

Abstract
Background
Proximal row carpectomy and scaphoid-excision four-corner fusion are salvage procedures that relieve pain by removing arthritic joint surfaces. While numerous studies have examined how these procedures affect joint motion, few have examined how they influence muscle mechanical actions. This study examines whether muscle moment arms change after these procedures.
Methods
Moment arms of primary wrist muscles were measured in 8 cadaveric specimens using the tendon excursion method. In each specimen, moment arms were measured for two degrees of freedom (flexion-extension and radial-ulnar deviation) and three conditions (nonimpaired, scaphoid-excision four-corner fusion, and proximal row carpectomy). For each muscle and degree of freedom, moment arm versus joint angle curves for the three conditions were statistically compared.
Findings
Wrist salvage procedures significantly alter moment arms of the primary wrist muscles. Proximal row carpectomy primarily alters flexion-extension moment arms, while scaphoid-excision four-corner fusion primarily alters radial-ulnar deviation moment arms. Both procedures also alter the balance between agonist and antagonist wrist muscles. Following proximal row carpectomy, wrist extensors have smaller moment arms in extended postures. Following scaphoid-excision four-corner fusion, radial deviators have larger moment arms throughout radial-ulnar deviation.
Interpretation
Different moment arms indicate that different forces are required to complete the same tasks in nonimpaired and surgically altered wrists. The altered muscle moment arms likely contribute to post-operative impairments. Understanding how salvage procedures alter muscle mechanical actions is a critical first step toward identifying the cause of post-operative impairments and is necessary to develop effective interventions to augment deficient muscles and improve overall function.
Keywords: four-corner fusion, moment arm, proximal row carpectomy, wrist
1. Introduction
During wrist salvage procedures, some aspects of wrist and hand function are sacrificed to relieve osteoarthritic pain. Which salvage procedure has the best outcome is unclear. In particular, numerous studies have compared proximal row carpectomy (PRC) and scaphoid-excision four-corner fusion (SE4CF) [1–7]. Although several of these studies conclude that PRC preserves wrist range of motion, while SE4CF preserves grip strength [2, 3, 5], studies of long-term outcomes report that grip strength and wrist range of motion remain similarly and permanently impaired following both procedures [8–11].
Most scientific studies examining the mechanism responsible for impairments following PRC and SE4CF have focused on skeletal changes. For example, limits in wrist range of motion following SE4CF have been attributed to the fused position of the lunate; misaligning the lunate and capitate can bias the wrist toward either flexion or extension [12, 13]. Alternatively, limits in wrist range of motion following PRC have been attributed to impingement between carpal bones and the radial styloid [14] as well as differences in curvature between the surfaces of the lunate, capitate, and radius [15, 16].
How the geometric changes imposed by PRC and SE4CF influence muscle function is not fully understood. Because PRC shortens the carpus, it is assumed that muscles crossing the wrist operate at longer lengths following PRC, thereby reducing grip strength [17]. Yet, SE4CF does not involve shortening the carpus, and reduced grip strength is still reported [2]. To our knowledge, only one study has compared muscle actions following SE4CF and PRC [18]. This cadaver study demonstrated that to move nonimpaired, SE4CF, and PRC wrists through identical motions, different forces must be applied to the tendons of the primary wrist muscles. The fact that different tendon forces were required suggests that these procedures alter muscle moment arms. A muscle’s moment arm is the geometric factor that transforms the force produced by a muscle into torque about the joint’s axis of rotation, thereby determining how the joint moves. For example, when the extensor carpi radialis longus (ECRL) produces force, the wrist moves in extension and radial deviation; in contrast, the flexor carpi ulnaris (FCU) moves the wrist in the opposite directions (i.e., flexion and ulnar deviation). As demonstrated by Brand and Hollister [19], the opposing mechanical actions of these muscles are reflected in their moment arms. While the data from DeBottis et al. [18] suggests that the wrist muscle moment arms change following salvage procedures, their study did not quantify moment arms. To our knowledge, no studies report moment arms following SE4CF and only one study reports moment arms following PRC [20]. The significance of muscle moment arms at the wrist is well established by the works of Brand and Hollister [19] and Zajac [21], which describes the important role of moment arms in balancing antagonist muscle forces, dictating how muscles lenthen (or shorten) during joint movement, and determining how muscle oppose external loads at the hand. Thus, quantifying the differences in moment arms between nonimpaired and surgically altered wrists is critical for understanding why grip strength (i.e., the ability of muscles to produce external forces at the hand) is impaired following salvage procedures.
