

Abstract
Background:
Dental caries and deviations from normal weight are two conditions which share several broadly predisposing factors. So it's important to understand any relationship between dental state and body weight if either is to be managed appropriately.
Aims:
The study was done to find out the correlation between body mass index (BMI), diet, and dental caries among 12-15-year-old schoolgoing children in Panchkula District.
Materials and Methods:
A multistage sample of 12-15-year-old school children (n = 810) in Panchkula district, Haryana was considered. Child demographic details and diet history for 5 days was recorded. Data regarding dental caries status was collected using World Health Organization (1997) format. BMI was calculated and categorized according to the World Health Organization classification system for BMI. The data were subjected to statistical analysis using chi-square test and binomial regression developed using the Statistical Package for Social Sciences (SPSS) 20.0.
Results:
The mean Decayed Missing Filled Teeth (DMFT) score was found to be 1.72 with decayed, missing, and filled teeth to be 1.22, 0.04, and 0.44, respectively. When the sample was assessed based on type of diet, it was found that vegetarians had higher mean DMFT (1.72) as compared to children having mixed diet. Overweight children had highest DMFT (3.21) which was followed by underweight (2.31) and obese children (2.23). Binomial regression revealed that females were 1.293 times at risk of developing caries as compared to males. Fair and poor Simplified-Oral Hygiene Index (OHI-S) showed 3.920 and 4.297 times risk of developing caries as compared to good oral hygiene, respectively. Upper high socioeconomic status (SES) is at most risk of developing caries. Underweight, overweight, and obese are at 2.7, 2.5, and 3 times risk of developing caries as compared to children with normal BMI, respectively.
Conclusion:
Dental caries and deviations from normal weight are two conditions which share several broadly predisposing factors such as diet, SES, lifestyle and other environmental factors.
Keywords: Binomial regression, body mass index, dental caries, school children
Introduction
Dental caries during childhood continues to be significant public health concern. This disease not only causes damage to the tooth but also responsible for several morbid conditions in the oral cavity and other systems of the body.[1] Dental caries is the major oral health problem in developing countries, affecting 60-90% of the school children and the vast majority of adults.[2] In India, the prevalence of dental caries is reported to be 50-60%.[3] Incidence of dental caries is on the rise in spite of best efforts by dental health professionals to reduce its incidence.[4] Dental caries is a multifactorial infectious disease.[5] Factors affecting the onset of carious lesions include poor oral hygiene, nutrition, socioeconomic status (SES), salivary immunoglobulins, and bacterial load.[6]
Every human being has the right to access adequate, sufficient, and healthy nutrition. However, social inequalities, changes in lifestyle, the process of industrialization, and other factors have had a negative influence on the spread of this fundamental right.[7] Today the world faces two kinds of problem, one associated with hunger or nutritional deficiency and the other with dietary excess. Urbanization and economic development has resulted in rapid changes in diet and lifestyles.[8]
The body mass index (BMI) has always been considered a simple method for analysis of the nutritional status.[4] Dental caries and deviations from normal weight are two conditions which share several broadly predisposing factors such as diet, SES, lifestyle, and other environmental factors.[9] From the point of view both of public health and of individual healthcare it is important to understand any relationship between dental state and body weight if either are to be managed appropriately.[10]
While it seems plausible that there is positive correlation between deviation of body weight and caries prevalence, the evidence is highly variable. There is need to accurately identify children who are at high risk of poor oral health in order to commence and target prevention appropriately from young age. Studies are sparse in this region of the country on nutritional status and prevalence of dental caries. The aims of the study were to investigate specifically the correlation between BMI, diet, and dental caries among 12-15-year-old schoolgoing children in Panchkula District, Haryana, India.
Materials and Methods
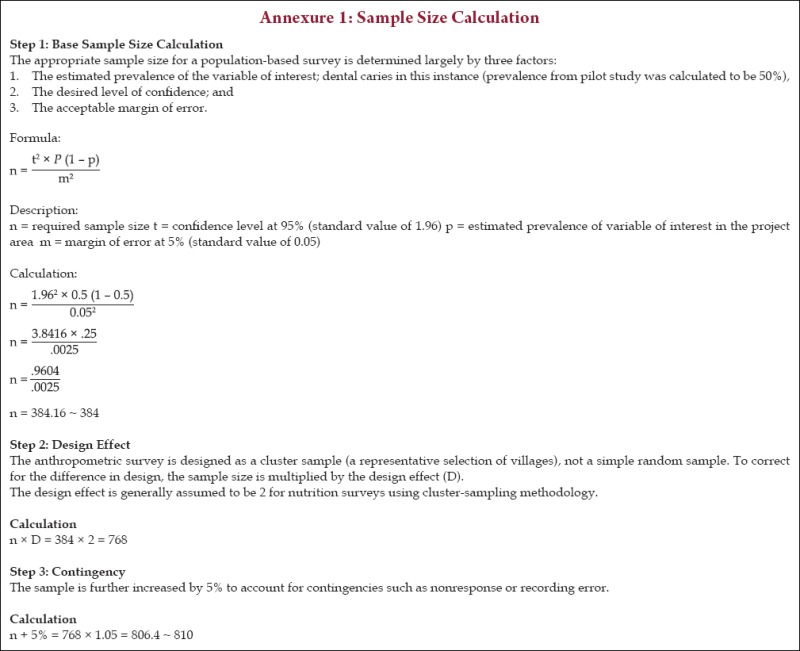
A cross-sectional study was conducted over a period of 6 months from April 2013 to September 2013 among 12-15-year-old schoolgoing children of Panchkula District, Haryana. Ethical clearance was obtained from the institutional ethical committee. A written consent was taken from the parents/primary caregivers and an oral informed consent was obtained from the participants before the complete oral examination was carried. A pilot study was conducted 1 month prior to the original study with a sample of 80 individuals who were not part of the main sample. Prevalence of dental caries was found to be 50%. Based on results of pilot study, sample size was calculated to 810 [Annexure 1].
