Hausen T, Tala H, Paunio I, Heinonen OP. Caries in 3-5 years-old, Finnish children participating in public dental car during 1975-79. Community Dent Oral Epidemiol. 1981;9:270–4. doi: 10.1111/j.1600-0528.1981.tb00344.x. [DOI] [PubMed] [Google Scholar]
- 11.Jain A, Bhaskar DJ, Gupta D, Agali C, Gupta V, Gupta RK, et al. Comparative evaluation of honey, chlorhexidine gluconate (0.2%) and combination of xylitol and chlorhexidine mouthwash (0.2%) on the clinical level of dental plaque: A 30 days randomized control trial. Perspect Clin Res. 2015;6:53–7. doi: 10.4103/2229-3485.148819. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Gupta D, Bhaskar DJ, Gupta RK. Contemporary and alternative dentistry: Ayurveda in dentistry. Saarbrücken: Lap Lambert Academic Publishing. 2013:28–30. [Google Scholar]
- 13.Gupta D, Bhaskar DJ, Gupta RK, Karim B, Jain A, Singh R, et al. A randomized controlled clinical trial of Ocimum sanctum and chlorhexidine mouthwash on dental plaque and gingival in ammation. J Ayurveda Integr Med. 2014;5:109–16. doi: 10.4103/0975-9476.131727. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Narinder, Tewari A, Chawla HS. Intercomparison of sugar and dental caries relationship in urban and rural children. J Indian Soc Pedod Prev Dent. 1986;4:52–60. [PubMed] [Google Scholar]
- 15.Babeely K. The relationship between the severity of nursing bottle caries and and feeding patterns. J Indian dent Assoc. 1987;66:327–30. [Google Scholar]
- 16.Gupta D, Nagar P, Karim B, Khan IM, Naveen B, Chaturvedi M, et al. Tobacco abuse amongst the school going students of 15 to 18 years of Almora district, Uttarakhand: a cross sectional study. Oral Health Dent Manag. 2014;13:680–6. [PubMed] [Google Scholar]
- 17.Gupta D, Gupta RK. Investigation of antibacterial efficacy of Acacia nilotica against salivary mutans streptococci: a randomized control trial. Gen Dent. 2015;63:23–7. [PubMed] [Google Scholar]
- 18.Seow WK, Amaratunge A, Bennett R, Bionscb D, Lai PY. Dental health of aboriginal pre-schools children in Brisbane, Australia. Community Dent Oral Epidemiol. 1996;24:187–90. doi: 10.1111/j.1600-0528.1996.tb00839.x. [DOI] [PubMed] [Google Scholar]
- 19.Yam AA, Ba M, Faye M, Sane DD. Caries and gingivitis study among preschool children (2-5 years) of the region of Ziguinchor in Senegal. Strategies of prevention. Dakar Med. 2000;45:180–4. [PubMed] [Google Scholar]
- 20.Dash JK, Sahoo P, Bhuyan K, Sahoo SK. Prevalence of dental caries and treatment needs among children of Cuttack (Orissa) J Indian Soc Pedod Prev Dent. 2002;20:139–43. [PubMed] [Google Scholar]
- 21.Meghashyam B, Nagesh L, Ankola A. Dental caries status and treatment needs of children of fisher folk communities, residing in the coastal areas of Karnataka region, south India. West Indian Med J. 2007;56:96–8. doi: 10.1590/s0043-31442007000100018. [DOI] [PubMed] [Google Scholar]
- 22.Fung MH, Wong MC, Lo EC, Chu CH. Early Childhood Caries: A Literature Review. Oral Hyg Health. 2013;1:107–10. [Google Scholar]
- 23.Zoitopoulos L, Athanassouli T, Gelbier S, Apostolopoulos A. Caries prevalence of 5-year-old children in Athens and in South London. Int J Paediatr Dent. 1996;6:3–6. doi: 10.1111/j.1365-263x.1996.tb00200.x. [DOI] [PubMed] [Google Scholar]
- 24.Albert DA, Park K, Findley S, Mitchell DA, McManus JM. Dental caries among disadvantaged 3- to 4-year-old children in northern Manhattan. Pediatr Dent. 2002;24:229–33. [PubMed] [Google Scholar]
- 25.Skeie MS, Espelid I, Skaare AB, Gimmestad A. Caries patterns in an urban preschool population in Norway. Eur J Paediatr Dent. 2005;6:16–22. [PubMed] [Google Scholar]
- 26.Arora SA, Setia S, Ahuja P, Singh D, Chandna A. Prevalence of dental caries among pre-school children of Greater Noida city. Indian J Dent Sci. 2012;2:4–6. [Google Scholar]
- 27.Paul TR. Dental health status and caries pattern of preschool children in Al-Kharj, Saudi Arabia. Saudi Med J. 2003;24:1347–51. [PubMed] [Google Scholar]
- 28.Awooda EM, Saeed SM, Elbasir EI. Caries prevalence among 3-5 years old children in Khartoum State Sudan. Innov J Med Health Sci. 2013;3:42–4. [Google Scholar]
- 29.Fernandes JM, Paredes SO, Almeida DB, Sampaio FC, Forte FD. Prevalence of dental caries and treatment needs in preschool children in a recently fluoridated Brazilian town. Braz J Oral Sci. 2009;8:185–8. [Google Scholar]
- 30.Saravanan S, Madivanan I, Subashini B, Felix JW. Prevalence pattern of dental caries in the primary dentition among school children. Indian J Dent Res. 2005;16:140–6. doi: 10.4103/0970-9290.29907. [DOI] [PubMed] [Google Scholar]