The purpose of this study was to measure and compare muscle moment arms in nonimpaired, SE4CF, and PRC wrists in a cadaveric model. We hypothesized that moment arms following salvage procedures would differ from the nonimpaired wrist. Additionally, because the geometric construction of the wrist joint is substantially different following PRC versus SE4CF, we expected that moment arms following each procedure would change in divergent ways.
2. Methods
The muscle moment arms of nonimpaired and surgically altered wrists were studied using eight unmatched, fresh-frozen cadaver upper extremities (four male; four female) amputated at the midhumeral level. The average age of donors at time of death was 62.3 (standard deviation, 8.9 years; range, forty-four to seventy-three). Radiographs were taken to exclude specimens with abnormalities.
Moment arms were estimated using the tendon excursion method [22], which defines moment arm as the derivative of tendon excursion with respect to joint angle. Tendon excursions were measured using rotary potentiometers (Model 3543s, Bourns Inc.); calibration of the devices within our experimental set-up indicates that, as implemented, they could resolve 0.08 mm excursions. Joint angles were calculated from the position of infrared targets, which were measured using a motion capture system (Optotrak Certus, Northern Digital Inc.) that has an accuracy of 0.1 mm.
2.1 Specimen Preparation
Each specimen was thawed at room temperature and prepped twenty-four hours prior to testing. Preparation included: exposing the tendons of five primary wrist muscles and securing infrared targets. The wrist muscles were exposed via three incisions. One dorsal incision exposed the tendons of the extensor carpi radialis brevis (ECRB), extensor carpi radialis longus (ECRL), and extensor carpi ulnaris (ECU). Two separate volar incisions exposed the tendons of the flexor carpi radialis (FCR) and flexor carpi ulnaris (FCU). The extensor retinaculum was preserved. Infrared targets were secured to the radius and third metacarpal via external fixators (Fig. 1, white arrows). A third infrared target on the base established a global reference frame (Fig. 1, indicated by white, outlined box). Each custom-made target had six infrared light emitting diodes that could be optically recorded and used to establish local coordinate frames. These targets were necessary for joint angle measurements.
Figure 1.
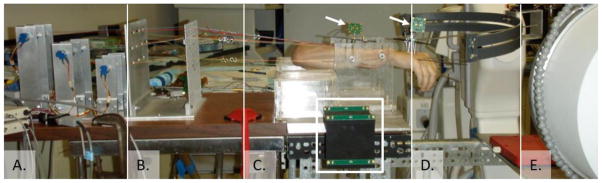
The full experimental set-up included (A) potentiometers to measure tendon excursion, (B) suture lines extended by nylon line to connect exposed tendons and potentiometers, (C) custom, acrylic jig to secure the specimen during testing, (D) planar track to guide wrist motion, and (E) C-arm to capture fluoroscopy while performing surgeries in the jig. Wrist joint angles were measured using a motion capture system (not shown), which measured the position of the global reference frame (enclosed by white rectangle) and two infrared targets secured to the third metacarpal and radius (marked by white arrows).
2.2 Experimental Testing
For a single specimen, all data were collected in a single day with the specimen at room temperature. During testing, each specimen was mounted in a custom, x-ray compatible acrylic jig by drilling two 4.76 mm threaded steel rods through the radius and ulna (Fig. 1C). The humerus was fixed to an acrylic support so that the elbow was at ninety degrees. The forearm was fixed in neutral pronation-supination. The wrist was not fixed. Wrist motions were guided by a single experimenter, who applied passive motion by moving a steel rod along a planar track (Fig. 1D); the steel rod was connected to the second metacarpal via an external fixators. This setup is similar to previous wrist moment arm studies [20, 23–26].
While the specimen was in the jig, each exposed tendon was connected to one of the rotary potentiometers (Fig. 1A). Specifically, four-0 braided nylon sutures were attached to each tendon immediately distal to the musculotendinous junction via a modified Kessler-Tajima stitch, and the suture ends were extended using FF-nylon line (Fig. 1B). Care was taken to ensure that each extended suture line aligned with the muscle-tendon line of action; retaining the muscle origins by not removing the humerus and proximal forearm facilitated this alignment. Tendon slack was eliminated by tensioning each line with 250 g weight. These weights were applied early during the experimental set-up in order to pre-tension the sutures, FF-nylon line, and tendons; thereby ensuring that they did not stretch during data collection.
Tendon excursion and joint angle data were collected during passive motion for two degrees of freedom (flexion-extension and radial-ulnar deviation), consistent with previous studies of the nonimpaired wrist [23]. For each specimen and surgical condition, tendon excursions for the five muscles and positions for the three infrared targets were recorded simultaneously using standard data acquisition software (TestPoint, Measurement Computing Corp.; Nortan, MA) on a single computer. Tendon excursions were sampled at 150 Hz; target positions were sampled at 30 Hz. To minimize the effects of noise and verify the reproducibility of the raw data, at least 30 trials were collected for each condition and degree of freedom; each trial lasted approximately 5 to 10 seconds.