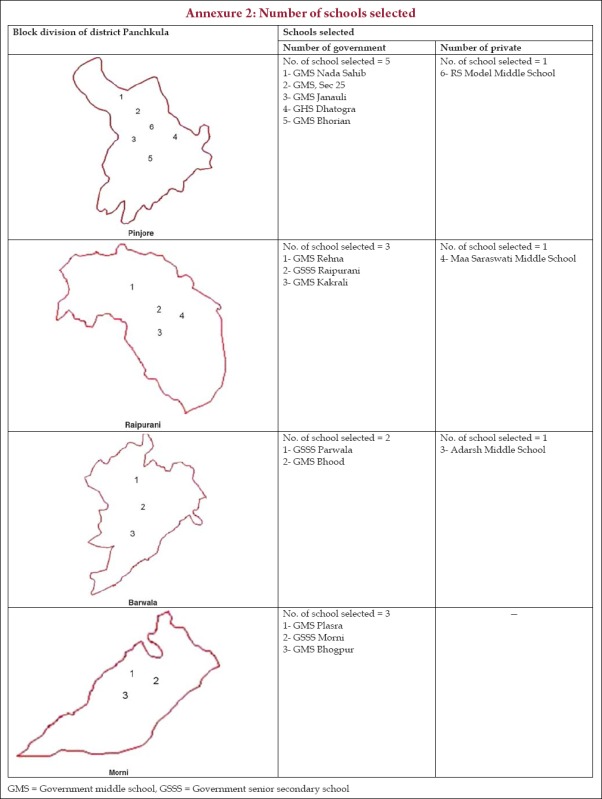
A multistage sampling technique was adopted to select the children. The primary sampling unit consists of four blocks of Panchkula (i. e., Pinjore, Raipur Rani, Barwala, and Morni). Within each block, the schools were randomly selected proportional to number of private and government schools and the total number of school going children [Annexure 2].
Before examining the children, the consent was obtained from the concerned authorities of education department and principal of respective schools of the District Panchkula. All the children belonging to the age group of 12-15 years and who were available on the day of examination in the selected schools were examined till the desired sample size was achieved. Children having any chronic illness, severe malnutrition, endocrinal problems, physical and mental defects, undergoing orthodontic treatment, those with apparent obesity induced or associated with any syndrome, those found to be smokers (defined as any amount of smoking or tobacco chewing at any time during past 6 months), and those not cooperating for anthropometric measurements were excluded.
All the recruited children received clinical examinations by two trained and calibrated examiners (one measuring BMI and one examining for dental caries). The examination procedure was double blinded. A presurvey calibration was performed on group of 30 subjects in the age group of 12-15 years who were chosen from the school oral health programme conducted by Dental Institution. The results so obtained were subjected to kappa statistics. The calibration exercise and the kappa value (0.95) showed good agreement for these observations and measurements in terms of intraexaminer variability which validated the examination procedure.
A pro forma (consisting of children demographic details, family income, past dental history, any relevant medical history, and diet history of 5 days) was distributed to all the students prior to the examination. After 5 days pro forma was collected.
Students were than examined with mouth mirror, explorer under natural light/torch as per guidelines of American Dental Association for Type III examination. Data regarding dental caries status was collected using World Health Organization (WHO, 1997) format.[11] The weight of the subjects in kilograms was recorded using standard physician's scale. The height of the subjects in meters was recorded using stadiometer. Then, calculation of BMI (kg/m2) was done and categorized using WHO classification system for BMI.[12]
Diet analysis was done using criteria given by Nizzle[13] and SES was assessed using Parsad's Socioeconomic Classification.[14]
Statistical study
The data were processed and analyzed by means of Statistical Package for Social Sciences (SPSS) PC version 20.0 (Chicago, IL, USA). Descriptive statistical analysis was been carried out in the present study to assess BMI. Results on continuous measurements were presented on mean ± SD (95% CI) and results on categorical measurements are presented in number (%). Chi-square test and analysis of variance had been used to find the significance of children with caries according to BMI in gender, age, SES, Simplified-Oral Hygiene Index (OHI-S), and other covariates. Binomial regression analysis has been carried out to find the significant correlation of independents with caries.
