

Abstract
The aim of this article is to investigate a retrocaruncular approach for repairing medial orbital wall fractures. A total of 10 fresh cadaver orbits were dissected to investigate a transconjunctival approach to the orbit posterior to the caruncle. Medical records of consecutive patients with medial orbital wall fractures repaired via a retrocaruncular incision at Wilmer Eye Institute over a 10-year period were retrospectively reviewed. The study was approved by the Johns Hopkins Medical Institution's Institutional Review Board. Feasibility of this approach was clearly demonstrated on all cadavers. Horner muscle was observed to be directly attached to the caruncle and remained undisturbed throughout the retrocaruncular approach. For each of the 174 patients reviewed, this approach allowed successful access to the fracture and proper implant placement. The origin of the inferior oblique muscle was divided in only 19 patients. Sutures were not used for conjunctival incision closure in any patient. For 120 patients who underwent acute repair, the percentage with enophthalmos (≥ 2 mm) decreased from 34% preoperatively to 4% postoperatively; extraocular motility deficit decreased from 41 to 11%. Postoperative complications included recurrence of the preexisting retrobulbar hemorrhage, conjunctival granuloma, and temporary torsional diplopia, each in one patient. The retrocaruncular transconjunctival incision is an effective and safe approach for repairing medial orbital wall fractures with minimal complications. The retrocaruncular incision offers advantages over dividing the caruncle because Horner muscle is left undisturbed, and the incision heals well without suturing.
Keywords: transconjunctival, orbital fracture, enophthalmos
Various surgical approaches to the medial orbit, including transcutaneous, transcaruncular, and endoscopic, have been described. Lynch first popularized the direct approach through a superior nasal cutaneous incision.1 Although various modifications of the original Lynch incision were designed in an attempt to minimize the potential scar problems, this concern has continued to limit its popularity.2 3 4 5 To avoid a cutaneous incision while still providing adequate intraoperative visualization, various transnasal endoscope-assisted approaches have also been investigated.6 7 8 9 10 However, these transnasal techniques require expert endoscopic skills, which are usually more time-consuming, and depend on indirect fracture reduction.
A transcaruncular approach has been reported to allow direct binocular visualization of the medial orbital wall for accurate fracture definition and direct implantation.11 12 13 We initially adopted this technique for medial orbital fractures with or without other facial bone fractures. Later, we modified this technique by placing the incision more laterally, between the caruncle and the plica semilunaris. This incision, which falls naturally in the indentation between the caruncle and the plica, heals without suturing and leaves a hidden scar. The purpose of this study is to describe the results of repairing medial orbital wall fractures with this technique in a series of patients. An anatomical study on fresh cadaver orbits was also performed for an in depth understanding of this surgical approach.
Methods
Anatomical Study
A total of 10 orbits of fresh cadavers were dissected to define the anatomy associated with our surgical procedures (Fig. 1).
Fig. 1.