- 31.Tyagi P. The prevalence and pattern of dental caries in pre-school children. People's J Sci Res. 2009;2:1–4. [Google Scholar]
- 32.Davies GM, Blinkhorn FA, Duxbury JT. Caries among 3-year-olds in greater Manchester. Br Dent J. 2001;190:381–4. doi: 10.1038/sj.bdj.4800979. [DOI] [PubMed] [Google Scholar]
- 33.Ferro R, Besostri A, Meneghetti B. Dental caries experience in preschool children in Veneto region (Italy) Community Dent Health. 2006;23:91–4. [PubMed] [Google Scholar]
- 34.Jose B, King NM. Early childhood caries lesions in preschool children in Kerala, India. Pediatr Dent. 2003;25:594–600. [PubMed] [Google Scholar]
- 35.Al-Malik MI, Holt RD, Bedi R. Prevalence and patterns of caries, rampant caries, and oral health in two- to five-year-old children in Saudi Arabia. J Dent Child (Chic) 2003;70:235–42. [PubMed] [Google Scholar]
- 36.Adekoya C, Sofowora, Nasir WO, Taiwo M, Adesina OA. Caries experience in the primary Dentition of Nursery School Children in Ile-Ife, Nigeria. Afr J Oral Health. 2006;2:19–25. [Google Scholar]
- 37.Hashim R, Thomson WM, Ayers KM, Lewsey JD, Awad M. Dental caries experience and use of dental services among preschool children in Ajman, UAE. Int J Paediatr Dent. 2006;16:257–62. doi: 10.1111/j.1365-263X.2006.00746.x. [DOI] [PubMed] [Google Scholar]
- 38.Maragakis GM, Kapetanakou DN, Manios Y. Caries prevalence and location and dental treatment needs in preschoolers in Athens - GENESIS project. Community Dent Health. 2007;24:264–7. [PubMed] [Google Scholar]
- 39.Gupta D, Gupta RK, Bhaskar DJ, Gupta V. Comparative Evaluation of Terminalia chebula Extract Mouthwash and Chlorhexidine Mouthwash on Plaque and Gingival Inflammation - 4 - week Randomised Control Trial. Oral Health Prev Dent. 2015;13:5–12. doi: 10.3290/j.ohpd.a32994. [DOI] [PubMed] [Google Scholar]
- 40.Gupta D, Dalai DR, Swapnadeep, Mehta P, Indra BN, Rastogi S, et al. Acupuncture (zhçn jiŭ) - an emerging adjunct in routine oral care. J Tradit Complement Med. 2014;4:218–23. doi: 10.4103/2225-4110.139113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Gupta RK, Gupta D, Bhaskar DJ, Yadav A, Obaid K, Mishra S. Preliminary antiplaque efficacy of aloe vera mouthwash on 4 day plaque re-growth model: randomized control trial. Ethiop J Health Sci. 2014;24:139–44. doi: 10.4314/ejhs.v24i2.6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Gupta D, Bhaskar DJ, Gupta RK, Karim B, Gupta V, Punia H, et al. Effect of Terminalia chebula extract and chlorhexidine on salivary pH and periodontal health: 2 weeks randomized control trial. Phytother Res. 2014;28:992–8. doi: 10.1002/ptr.5075. [DOI] [PubMed] [Google Scholar]
- 43.Gupta D, Bhaskar DJ, Gupta KR, Karim B, Kanwar A, Jain A, et al. Use of complementary and alternative medicine for work related musculoskeletal disorders associated with job contentment in dental professionals: Indian outlook. Ethiop J Health Sci. 2014;24:117–24. doi: 10.4314/ejhs.v24i2.3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Gupta D, Bhaskar DJ, Gupta RK, Jain A, Yadav P, Dalai DR, et al. Is complementary and alternative medicine effective in job satisfaction among dentists with musculoskeletal disorders. A cross sectional study? Med Pr. 2014;65:317–23. [PubMed] [Google Scholar]
- 45.Gupta D, Batra R, Mahajan S, Bhaskar DJ, Jain A, Shiju M, et al. Comparative Evaluation of the Complementary and Alternative Medicine Therapy and Conventional Therapy Use for Musculoskeletal Disorders Management and Its Association with Job Satisfaction among Dentists of West India. J Tradit Complement Med. 2014;4:218–23. doi: 10.4103/2225-4110.126632. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Randhawa RK, Gupta N, Arora V, Gupta P. Antioxidants in oral health. Inter J Contempor Med Res. 2015;2:53–58. [Google Scholar]
- 47.Sood S, Bhargava M, Rathore P. Diabetes Mellitus Leading Expiry of Oral Health. Inter J Contempor Med Res. 2015;2:100–4. [Google Scholar]
- 48.Raghav P, Jain S, Reedy M, Singh S, Phull TS, Verma RK. Evaluation of nasal form in average, pleasing and attractive looking individuals. Inter J Contempor Med Res. 2015;2:12–19. [Google Scholar]
- 49.Megalaa N, Kayalvizhi G, Silas AJ, Sajeev R, Saravana Kumar MS. Role of herbal leaf extracts in caries prevention. Inter J Contempor Med Res. 2014;1:71–78. [Google Scholar]
- 50.Gupta D, Nayan S, Tippanawar HK, Patil GI, Jain A, Gupta RK. Are herbal mouthwash efficacious over chlorhexidine on the dental plaque? Phcog Res [Epub ahead of print] doi: 10.4103/0974-8490.155874. DOI: 10.4103/0974-8490.155874. [DOI] [PMC free article] [PubMed] [Google Scholar]