Results
Study population consisted of 810 children, of which 459 (56.7%) were males and 351 (43.3%) were females. Based on age, the study population belonging to 12, 13, 14, and 15 years consisted of 283, 193, 170, and 164 respectively.
The mean score of decayed, missing, and filled teeth were 1.22, 0.04, and 0.44, respectively. Mean DMFT score was found to be more among females (1.82) as compared to males (1.64). This value was not found to be significant (P - value > 0.05) [Figure 1]. As the age increases the mean DMFT score also increases. Mean DMFT was found to be highest among 15-year-olds (DMFT = 1.82) and lowest among 12-year-old (1.66) children, but this was not found to be statistically significant (P - value > 0.05) [Figure 2].
Figure 1.
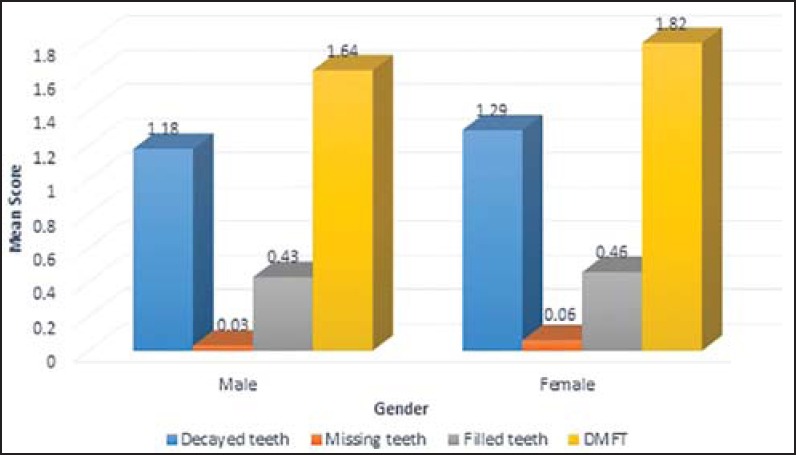
Mean DMFT according to gender. DMFT = Decayed Missing Filled Teeth
Figure 2.
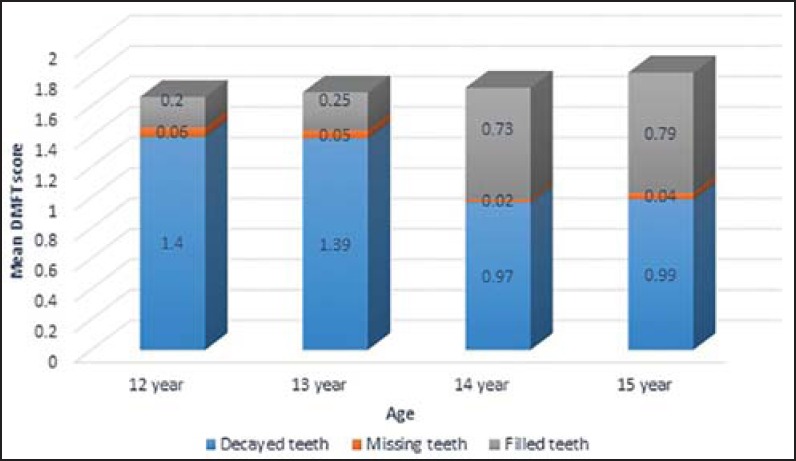
Mean DMFT according to age
Based on SES, mean decayed score was found to be highest among children with poor SES (1.85). Mean missing tooth was found to be highest in children who belong to lower middle class (0.10). Mean filled tooth score was found to be highest in children with upper high class (1.81). DMFT score was observed to be highest in upper high class (2.43) [Figure 3].
Figure 3.
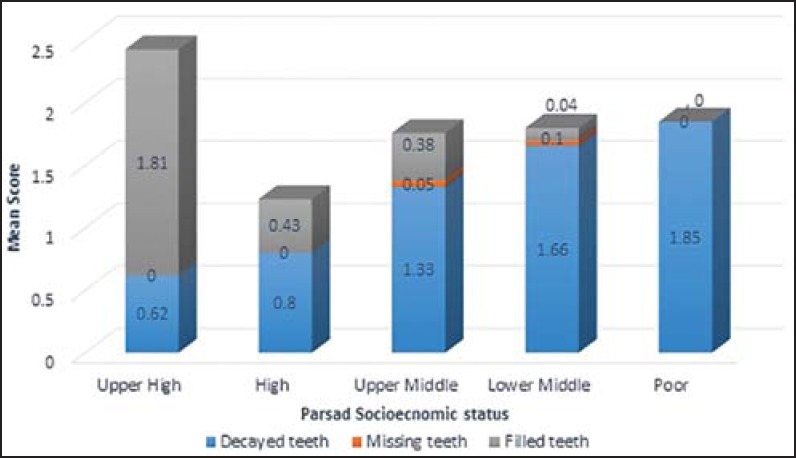
Mean DMFT according to Parsad's socioeconomic status
Based on type of schooling, mean decayed (1.46) and missing score (0.06) was found to be more in government school children; whereas, mean filled score (0.79) was found to be more in private school children. The overall mean DMFT score was found to be more in government school children (1.75) than private school children (1.66) [Figure 4].