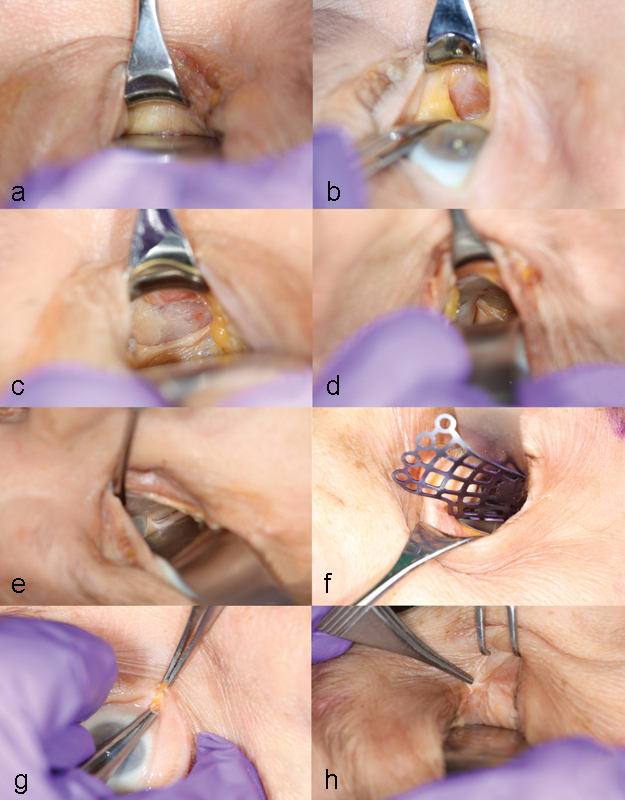
Cadaveric dissection illustrating the retrocaruncular approach to the medial orbit (looking toward the medial canthus). (a) The caruncle is retracted and protected with a Desmarres retractor and the globe protected with a malleable retractor. (b) After the retrocaruncular conjunctival incision, Horner muscle can be identified and left undisturbed. (c) Periosteum is incised just posterior to Horner muscle, and the bony medial orbital wall is visualized. (d) The anterior ethmoidal neurovascular bundle usually needs to be divided to expose the entire medial wall. (e) The posterior neurovascular bundle. (f) A small-sized prefabricated titanium plate is inserted into the orbit through an inferior fornix incision, which has been extended from the retroconjunctival incision. (g) Division of the caruncle in the transcaruncular approach. (h) The divided caruncle showing Horner muscle directly attached to the caruncle.
Clinical Study
A retrospective medical record review was performed for outcomes and complications in a series of consecutive patients with medial orbital wall fractures operated on by two of the authors (S.L.M. and M.P.G.) between August 2000 and November 2010 at the Wilmer Eye Institute. The study was approved by the Johns Hopkins Medical Institution's Institutional Review Board (NA_00032454). Surgeries were performed via a retrocaruncular incision as described below. Data extracted from the medical records included patient demographics, etiology of the trauma, concurrent ocular injuries, concomitant facial bone injuries, visual acuity, globe projection, ocular motility, and surgical complications. The patients were classified into one of three groups based on their previous surgical history: Group 1—patients without previous history of orbital surgery who underwent surgery within 4 weeks of injury (acute repair); Group 2—patients who underwent surgery > 4 weeks of injury (late repair); or Group 3—patients with a history of previous orbital surgery (secondary repair). Outcome measures for this study were the presence of residual clinically significant enophthalmos (≥ 2 mm) and either limitation of extraocular motility (EOM) on exam or complaint of diplopia in any gaze (EOM deficit). In addition, the presence of ocular surface complications, including keratopathy, symblepharon, and conjunctival granuloma were noted. The operative notes were reviewed or type of implant used, and whether or not the inferior oblique (IO) was divided or disinserted at its origin. All available computed tomographic (CT) scans were assessed for the evaluation of the orbital contour pre and postoperatively. Patients treated with enucleation as a result of concurrent ocular injuries were excluded because of the difficulty in assessing the outcome measures defined in this study.
Operative Technique
All surgeries were performed under general anesthesia. The nasal aspects of the upper and lower eyelids were retracted to expose the caruncle. A small malleable retractor was used to protect the globe while a lacrimal rake was used to protect the caruncle. A 12 mm vertical conjunctival incision was made between the caruncle and the plica semilunaris with Bovie electrocautery using a Colorado needle. A hypovascular plane posterior to the surface of Horner muscle was subsequently defined with careful blunt dissection down to the bone posterior to the lacrimal crest. The periorbita was incised posterior to Horner muscle and a subperiosteal dissection was performed to expose the fracture site in its entirety. The anterior ethmoidal neurovascular bundle was typically visualized, although it had frequently been injured by the original trauma. Bipolar electrocautery was used before division of the anterior ethmoid artery. Once the perimeter of the fracture and stable bone edges were defined, a suitably sized BARRIER MEDPOR sheet (Stryker, Kalamazoo, MI), BARRIER MEDPOR TITAN sheet (Stryker, Kalamazoo, MI), a titanium MatrixMIDFACE Preformed Orbital Plate (Synthes, West Chester, PA), or SupraFOIL (S. Jackson, Alexandria, VA) was shaped to cover the defect in its entirety. After the implant was confirmed, properly placed, and the force duction test was found to be negative, one or two miniscrews were placed to stabilize the implant in place if necessary. MEDPOR and MEDPOR TITAN plates were usually left unsecured. If an orbital floor fractures was also present, the medial transconjunctival incision was extended to connect with a retroseptal inferior transconjunctival incision to gain access to the orbital floor. Upon completion of surgery, a fenestrated drain was placed into the orbit and a traction suture from lower eyelid was taped to the forehead overnight. All conjunctival incisions were left unsutured.