2.3 Surgical Conditions
Three conditions were evaluated sequentially in all specimens: nonimpaired, SE4CF, and PRC. The nonimpaired condition represents the native state. SE4CF was performed by pinning the lunate, capitate, hamate, and triquetrum using two 1.59 mm Kirschner wires and excising the scaphoid. The first wire, directed distally to proximally through the second web space, pinned the lunate in a neutral position relative to the capitate. The second wire, directed distally to proximally through the fourth web space, pinned the lunate and hamate. The scaphoid was excised through a small dorsal incision; care was taken to neither interrupt the tendon lines of action nor sever the palmar ligaments. Placements of the Kirschner wires, neutral alignment of the lunate and capitate, and excision of the scaphoid were verified using fluoroscopy. PRC was performed by removing the Kirschner wires and excising the remaining proximal carpal bones. The lunate and triquetrum were excised by transversely extending the dorsal excision used to remove the scaphoid. The dorsal wrist capsule was imbricated and repaired to establish an interface between the radius and capitate. Alignment of the capitate and radius was verified using fluoroscopy. All surgeries and the associated fluoroscopy were performed while the specimen was in the jig (Fig. 1E).
2.4 Data Processing
Moment arms were calculated from the tendon excursion and joint angle data using numerical differentiation. Prior to numerical differentiation, the collected data were processed digitally using linear interpolation to provide tendon excursion data at half-degree increments. Tendon excursions were determined from the potentiometer outputs, which were proportional to the displacements of the tendons. Wrist joint angles were calculated from the recorded positions of the infrared targets. For each recorded motion, we calculated the three angles that fully describe the position of the third metacarpal relative to the radius. Based on these calculations, we report flexion-extension angles, defined as the angle between the long axis of the third metacarpal and the anterior-posterior plane of the radius, and radial-ulnar deviation angles, defined as the angle between the long axis of the third metacarpal and the medial-lateral plane of the radius.
Moment arm versus joint angle curves were obtained for each combination of specimen, muscle, surgical condition, and degree of freedom by fitting fourth order polynomials to all trials of collected data. This technique is consistent with previous literature [27]. Representative moment arm versus joint angle curves (Appendix) were then calculated by averaging the moment arm versus joint angle curves across all specimens (Fig. 2). Moment arm versus joint angle curves were analyzed for a limited range of wrist motion (40 extension to 40 flexion; 10 radial deviation to 30 ulnar deviation), which corresponds to the range of motion all specimens were able to achieve following the salvage procedures.
Figure 2.

Example of measured moment arm versus joint angle curve. Data shown is the nonimpaired (black), SE4CF (blue), and PRC (red) flexion-extension moment arm for the FCR. Lines are truncated at limits of recorded motion. Shaded regions represent one standard deviation, thereby depicting the variability in the data due to specimen. See Appendix for curves of other muscles and degrees of freedom.
2.5 Statistical Analysis
To test the hypothesis that moment arms following salvage procedures would be different than those of the nonimpaired wrist, a repeated measures analysis of variance (ANOVA) was used. The ANOVA tested the null hypothesis that moment arms for all three conditions (nonimpaired, SE4CF, and PRC) were equal, against the alternative hypothesis that moment arms of at least one condition were different. When the F-test of the ANOVA was significant, Tukey’s test for multiple comparisons was used to compare specific conditions; thereby testing the hypothesis that moment arms following PRC and SE4CF change in different ways. A significance level of p<0.05 was used for all tests.
All statistical analyses compared the moment arm curves that result from the data processing. Analyzing curves allowed us to statistically compare moment arms across all possible joint angles, instead of at discrete increments. To allow statistical comparison of curves, the ANOVA and multiple comparison tests were performed using mixed effects models, which can describe observed quantities (e.g., moment arms) in terms of multiple variables (e.g., surgical condition, joint angle, specimen). A distinct mixed effects model was defined for each muscle at each degree of freedom; each model represented the complete data set for that muscle and degree of freedom, prior to across-specimen averaging. In each model, condition and joint angle were fixed factors and specimen was a random factor.
To ensure sufficient sample size, a pre-hoc power analysis was conducted on the ANOVA test. The power analysis indicated that a power of greater than 0.80 would be achieved given 8 subjects, 3 groups, and an effect size of 1.96. This effect size indicates that the smallest detectable difference in mean moment arm magnitude is approximately 2 mm. The validity of the pre-hoc power analysis was verified by confirming that the effect sizes measured in this study were greater than or equal to those assumed from the literature [26].