Figure 4.
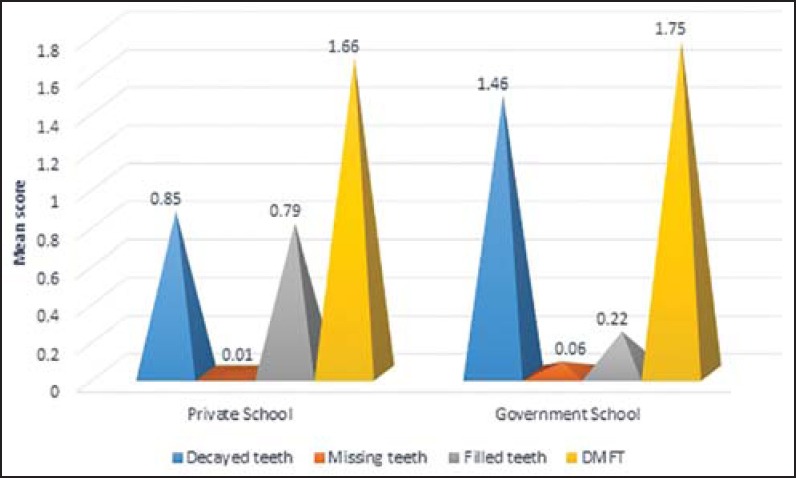
Mean DMFT according to type of schooling
Mean decayed score was observed to be more in children who had not visited dentist (1.34) as compared to children who had visited the dentist (0.74). Mean filled score was more in children who had past dental visit (2.02) as compared to children who did not have past dental visit (0.05). This was found to be statistically significant. Pain (39.8%) followed by decayed tooth (24.8%) was most common reason for visiting dentist.
The vegetarians had higher DMFT (1.72) as compared to mixed diet children (1.70). Children with 75-89 oral health diet (OHD) score had higher mean DMFT followed by children with OHD score of 59 and below and 60-74, respectively. But values were not found to be statistically significant [Figure 5].
Figure 5.
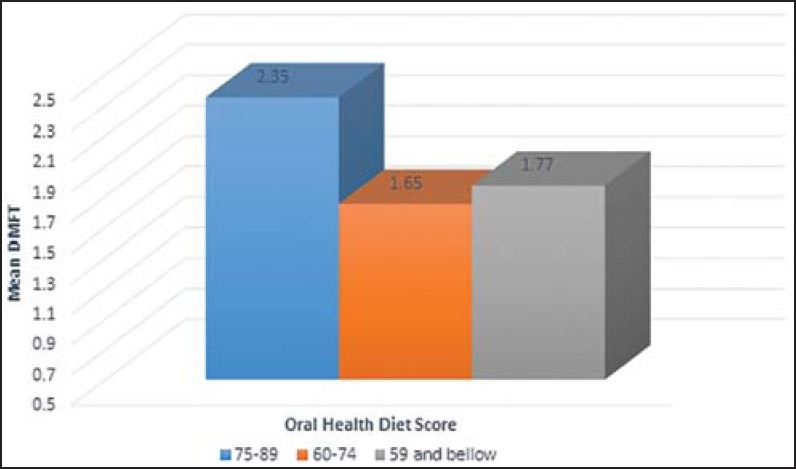
Mean DMFT according to oral health diet score
Children with poor OHI-S had highest mean DMFT (3.48) which was found to be statistically significant (P < 0.05) [Figure 6].
Figure 6.
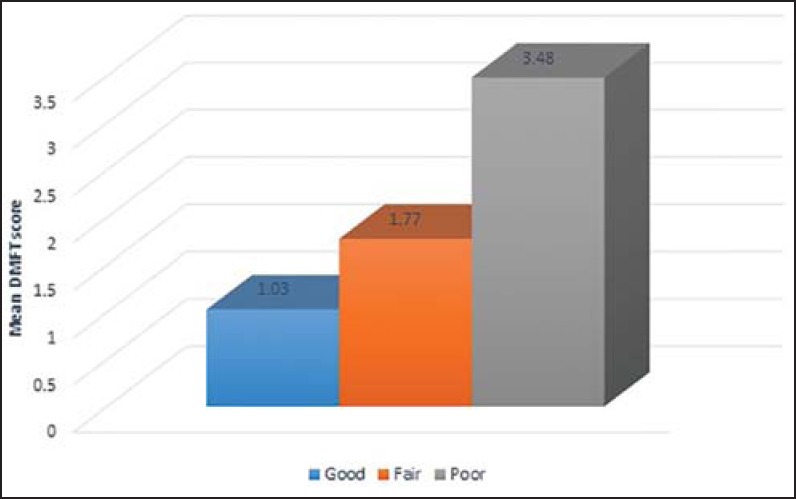
Mean DMFT according to Oral Hygiene Index-Simplified
The prevalence of underweight, normal weight, overweight, and obese was 13.6, 58.4, 22.7, and 5.3%, respectively. Overweight children had highest mean DMFT (3.21), which was followed by underweight (2.31) and obese children (2.23). This value was found to be statistically significant. (P < 0.05) [Figure 7].