Results
Anatomic Study
After the caruncle was retracted by a Desmarres retractor and the globe was protected by a malleable retractor, an incision was made in conjunctival indentation between the caruncle and plica semilunaris with a scalpel blade (Fig. 1a). The dissection was continued with blunt Steven tenotomy scissors to the level of bone as previously described.11 12 13 Horner muscle was identified in all dissections and protected anterior to the incision (Fig. 1b). The periosteum was incised immediately posterior to Horner muscle (Fig. 1c), and a wide subperiosteal dissection was performed. The important anatomical structures and surgical landmarks, including Horner muscle, the anterior and posterior ethmoidal neurovascular bundles (Fig. 1d, e), and the inferonasal orbital strut were all demonstrated. Horner muscle was clearly identified and undisturbed throughout the dissection in all cases. Using a 12 mm incision, the entire medial wall was easily visualized without the aid of an endoscope. The insertion of an orbital implant was feasible even for a small-sized, preformed, titanium orbital implant, without disinsertion of the IO (Fig. 1f). To compare our approach directly to the traditional, transcaruncular approach, a separate cadaver orbit was dissected, starting with division of the caruncle (Fig. 1g), and Horner muscle could be seen directly attached to the caruncle (Fig. 1h).
Clinical Study
A total of 174 individuals were included in the study, 124 males and 50 females. The median patient age was 31 years (range, 7–90 years). All the patients had history of a blunt orbital trauma from either assault in 83 patients (48%), fall in 21 patients (12%), sports in 29 patients (17%), motor vehicle accident in 24 patients (14%), gunshot wound in 3 patients (2%), and other mechanisms in 14 patients (8%). The median time interval from the time of injury to primary repair for the Group 1 patients was10 days and for the Group 2 patients was 90 days. The median time to secondary repair for the Group 3 patients was 300 days.
Of the 174 patients, 33 (19%) had pure medial internal orbital wall fracture and 141 patients (81%) had other concomitant facial fractures, which included orbital floor fractures (137 patients), fractures involving zygomaticomaxillary complex (21 patients), fractures involving nasoethmoidal complex (15 patients), mandibular fracture (1 patient), and orbital roof fracture (1 patient). The most common concurrent ocular injuries were commotio retinae (27 patients) and eyelid laceration (27 patients).
In 19 patients, the IO muscle was either divided at its origin (two patients) or disinserted subperiosteally at its origin to facilitate two-walled implant placement. In the two patients in whom the IO was divided, the muscle was later sutured back to its origin after implant placement; in the other 17 patients, the IO was not surgically reattached. The implants used to repair the medial wall fracture included BARRIER MEDPOR or BARRIER MEDPOR TITAN in 98 patients (56%), a titanium MatrixMIDFACE Preformed Orbital Plate in 73 patients (42%), and a SupraFOIL implant in 3 patients (2%).
The main outcome measures are listed in Table 1. In Group 1 patients, clinically significant enophthalmos (≥ 2 mm) improved from 34 to 4%, in Group 2 from 73 to 21%, and in Group 3 from 92 to 32% of patients. Likewise, in Group 1 patients, EOM improved from 41 to 11%, in Group 2 from 34 to 14%, and in Group 3 from 44 to 36% of patients. One Group 1 patient, one Group 2 patient, and five Group 3 patients subsequently underwent strabismus surgery for diplopia. Postoperative CT scans were re-reviewed for these patients and in no case could the EOM deficit be attributed to implant misplacement. One of the two patients in whom the IO was divided and sutured experienced, temporary torsional diplopia compatible with an IO palsy, which resolved by his last follow-up.