2.6 Analysis of Wrist Balance
To understand the impact that changing individual muscle moment arms have on overall wrist function, we calculated ratios of moment arm magnitudes for antagonistic muscle groups. Specifically, we calculated the ratio between flexors and extensors by dividing the sum of the wrist flexor moment arm magnitudes (FCR, FCU) by the sum of the wrist extensor moment arm magnitudes (ECRL, ECRB, ECU) throughout the range of wrist motion. Similarly, the sum of the radial deviator moment arm magnitudes (ECRL, ECRB, FCR) was divided by the sum of the ulnar deviator moment arm magnitudes (ECU, FCU) to determine the ratio between radial and ulnar deviators. This analysis of wrist balance is similar to Lieber and Friden [28], who calculated torque ratios by multiplying moment arms by muscle force. During data analysis, we examined both moment arm ratios and torque ratios, and both analyses supported the conclusions presented in this study. We chose to report moment arm ratios because they do not rely on assumptions regarding muscle force-generating capacity. Specifically, because there are no existing studies documenting wrist muscle architecture following PRC and SE4CF, torque ratios can only be calculated by hypothesizing about how each surgery alters muscle force-generating capacity; moment arm ratios can be calculated using only data explicitly measured in this study. A change in the moment arm ratio for a given surgery relative to that of the nonimpaired wrist indicates how the combined changes to each individual wrist muscle’s moment arms impart systematic changes to the wrist.
3. Results
Salvage procedures alter moment arms of the primary wrist muscles (Fig. 3). The effect of condition was significant for either flexion-extension or radial-ulnar deviation moment arms for 4 of 5 primary wrist muscles (Table 1). No significant differences in moment arms for either degree of freedom were observed for FCU. In addition, FCU was the only muscle for which the measured effect size was smaller than that assumed in the pre-hoc power analysis. If PRC or SE4CF do impose changes to FCU moment arms, our study design suggests these changes would be less than 2 mm.
Figure 3.

Flexion-extension moment arms plotted as a function of radial-ulnar deviation moment arms when the wrist is in a neutral position. The moment arms measured in the nonimpaired wrist (black) is compared to those measured following (A) PRC (red) and (B) SE4CF (blue). Positive moment arms indicate extension and ulnar deviation; negative moment arms indicate flexion and radial deviation. Error bars represent one standard deviation.
Table 1.
Results of ANOVA: Do Salvage Procedures Alter Wrist Moment Arms?#
| Muscle | Flexion-Extension | Radial-Ulnar Deviation |
|---|---|---|
| FCR | p < 0.001* | p < 0.001* |
| FCU | p = 0.53 | p = 0.48 |
| ECRB | p < 0.001* | p = 0.01* |
| ECRL | p = 0.11 | p < 0.001* |
| ECU | p < 0.001* | p < 0.001* |
Two mixed effects models were derived per muscle, one for flexion-extension and one for radial-ulnar deviation. For each muscle and degree of freedom, the p-values of the ANOVA are presented. P-values < 0.05 (bolded with asterisks) indicate that the moment arm curves were significantly different for at least one condition (nonimpaired, SE4CF, PRC) for the given muscle and degree of freedom. For complete data set of moment arm versus joint angle curves, please refer to the Appendix.
The data indicate that PRC primarily alters flexion-extension moment arms, while SE4CF primarily alters radial-ulnar deviation moment arms (Table 2). Relative to the nonimpaired wrist, three muscles demonstrated significant changes in flexion-extension moment arms following PRC, compared to zero muscles following SE4CF. In contrast, for radial-ulnar deviation, only one muscle demonstrated significant changes in moment arm following PRC, compared to four muscles following SE4CF.
Table 2.
Results of Multiple Comparisons: Do SE4CF and PRC Alter Moment Arms Differently?#
| Muscle | Flexion-Extension | Deviation | ||
|---|---|---|---|---|
| SE4CF | PRC | SE4CF | PRC | |
| FCR | p = 0.302 | p < 0.001* | p < 0.001* | p = 0.949 |
| FCU | - | - | - | - |
| ECRB | p = 0.161 | p = 0.040* | p = 0.015* | p = 0.808 |
| ECRL | - | - | p = 0.003* | p = 0.207 |
| ECU | p = 0.616 | p < 0.001* | p < 0.001* | p < 0.001* |
| Total: | 0 | 3 | 4 | 1 |
For each muscle and degree of freedom for which the F-test of the ANOVA was significant, p-values of the multiple comparisons are presented. P-values < 0.05 (bolded with asterisks) indicate that the moment arm curves were significantly different than the nonimpaired wrist for the given surgery, muscle and degree of freedom. Muscles for which multiple comparisons were not performed (F-test of the ANOVA was not significant, as indicated in Table 1) marked by gray shading. For complete data set of moment arm versus joint angle curves, please refer to the Appendix.