Figure 7.
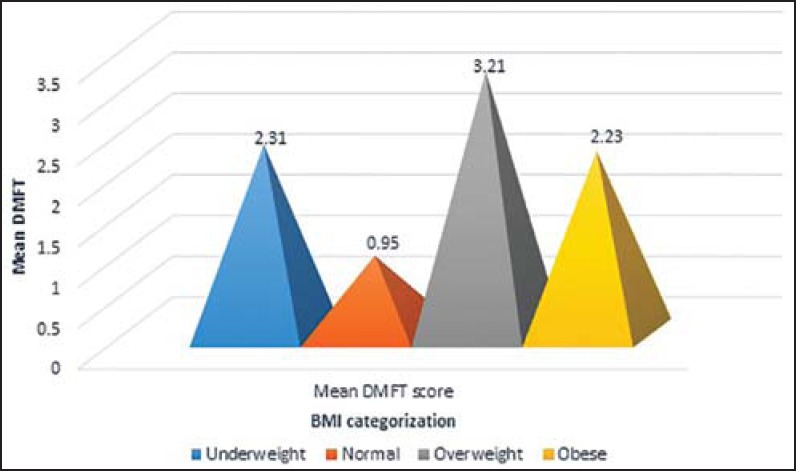
Mean DMFT according to BMI. BMI = Body mass index
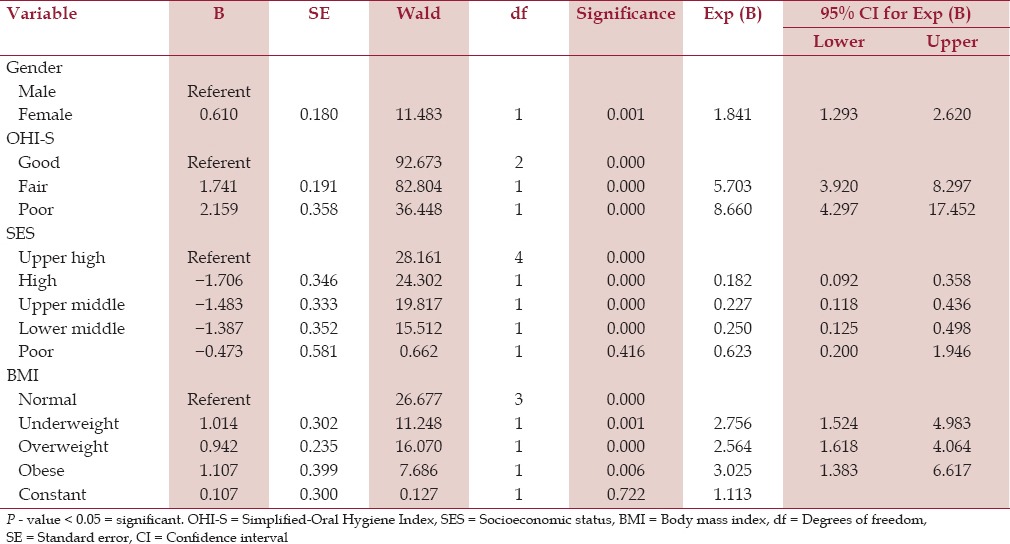
Females were 1.293 times at risk of developing caries as compared to males. Fair and poor OHI-S showed 3.920 and 4.297 times risk of developing caries as compared to good oral hygiene, respectively. Upper high SES is at most risk of developing caries. Underweight, overweight, and obese are at 2.7, 2.5, and 3 times risk of developing caries as compared to children with normal BMI [Table 1].
Table 1.
Relationship of caries with gender, OHI-S, SES, and BMI
Discussion
Modernization brings with it the ill effects such as reduced outdoor activity, while encouraging snacking combined with an unprecedented abundance of cheap and consumption of energy dense food.[15,16] In the developing world, these nutritional transitions that involve more junk food and together with complacent activities have been associated with rapidly growing rates of overweight.[17] Despite the escalating problem of obesity, underweight also remains a major problem in the developing countries.[18] Overweight and underweight both exhibiting the cumulative environmental effects of dietary factors which could be responsible for the higher rates of dental caries in these children.[19] Given the link between refined carbohydrate consumption and dental caries and link between dietary intake and overweight; it is appropriate to hypothesize that food choices, dietary habits, BMI, and SES are interrelated.[20]
There are conflicting reports in literature on the association between BMI and dental caries among different populations. Also, there is limited data available in India regarding the association between BMI and oral health outcomes. Hence, this cross-sectional study was undertaken to determine the association of BMI with dental caries.
Children in the age group of 12 and 15 years were chosen for this study, as these are global monitoring ages for dental caries as mentioned by WHO for international comparisons and monitoring of disease trends.[11] The range from 12 to 15 years was selected to have sufficient sample size.
Children of both genders were considered to take into account the gender differences in the amount of body fat due to differences in the growth milestones, body structure, and hormonal effects. School children from both public and private schools were included in order to have children from all the social, economic, and cultural backgrounds.