Table 1. Outcomes of medial orbital wall fracture repair by the retrocaruncular approach.
| Enophthalmos (≥ 2 mm) | EOM deficit | ||||
|---|---|---|---|---|---|
| Group | No. | Preop | Postop | Preop | Postop |
| Group 1, acute repair | 120 | 41 | 5 | 49 | 13 |
| Group 2, delayed repair | 29 | 21 | 6 | 10 | 4 |
| Group 3, secondary repair | 25 | 23 | 8 | 11 | 9 |
Abbreviations: EOM, extraocular ocular motility; preop, preoperative; postop, postoperative.
Postoperatively, no patient was noted to have decreased visual acuity. One patient had recurrence of a preexisting retrobulbar hemorrhage from the original trauma, which was subsequently treated by exploration of the orbit, removal of the implant, drainage of the blood, and subsequent replacement of the orbital implant, without permanent sequelae. A pyogenic granuloma developed at the conjunctival incision site in one patient, which was excised and did not recur. After review of postoperative CT scans, all implants were felt to be in good position, and no implant was repositioned or revised.
Discussion
Although various approaches to the medial wall have been described, the isolated transcaruncular approach has continued to gain popularity since its introduction more than 10 years ago.13 In this study, which to our knowledge is the largest review of transconjunctival fracture repair, we show that a retrocaruncular approach gives the same excellent access as the transcaruncular approach but offers a few additional advantages. Specifically, the retrocaruncular approach uses an incision position that does not disturb the attachments of Horner muscle to the caruncle, and creates an incision that heals without suturing and is hidden in the indentation between the plica semilunaris and the caruncle.
The transcaruncular approach was developed to avoid the obvious scar from a Lynch incision and was first described as direct conjunctival approach to the medial orbit in 1968.14 Magnus et al later reported a case in which the medial orbit was accessed via the space underneath a fornix-based conjunctival flap.15 More than 25 years later, as an approach to the medial orbit for both orbital trauma repair and decompression surgery, the transcaruncular approach, consisting of an inferior transconjunctival incision extending medially and superiorly across the caruncle was described.11 16 The divided caruncle was always repaired by suturing,11 13 16 and the caruncular incision was felt to provide “a landmark to align the closure.”12 In the vast majority of patients described, the origin of the IO muscle was divided for access and subsequently repaired at the end of the surgery.11 13 The transcaruncular approach, in which the caruncle and the IO were divided and subsequently repaired, was later adopted by many surgeons as the preferred approach for medial wall fractures.17 18 19 20 21
In our modification of the medial transconjunctival incision, the retrocaruncular approach, the incision is made lateral to the caruncle. Avoiding division of the caruncle has several advantages. In our anatomical dissection and those of others, Horner muscle is noted to directly fixate the caruncle to the posterior lacrimal crest22; therefore, division of the caruncle runs the risk of injuring Horner muscle, which helps to support the medial eyelid, and of causing additional intraoperative bleeding if Horner muscle is disturbed. Furthermore, a portion of the lower eyelid retractors attach to the caruncle, and Kakizaki and Valenzuela have observed that the lateral portion of the caruncle can shift inferolaterally after being divided in a transcaruncular approach to the medial orbit.23 Part of the caruncle derives from the skin embryologically.24 Performing a medial orbitotomy through the caruncle and extending into the upper and lower conjunctiva crosses two different tissue types, and may pose potential problems with wound healing. Some of these complications were described in those clinical studies about this approach11 20 and possibly could be minimized or avoided altogether by a retrocaruncular approach. Finally, in the retrocaruncular approach, the conjunctival incision is self-reapproximating and effectively heals without suturing, even if extended into a transconjunctival incision into the inferior fornix. In the immediate postoperative period, the unsutured incision provides a potential passageway for blood to egress.