The ratios of moment arms for antagonistic muscle groups demonstrate that both PRC and SE4CF alter the balance between the mechanical actions of the primary wrist muscles. PRC changes the balance between the moment arms of the wrist extensors and flexors. In the nonimpaired wrist, the sum of the wrist extensor moment arms is approximately equal to the sum of the wrist flexor moment arms throughout the functional range of wrist motion (cf., Fig. 4A, black line, ratio approximately equal to 1). Following PRC, the specimens demonstrated a bias toward flexion in extended wrist postures (cf., Fig. 4A, red line, ratio greater than 1 for negative joint angles). This flexion bias is caused by the decrease in ECRB and ECU extension moment arms (c.f., Fig. 4B, percent change in ECRB and ECU moment arms is negative for joint angles less than 0 degrees). In contrast, SE4CF substantially alters the balance between the moment arms of the radial and ulnar deviators. In the nonimpaired wrist, the sum of the radial deviator moment arms is approximately equal to the sum of the ulnar deviator moment arms (Fig. 5A, black line, ratio approximately equal to 1). Following SE4CF, the specimens demonstrated a bias toward radial deviation throughout the range of motion (cf., 5A, blue line, ratio greater than 1 for joint angles between −10 and 20 degrees). This radial deviation bias is caused by an increase in radial-ulnar deviation moment arms for all three radial deviators (FCR, ECRL, ECRB) and a decrease in radial-ulnar deviation moment arm for ECU (Fig. 5B).
Figure 4.

Comparison of flexion-extension moment arms for the nonimpaired (black) and PRC (red) wrists. (A) Ratio between the sum of the moment arms of the primary wrist flexors and the sum of the moment arms of the primary wrist extensors plotted as a function of joint angle. Solid line indicates the average ratio across all specimens; shaded area represents the 95 percent confidence interval about the average. (B) Percent change in individual flexion moment arms for the primary wrist muscles in the PRC wrist relative to the nonimpaired wrist. Bars to the left of the dashed line indicate average percent change for wrist extension (joint angles between −35 to 0 degrees); bars to the right indicate average percent change for wrist flexion (joint angles between 0 to 35 degrees). Filled bars indicate muscles with statistically significant changes in moment arm, zero percent represents no change from the nonimpaired condition, and error bars represent one standard deviation.
Figure 5.

Comparison of radial-ulnar deviation moment arms for the nonimpaired (black) and SE4CF (blue) wrists. (A) Ratio between the sum of the moment arms of the radial deviators and the sum of the moment arms of the ulnar deviators plotted as a function of joint angle. Solid line indicates the average ratio across all specimens; shaded area represents the 95 percent confidence interval about the average. (B) Percent change in individual deviation moment arms for the primary wrist muscles in the SE4CF wrist relative to the nonimpaired wrist. Bars to the left of the dashed line indicate average percent change for radial deviation (joint angles between −10 to 0 degrees); bars to the right indicate average percent change for ulnar deviation (joint angles between 0 to 25 degrees). Filled bars indicate muscles with statistically significant changes in moment arm, zero percent represents no change from the nonimpaired condition, and error bars represent one standard deviation.
4. Discussion
The present study demonstrates that a critical difference between PRC and SE4CF is how they influence the mechanical actions of individual muscles crossing the wrist. Specifically, PRC alters muscle actions for flexion-extension, while SE4CF alters them for radial-ulnar deviation. Despite the fact that PRC and SE4CF have been compared in numerous studies [5], we are unaware of any studies that highlight differences in how these procedures influence the mechanics of flexion-extension compared to radial-ulnar deviation. Our results suggests that post-operative impairments in function following PRC and SE4CF would be better understood by developing clinical assessments to specifically discriminate changes in wrist strength across flexion-extension versus radial-ulnar deviation.
By changing wrist balance, PRC and SE4CF alter how the wrist muscles must function. For example, the flexion bias imposed by PRC (cf., Fig. 4A, red curve, ratio greater than 1 for negative joint angles) influences the forces that the wrist muscles must produce during wrist extension, a posture required for most activities of daily living. Even without considering muscle force-generating capacity, following PRC, the net mechanical actions of the flexors overpower those of the extensors during wrist extension (i.e., to match the nonimpaired condition, the wrist extensors have to generate more force or the flexors have to generate less force in extended postures following PRC). The need to compensate for these altered force-generating requirements may contribute to weakness following PRC.