The mean decayed, missing, and filled score was found to be 1.22, 0.04, and 0.44, respectively. The reason for the high proportion of unrestored teeth in study children was that dental services were expensive. Furthermore, lack of dental awareness and low priority placed on oral health care compared with other needs could be responsible for not restoring teeth.
In the present study, caries prevalence was higher among females (mean DMFT = 1.82) than males (mean DMFT = 1.64), which was not statistically significant. Similar results were obtained by Yee and McDonald (2002);[21] Augusto et al., (2003);[22] Jamelli et al., (2010);[7] and Narang et al., (2012).[23] On application of binomial regression analysis, females were found to be 1.84 times risk of developing caries than males. The results were in concordance with study done by Chu et al., (2013)[24] who found the females were 1.34 times risk of developing caries than males. This is perhaps due to the fact that girls are having the habit of taking snacks between meals because of their longer indoor stay in comparison to boys who mostly spend time in outdoor activities. It may also be attributed to the fact that girls’ permanent teeth erupt at an earlier age than boys’ teeth.[25] Other risk factors for girls include a different salivary composition and flow rate, hormonal fluctuations, dietary habits, genetic variations, and particular social roles among their family.[26]
The caries prevalence was slightly higher among children with vegetarians than children having mixed diet. The value was not found to be significant; this could be due to small sample in mixed diet group. Further, it might be suggested that the persons who consume plenty of protein rich food in comparison to sugar, will develop less amount of acid in their mouth and relatively be protected from dental caries. It might be the reason for less number of cases among the nonvegetarian (mixed diet) population.[27,28]
Children with poor OHI-S had highest mean DMFT (3.48), which was found to be statistically significant (P < 0.05). Further on application of binomial regression, it was found that fair and poor OHI-S is 3.920 and 4.297 times risk of developing caries as compared to good oral hygiene, respectively.
Caries prevalence was more among government school children (mean DMFT = 1.75) than private school children (mean DMFT = 1.66). Similar results have been obtained in the study conducted by Yee and McDonald (2002)[21] and Augusto et al., (2003).[22] High caries prevalence among government school children may be due to difference in the SES and parent's education level, which in turn may influence the oral hygiene practices and dietary habits.
In the present study, the mean DMFT at 12 years and 15 years was 1.66 and 1.82, respectively; similar values were also reported by Bhardwaj and Sharma (2011)[28] and Naidu et al., (2006).[29] The reason for the higher prevalence of dental caries at 15 years as compared to 12 years is that caries being a continuous and cumulative process increases with age in any population independent of gender, urbanization, and social status; probably due to longer exposure time of the dentition to the etiologic factors of caries; moreover, the number of teeth is more at the age of 15 years.
Studies, primarily cross-sectional surveys that have assessed the association between SES and caries have given varied reports. Sogi and Bhaskar (2002)[30] have found that children with low SES tend to have more caries. In our study, although a higher number of children belonging to upper high class showed caries. Access to money in children from upper class families has a direct influence on sweet snacking, which leads to higher caries prevalence.[31]
Regarding the central issue of the study, the present study findings showed an increase in mean DMFT scores from normal to obese, underweight, and overweight. These findings might illustrate that the relationship between BMI and dental caries in children is far more complex than can be explained by carbohydrate consumption alone. When binomial regression was used, the obese were at maximum risk of developing caries. This was in accordance with studies that reported high caries scores in children with a high BMI.[19,32,33,34,35] Caries is higher in obese children due to increased intake and prolonged exposure to carbohydrates in various dietary forms.[36]
On the contrary, studies done on US children have shown that overweight children were less likely to have caries than normal weight children. This is because in the US, overweight is a public health concern with a lot of emphasis given to proper health education and dietary counseling to the parents of these children.[20]
Our study shows that the children with normal BMI had less caries in their permanent teeth, than the overweight children. This is in accordance with a German study which reported that children with normal weight had significantly lower caries scores in the primary and permanent dentition than overweight children.[37] Both overweight and dental caries are diet-based conditions, wherein, children with excessive ingestion of fermentable carbohydrates have a higher prevalence of dental caries.
In our study caries was not confined to any particular BMI category and socioeconomic class. This indicates that body weight exhibits the cumulative environmental effects of dietary factors, which could be responsible for the occurrence of caries in various socioeconomic classes. Research should be conducted to address what factors specific to body weight might be responsible for caries in children and adolescents.
The present study is an attempt to find if there is any relationship between BMI and dental caries. It should be remembered that the concept of biological plausibility suggests that neither the hypothesis “obesity increases risk of caries” nor “caries increases the risk of obesity” is particularly logical. Rather, it is more realistic that a common risk factor increases the likelihood of both diseases, which are then observed in association.
This study had some limitations:
Since the data were cross-sectional, causal relationships cannot be established and the observed association could be due to other unexplored factors;
Caries detection was carried out visually, without taking radiographs;
Non-schoolgoing children were not studied; and
Only qualitative and not quantitative analysis of diet was done in our study.
As most of the diet taken by Indians is custom made, it is difficult to assess the calorific value of such diet which might give an exact picture about the diet's influence on body weight. Besides, risk factors for childhood obesity could not be directly studied as this information was not specifically sought for in the original study.