In this study, a minority of patients (11%) underwent division or detachment of the IO to facilitate implant placement in contrast to other earlier studies.11 16 We were able to insert the small preformed anatomic plate in 60 of the 73 patients without disinserting the IO as shown in Fig. 1f. However, in our experience, when the large anatomic plate is used, disinsertion of the IO is typically required. Although none of the 17 patients in whom the IO was stripped along with the periosteum using a periosteal elevator, had torsional diplopia postoperatively, 1 of the 2 patients in whom the IO was divided at its origin and sutured back in place had temporary torsional diplopia. Perhaps, a subperiosteal disinsertion is preferable for postsurgical muscular function analogous to the trochlea, which successfully reattaches when stripped subperiosteally in an approach to the orbital roof.25 However, we still believe that disinsertion of the IO carries a small risk of causing diplopia as described in other studies11 20 and should be avoided if possible.
In conclusion, our retrocaruncular approach provides equally excellent access to the medial orbit as does the transcaruncular approach from which it was adapted. We believe that the incremental advantages over traditional caruncular division improves the traditional approach and should be considered for medial orbital wall fracture repairs, as well as other conditions requiring access to the medial orbit.
References
- 1.Lynch R. The technique of a radical frontal sinus operation which has given me the best results. Laryngoscope. 1921;31:1–5. [Google Scholar]
- 2.Burm J S, Oh S J. Direct local approach through a W-shaped incision in moderate or severe blowout fractures of the medial orbital wall. Plast Reconstr Surg. 2001;107(4):920–928. doi: 10.1097/00006534-200104010-00003. [DOI] [PubMed] [Google Scholar]
- 3.Esclamado R M, Cummings C W. Z-plasty modification of the Lynch incision. Laryngoscope. 1989;99(9):986–987. doi: 10.1288/00005537-198909000-00015. [DOI] [PubMed] [Google Scholar]
- 4.Katowitz J A, Welsh M G, Bersani T A. Lid crease approach for medial wall fracture repair. Ophthalmic Surg. 1987;18(4):288–290. [PubMed] [Google Scholar]
- 5.Arthurs B, Silverstone P, Della Rocca R C. Medial wall fractures. Adv Ophthalmic Plast Reconstr Surg. 1987;6:393–401. [PubMed] [Google Scholar]
- 6.Lee H M, Han S K, Chae S W, Hwang S J, Lee S H. Endoscopic endonasal reconstruction of blowout fractures of the medial orbital walls. Plast Reconstr Surg. 2002;109(3):872–876. doi: 10.1097/00006534-200203000-00006. [DOI] [PubMed] [Google Scholar]
- 7.Lee M J Kang Y S Yang J Y Lee D Y Chung Y Y Rohrich R J Endoscopic transnasal approach for the treatment of medial orbital blow-out fracture: a technique for controlling the fractured wall with a balloon catheter and Merocel Plast Reconstr Surg 20021102417–426., discussion 427–428 [DOI] [PubMed] [Google Scholar]
- 8.Naraghi M, Kashfi A. Endonasal endoscopic treatment of medial orbital wall fracture via rotational repositioning. Am J Otolaryngol. 2002;23(5):312–315. doi: 10.1053/ajot.2002.124197. [DOI] [PubMed] [Google Scholar]
- 9.Sanno T Tahara S Nomura T Hashikawa K Endoscopic endonasal reduction for blowout fracture of the medial orbital wall Plast Reconstr Surg 200311251228–1237., discussion 1238 [DOI] [PubMed] [Google Scholar]