In contrast, SE4CF imposes a radial deviation bias (cf., Fig. 5A, blue line greater than 1 between −10 and 20 degrees). This suggests that the net mechanical actions of the radial deviators overpower those of the ulnar deviators following SE4CF (i.e., to match the nonimpaired condition, the radial deviators need to generate less force or the ulnar deviators more force in all postures following SE4CF). Altering radial-ulnar deviation moment arms without a comparable alteration to flexion-extension moment arms will affect the ability of muscles to execute movements that require combined flexion-extension and radial-ulnar deviation (e.g., dart thrower’s motion, power grip). Functional impairments following SE4CF may reflect the inability of wrist muscles to generate forces that efficiently produce combined flexion-extension and radial-ulnar deviation motion.
Even though long-term clinical studies report similar impairments following PRC and SE4CF [8, 11], this study suggests that different biomechanical mechanisms (i.e., flexion bias following PRC versus radial deviation bias following SE4CF) are associated with those impairments. The conclusion of our study is consistent with the work of DeBottis et al. [18] that demonstrated different muscle forces are required to generate the same wrist motion following PRC and SE4CF. Thus, results from more than one current anatomical study highlight the possibility that different rehabilitation strategies may be necessary to optimize hand function following these two salvage procedures. Notably, the results from both anatomical studies are most directly related to wrist strength, a measure that is not commonly assessed clinically. Given that there is a complex relationship between the degrees of freedom of the wrist, wrist strength, and functional outcomes, further study is needed assessing both wrist strength and hand function together in human subjects following salvage procedures to fully translate these anatomical findings to clinical recommendations.
Only one previous study has examined moment arms following PRC [20]; to our knowledge, moment arms following SE4CF have not been measured previously. Both this study and that of Sobczak et al. [20] report significant changes in flexion-extension moment arms following PRC. Importantly, for three muscles (ECRB, ECU, FCR), the changes observed in moment arms following PRC were particularly comparable (cf., Fig. 6A, the gray arrows connecting black (nonimpaired) and red (PRC) symbols point in the same direction for these three muscles in both studies). While the directions of the changes in moment arms following PRC were similar across these two studies, the magnitudes of the changes were variable (Fig. 6). This variability could reflect both differences in experimental technique (e.g., the two studies used different muscle loading and different ranges of motion used to calculate the average moment arm) and surgical technique (e.g., longitudinal versus transverse incision). Given the paucity of data characterizing how the mechanical actions of muscles change following surgical salvage procedures, it is difficult to interpret the clinical significance of the variability observed across these two studies. In contrast, at least six studies from different investigators have quantified moment arms for the nonimpaired wrist [19, 20, 23–26]. For all muscles examined, the nonimpaired moment arms in this study fell within two standard deviations of the average data reported among these six studies (Fig. 7).
Figure 6.

Comparison of how moment arms change from the nonimpaired (black) to PRC (red) wrists as reported in this study (filled circles) and as reported by Sobczak et al. [20] (open squares). Flexion-extension moment arms are plotted as a function of deviation moment arms. To allow direct comparison, values are moment arms averaged across all joint angles. Arrows highlight similarities across studies in how moment arms change between the nonimpaired and PRC wrists.
Figure 7.

Nonimpaired moment arms measured in this study (black, filled circles) compared to those reported in the literature; flexion-extension moment arms are plotted as a function of deviation moment arms. The values are measured moment arms averaged across joint angles. Ellipses are centered at the average of previously reported moment arms and enclose one standard deviation of those previously reported averages [19, 20, 22, 24, 25, 26]. Error bars on data measured in this study represent one standard deviation.
This study demonstrates significant differences in how PRC and SE4CF alter flexion-extension versus radial-ulnar deviation moment arms and suggests that these procedures substantially alter wrist balance. Therefore, the biomechanical changes imposed by PRC and SE4CF to the primary wrist muscles should be considered when evaluating these procedures, recommending therapies, or implementing further surgical interventions.
Supplementary Material
HIGHLIGHTS.
We measure moment arms of the five primary wrist muscles for three conditions.
We compare nonimpaired, proximal row carpectomy, scaphoid-excision 4-corner fusion.
Proximal row carpectomy primarily alters flexion-extension moment arms.
Scaphoid-excision four-corner fusion primarily alters deviation moment arms.
Assessments to discriminate wrist strength among these conditions are needed.