Summary
The present study was probably the first of its kind in Panchkula, to find out the correlation between BMI, diet, and dental caries among 12-15-year-old schoolgoing children in Panchkula District.
The study revealed that overweight children had highest DMFT (3.21), which was followed by underweight (2.31) and obese children (2.23). The binomial regression revealed that females were 1.293 times at risk of developing caries as compared to males. Fair and poor OHI-S showed 3.920 and 4.297 times risk of developing caries as compared to good oral hygiene. Upper high SES is at most risk of developing caries. Underweight, overweight, and obese are 2.7, 2.5, and 3 times risk of developing caries as compared to children with normal BMI.
It may be concluded that, based on the findings of this study that dental caries and deviations from normal weight are two conditions which share several broadly predisposing factors such as diet, SES, lifestyle, and other environmental factors. Further investigation on the relationship between physical activity, gender, SES, BMI, and dental caries should be carried out. Physicians and dentists treating young children should consider that deviation from weight is a risk marker for childhood caries. Continuous education and motivation of parents and children can help to some extent to improve their health status.
Annexure 1: Sample Size Calculation
Annexure 2: Number of schools selected
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Singh RD, Khatter R, Bal CS. Prevalence of dental caries among school going children of Amritsar city in relation of different associated factors. Indian J Compr Dent Care. 2011;1:25–9. [Google Scholar]
- 2.World Health Organization. Continuous improvement of oral health in the 21st century- the approach of the WHO Global Oral Health Programme. Geneva: WHO; 2003. The World Oral Health report 2003. [DOI] [PubMed] [Google Scholar]
- 3.Shah N. Oral and dental diseases: Causes, prevention and treatment strategies: Burden of disease. Natl Comm Macroecon Health. 2005:275–98. [Google Scholar]
- 4.Hong L, Ahmed A, McCunniff M, Overman P, Mathew M. Obesity and dental caries in children aged 2-6 Years in the United States: National Health and Nutrition Examination Survey 1999-2002. J Public Health Dent. 2008;68:227–33. doi: 10.1111/j.1752-7325.2008.00083.x. [DOI] [PubMed] [Google Scholar]
- 5.Tripathi S, Kiran K, Kamala BK. Relationship between obesity and dental in children - A preliminary study. J Int Oral Health. 2010;2:65–72. [Google Scholar]
- 6.Caufield PW, Li Y, Dasanayake A. Dental caries: An infectious and transmissible disease. Compend Contin Educ Dent. 2005;26:10–6. [PubMed] [Google Scholar]
- 7.Jamelli SR, Rodrigues CS, de Lira PI. Nutritional status and prevalence of dental caries among 12-year-old children at public schools: A case-control study. Oral Health Prev Dent. 2010;8:77–84. [PubMed] [Google Scholar]
- 8.Diet, nutrition and prevention of chronic diseases. World Health Organ Tech Rep Ser. 2003;916:i–viii. 1–149. [PubMed] [Google Scholar]
- 9.Trikaliotis A, Boka V, Kotsanos N, Karagiannis V, Hassapidou M. Short communication: Dmfs and BMI in preschool Greek children. An epidemiological study. Eur Arch Paediatr Dent. 2011;12:176–8. doi: 10.1007/BF03262802. [DOI] [PubMed] [Google Scholar]
- 10.Sheiha A, Steele JG, Marcenes W, Finch S, Walls AW. The relationship between oral health status and Body Mass Index among older people: A national survey of older people in Great Britain. Br Dent J. 2002;192:703–6. doi: 10.1038/sj.bdj.4801461. [DOI] [PubMed] [Google Scholar]
- 11.World Health Organization. Oral health surveys- Basic methods. 4th ed. Geneva: WHO; 1987. [Google Scholar]
- 12.World Health Organization. Global Database on Body Mass Index. 2006. [Accessed May 30, 2014]. at http://apps.who.int/bmi/index .
- 13.Nizel AE. Nutrition in preventive dentistry: science and practice. 2nd ed. Philadelphia: Saunders; 1981. pp. 417–21. [Google Scholar]
- 14.Dudala SR, Arlappa N. An updated prasad's socio economic status classification for 2013. Int J Res Dev Health. 2013;1:26–8. [Google Scholar]
- 15.Lemle H. A weighty problem in American children: The overweight epidemic. Obesity San Diego: Lucent Books. 2000. [Accessed May 30, 2015]. at https://www.worldfoodprize.org/documents/filelibrary/images/youth_programs/research_papers/2005_ papers/AnthonyWayneHighSchoolHannaLemle_ F5FE5286630F5.pdf .