- 10.Hinohira Y, Takahashi H, Komori M, Shiraishi A. Endoscopic endonasal management of medial orbital blowout fractures. Facial Plast Surg. 2009;25(1):17–22. doi: 10.1055/s-0028-1112227. [DOI] [PubMed] [Google Scholar]
- 11.Garcia G H, Goldberg R A, Shorr N. The transcaruncular approach in repair of orbital fractures: a retrospective study. J Craniomaxillofac Trauma. 1998;4(1):7–12. [PubMed] [Google Scholar]
- 12.Goldberg R A, Mancini R, Demer J L. The transcaruncular approach: surgical anatomy and technique. Arch Facial Plast Surg. 2007;9(6):443–447. doi: 10.1001/archfaci.9.6.443. [DOI] [PubMed] [Google Scholar]
- 13.Shorr N, Baylis H I, Goldberg R A, Perry J D. Transcaruncular approach to the medial orbit and orbital apex. Ophthalmology. 2000;107(8):1459–1463. doi: 10.1016/s0161-6420(00)00241-4. [DOI] [PubMed] [Google Scholar]
- 14.Edwards W C, Ridley R W. Blowout fracture of medial orbital wall. Am J Ophthalmol. 1968;65(2):248–249. doi: 10.1016/0002-9394(68)93596-4. [DOI] [PubMed] [Google Scholar]
- 15.Magnus W W, Castner D V, Schonder A A, Salz J J. A conjunctival approach to repair of fracture of medial wall of orbit: report of case. J Oral Surg. 1971;29(9):664–667. [PubMed] [Google Scholar]
- 16.Balch K, Goldberg R A, Green J, Shorr N. The transcaruncular approach to the medial orbit and the ethmoid sinus. A cosmetically superior option to the cutaneous (lynch) incision. Facial Plast Surg Clin North Am. 1998;6:71–77. [Google Scholar]
- 17.Edgin W A, Morgan-Marshall A, Fitzsimmons T D. Transcaruncular approach to medial orbital wall fractures. J Oral Maxillofac Surg. 2007;65(11):2345–2349. doi: 10.1016/j.joms.2006.06.270. [DOI] [PubMed] [Google Scholar]
- 18.Kim D W, Choi S R, Park S H, Koo S H. Versatile use of extended transconjunctival approach for orbital reconstruction. Ann Plast Surg. 2009;62(4):374–380. doi: 10.1097/SAP.0b013e3181855d27. [DOI] [PubMed] [Google Scholar]
- 19.Graham S M, Thomas R D, Carter K D, Nerad J A. The transcaruncular approach to the medial orbital wall. Laryngoscope. 2002;112(6):986–989. doi: 10.1097/00005537-200206000-00009. [DOI] [PubMed] [Google Scholar]
- 20.Malhotra R, Saleh G M, de Sousa J L, Sneddon K, Selva D. The transcaruncular approach to orbital fracture repair: ophthalmic sequelae. J Craniofac Surg. 2007;18(2):420–426. doi: 10.1097/scs.0b013e31803384c2. [DOI] [PubMed] [Google Scholar]
- 21.Baumann A, Ewers R. Transcaruncular approach for reconstruction of medial orbital wall fracture. Int J Oral Maxillofac Surg. 2000;29(4):264–267. [PubMed] [Google Scholar]
- 22.Kakizaki H, Zako M, Nakano T, Asamoto K, Miyaishi O, Iwaki M. Direct insertion of the medial rectus capsulopalpebral fascia to the tarsus. Ophthal Plast Reconstr Surg. 2008;24(2):126–130. doi: 10.1097/IOP.0b013e3181647cb2. [DOI] [PubMed] [Google Scholar]
- 23.Kakizaki H, Valenzuela A A. Lacrimal caruncle: continuation to the lower eyelid retractors. Ophthal Plast Reconstr Surg. 2011;27(3):198–200. doi: 10.1097/IOP.0b013e3181ed3573. [DOI] [PubMed] [Google Scholar]
- 24.Whitnall S. New York, NY: Robert E Krieger Publishing Company Inc; 1979. Anatomy of the human orbit and accessory organs of the vision. [Google Scholar]
- 25.Haug R H. Management of the trochlea of the superior oblique muscle in the repair of orbital roof trauma. J Oral Maxillofac Surg. 2000;58(6):602–606. doi: 10.1016/s0278-2391(00)90148-4. [DOI] [PubMed] [Google Scholar]