Acknowledgments
This work was funded by NIH (F31 AG041627 and T32 HD007418) and the Searle Funds of the Chicago Community Trust. Medcure donated cadaveric specimens. We would like to thank Ajay Balaram, MD and Hilton Gottschalk, MD for assistance with specimen preparation and the collection of pilot data; Julia Lee, PhD and Denise Scholtens, PhD for helpful discussions regarding statistical methods; and Vikram Darbhe, MS and Andrew Lee for building the experimental set-up and assisting with experimental testing, performed at the Edward Hines Jr. VA Hospital.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Contributor Information
Jennifer A. Nichols, Email: jnichols@u.northwestern.edu.
Michael S. Bednar, Email: mbednar@lumc.edu.
Robert M. Havey, Email: Robert.Havey@va.gov.
Wendy M. Murray, Email: w-murray@northwestern.edu.
References
- 1.Bisneto EN, Freitas MC, Paula EJ, Mattar R, Jr, Zumiotti AV. Comparison between proximal row carpectomy and four-corner fusion for treating osteoarthrosis following carpal trauma: a prospective randomized study. Clinics (Sao Paulo) 2011;66(1):51–55. doi: 10.1590/S1807-59322011000100010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Cohen MS, Kozin SH. Degenerative arthritis of the wrist: proximal row carpectomy versus scaphoid excision and four-corner arthrodesis. J Hand Surg Am. 2001;26(1):94–104. doi: 10.1053/jhsu.2001.20160. [DOI] [PubMed] [Google Scholar]
- 3.Dacho AK, Baumeister S, Germann G, Sauerbier M. Comparison of proximal row carpectomy and midcarpal arthrodesis for the treatment of scaphoid nonunion advanced collapse (SNAC-wrist) and scapholunate advanced collapse (SLAC-wrist) in stage II. J Plast Reconstr Aesthet Surg. 2008;61(10):1210–1218. doi: 10.1016/j.bjps.2007.08.007. [DOI] [PubMed] [Google Scholar]
- 4.De Smet L, Degreef I, Robijns F, Truyen J, Deprez P. Salvage procedures for degenerative osteoarthritis of the wrist due to advanced carpal collapse. Acta Orthop Belg. 2006;72(5):535–540. [PubMed] [Google Scholar]
- 5.Mulford JS, Ceulemans LJ, Nam D, Axelrod TS. Proximal row carpectomy vs four corner fusion for scapholunate (Slac) or scaphoid nonunion advanced collapse (Snac) wrists: a systematic review of outcomes. J Hand Surg Eur Vol. 2009;34(2):256–263. doi: 10.1177/1753193408100954. [DOI] [PubMed] [Google Scholar]
- 6.Vanhove W, De Vil J, Van Seymortier P, Boone B, Verdonk R. Proximal row carpectomy versus four-corner arthrodesis as a treatment for SLAC (scapholunate advanced collapse) wrist. J Hand Surg Eur Vol. 2008;33(2):118–125. doi: 10.1177/1753193408087116. [DOI] [PubMed] [Google Scholar]
- 7.Wyrick JD, Stern PJ, Kiefhaber TR. Motion-preserving procedures in the treatment of scapholunate advanced collapse wrist: proximal row carpectomy versus four-corner arthrodesis. J Hand Surg Am. 1995;20(6):965–970. doi: 10.1016/S0363-5023(05)80144-3. [DOI] [PubMed] [Google Scholar]
- 8.Bain GI, Watts AC. The outcome of scaphoid excision and four-corner arthrodesis for advanced carpal collapse at a minimum of ten years. J Hand Surg Am. 2010;35(5):719–725. doi: 10.1016/j.jhsa.2010.01.025. [DOI] [PubMed] [Google Scholar]
- 9.DiDonna ML, Kiefhaber TR, Stern PJ. Proximal row carpectomy: study with a minimum of ten years of follow-up. J Bone Joint Surg Am. 2004;86-A(11):2359–2365. [PubMed] [Google Scholar]
- 10.Jebson PJ, Hayes EP, Engber WD. Proximal row carpectomy: a minimum 10-year follow-up study. J Hand Surg Am. 2003;28(4):561–569. doi: 10.1016/s0363-5023(03)00248-x. [DOI] [PubMed] [Google Scholar]
- 11.Richou J, Chuinard C, Moineau G, Hanouz N, Hu W, Le Nen D. Proximal row carpectomy: long-term results. Chir Main. 2010;29(1):10–15. doi: 10.1016/j.main.2009.10.003. [DOI] [PubMed] [Google Scholar]