- 16.MacKenzie NR. Childhood obesity. Strategies for prevention. Pediatric Nurs. 2000;26:527–30. [PubMed] [Google Scholar]
- 17.Nguyen MD, Beresford SA, Drewnowski A. Trends in overweight by socio-economic status in Vietnam: 1992 to 2002. Public Health Nutr. 2007;10:115–21. doi: 10.1017/S1368980007224085. [DOI] [PubMed] [Google Scholar]
- 18.Gupta R, Rastogi P, Arora S. Low obesity and high under nutrition prevalence in lower socioeconomic status girls. Hum Ecol Spec Issue. 2006;14:65–70. [Google Scholar]
- 19.Marshall TA, Eichenberger-Gilmore JM, Broffitt BA, Warren JJ, Levy SM. Dental caries and childhood obesity: Roles of diet and socioeconomic status. Community Dent Oral Epidemiol. 2007;35:449–58. doi: 10.1111/j.1600-0528.2006.00353.x. [DOI] [PubMed] [Google Scholar]
- 20.Macek MD, Mitola DJ. Exploring the association between overweight and dental caries among us children. Pediatr Dent. 2006;28:375–80. [PubMed] [Google Scholar]
- 21.Yee R, McDonald N. Caries experience of 5-6-year-old and 12-13-year-old schoolchildren in central and western Nepal. Int Dent J. 2002;52:453–60. doi: 10.1111/j.1875-595x.2002.tb00642.x. [DOI] [PubMed] [Google Scholar]
- 22.Elias-Boneta AR, Crespo Kebler K, Gierbolini CC, Toro Vizcarrondo CE, Psoter WJ. Dental caries prevalence of twelve year olds in Puerto Rico. Community Dent Health. 2003;20:171–6. [PubMed] [Google Scholar]
- 23.Narang R, Saha S, Jagannath GV, S S, Kumari M, Mohd S. Nutritional status and caries experience among 12 to 15 years old school going children of Lucknow. J Int Dent Med Res. 2012;5:30–5. [Google Scholar]
- 24.Chu CH, Wang JH, Jan RH, Huang CH, Cheng CF. Association between health examination items and body mass index among school children in Hualien, Taiwan. BMC Public Health. 2013;13:975. doi: 10.1186/1471-2458-13-975. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.ur Rehman MM, Mahmood N, ur Rehman B. The Relationship of caries with oral hygiene status and extra-oral risk factors. J Ayub Med Coll Abbottabad. 2008;20:103–8. [PubMed] [Google Scholar]
- 26.Ferraro M, Vieira AR. Explaining gender differences in caries: A multifactorial approach to a multifactorial disease. Int J Dent. 2010;2010:649643. doi: 10.1155/2010/649643. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Khan AA, Jain SK, Shrivastav A. Prevalence of Dental Caries among the population of Gwalior (India) in Relation of Different Associated Factors. Eur J Dent. 2008;2:81–5. [PMC free article] [PubMed] [Google Scholar]
- 28.Bhardwaj VK, Sharma A. An epidemiological study of dental caries prevalence in mixed dentition among school children and its association with different variables in Shimla city. J Res Bede Athenaeum. 2011;2:1–5. [Google Scholar]
- 29.Naidu R, Prevatt I, Simeon D. The oral health and treatment needs of schoolchildren in Trinidad and Tobago: Findings of a national survey. Int J Paediatr Dent. 2006;16:412–8. doi: 10.1111/j.1365-263X.2006.00755.x. [DOI] [PubMed] [Google Scholar]
- 30.Sogi GM, Bhaskar DJ. Dental caries and oral hygiene status of school children in Davangere related to their socio-economic levels: An epidemiological study. J Indian Soc Pedo Prev Dent. 2002;20:152–7. [PubMed] [Google Scholar]
- 31.Roberts BP, Blinkhorn AS, Duxbury JT. The power of children over adults when obtaining sweet snacks. Int J Pediatric Dent. 2003;13:76–84. doi: 10.1046/j.1365-263x.2003.00434.x. [DOI] [PubMed] [Google Scholar]
- 32.Tuomi T. Pilot study on obesity in caries prediction. Community Dent Oral Epidemiol. 1989;17:289–91. doi: 10.1111/j.1600-0528.1989.tb00638.x. [DOI] [PubMed] [Google Scholar]
- 33.Larsson B, Johansson I, Hallmans G, Ericson T. Relationship between dental caries and risk factors for atherosclerosis in Swedish adolescents? Community Dent Oral Epidemiol. 1995;23:205–10. doi: 10.1111/j.1600-0528.1995.tb00232.x. [DOI] [PubMed] [Google Scholar]
- 34.Hilgers KK, Kinane DE, Scheetz JP. Association between childhood obesity and smooth-surface caries in posterior teeth: A preliminary study. Pediatr Dent. 2006;28:23–8. [PubMed] [Google Scholar]
- 35.Willershausen B, Moschos D, Azrak B, Blettner M. Correlation between oral health and body mass index (BMI) in 2071 primary school pupils. Eur J Med Res. 2007;12:295–9. [PubMed] [Google Scholar]
- 36.Kopycka-Kedzierawski DT, Auinger P, Billings RJ, Weitzman M. Caries status and overweight in 2- to 18-year-old US children: Findings from national surveys. Community Dent Oral Epidemiol. 2008;36:157–67. doi: 10.1111/j.1600-0528.2007.00384.x. [DOI] [PubMed] [Google Scholar]
- 37.Willershausen B, Haas G, Krummenauer F, Hohenfellner K. Relationship between high weight and caries frequency in german elementary school children. Eur J Med Res. 2004;9:400–4. [PubMed] [Google Scholar]