- 12.De Carli P, Donndorff AG, Alfie VA, Boretto JG, Lopez Ovenza JM, Gallucci GL. Four-corner arthrodesis: influence of the position of the lunate on postoperative wrist motion: a cadaveric study. J Hand Surg Am. 2007;32(9):1356–1362. doi: 10.1016/j.jhsa.2007.08.004. [DOI] [PubMed] [Google Scholar]
- 13.Dvinskikh NA, Blankevoort L, Strackee SD, Grimbergen CA, Streekstra GJ. The effect of lunate position on range of motion after a four-corner arthrodesis: a biomechanical simulation study. J Biomech. 2011;44(7):1387–1392. doi: 10.1016/j.jbiomech.2010.12.025. [DOI] [PubMed] [Google Scholar]
- 14.Blankenhorn BD, Pfaeffle HJ, Tang P, Robertson D, Imbriglia J, Goitz RJ. Carpal kinematics after proximal row carpectomy. J Hand Surg Am. 2007;32(1):37–46. doi: 10.1016/j.jhsa.2006.10.014. [DOI] [PubMed] [Google Scholar]
- 15.Hawkins-Rivers S, Budoff JE, Ismaily SK, Noble PC, Haddad J. MRI study of the capitate, lunate, and lunate fossa with relevance to proximal row carpectomy. J Hand Surg Am. 2008;33(6):841–849. doi: 10.1016/j.jhsa.2008.02.021. [DOI] [PubMed] [Google Scholar]
- 16.Imbriglia JE, Broudy AS, Hagberg WC, McKernan D. Proximal row carpectomy: clinical evaluation. J Hand Surg Am. 1990;15(3):426–430. doi: 10.1016/0363-5023(90)90054-u. [DOI] [PubMed] [Google Scholar]
- 17.Nagelvoort RW, Kon M, Schuurman AH. Proximal row carpectomy: a worthwhile salvage procedure. Scand J Plast Reconstr Surg Hand Surg. 2002;36(5):289–299. doi: 10.1080/028443102320791842. [DOI] [PubMed] [Google Scholar]
- 18.Debottis DP, Werner FW, Sutton LG, Harley BJ. 4-corner arthrodesis and proximal row carpectomy: a biomechanical comparison of wrist motion and tendon forces. J Hand Surg Am. 2013;38(5):893–898. doi: 10.1016/j.jhsa.2013.01.033. [DOI] [PubMed] [Google Scholar]
- 19.Brand PW, Hollister AM. Clinical Mechanics of the Hand. St. Louis, MO: Mosby, Inc; 1999. [Google Scholar]
- 20.Sobczak S, Rotsaert P, Vancabeke M, Van Sint Jan S, Salvia P, Feipel V. Effects of proximal row carpectomy on wrist biomechanics: a cadaveric study. Clin Biomech (Bristol, Avon) 2011;26(7):718–724. doi: 10.1016/j.clinbiomech.2011.03.002. [DOI] [PubMed] [Google Scholar]
- 21.Zajac FE. How musculotendon architecture and joint geometry affect the capacity of muscles to move and exert force on objects: a review with application to arm and forearm tendon transfer design. J Hand Surg Am. 1992;17(5):799–804. doi: 10.1016/0363-5023(92)90445-u. [DOI] [PubMed] [Google Scholar]
- 22.An K, Ueba Y, Chao E, Conney W, Linscheid R. Tendon excursion and moment arms of index finger muscles. J Biomech. 1983;16(6):419–425. doi: 10.1016/0021-9290(83)90074-x. [DOI] [PubMed] [Google Scholar]
- 23.Horii E, An KN, Linscheid RL. Excursion of prime wrist tendons. J Hand Surg Am. 1993;18(1):83–90. doi: 10.1016/0363-5023(93)90250-7. [DOI] [PubMed] [Google Scholar]
- 24.LaRoque ES, Murray WM, Langley S, Hariri S, Levine BP, Ladd AL. Muscle moment arms in the first dorsal extensor compartment after radial malunion. A cadaver study. J Bone Joint Surg Am. 2008;90(9):1979–1987. doi: 10.2106/JBJS.G.01015. [DOI] [PubMed] [Google Scholar]
- 25.Loren GJ, Shoemaker SD, Burkholder TJ, Jacobson MD, Friden J, Lieber RL. Human wrist motors: biomechanical design and application to tendon transfers. J Biomech. 1996;29(3):331–342. doi: 10.1016/0021-9290(95)00055-0. [DOI] [PubMed] [Google Scholar]
- 26.Tang JB, Ryu J, Han JS, Omokawa S, Kish V, Wearden S. Biomechanical changes of the wrist flexor and extensor tendons following loss of scaphoid integrity. J Orthop Res. 1997;15(1):69–75. doi: 10.1002/jor.1100150111. [DOI] [PubMed] [Google Scholar]
- 27.Murray WM, Delp SL, Buchanan TS. Variation of muscle moment arms with elbow and forearm position. J Biomech. 1995;28(5):513–525. doi: 10.1016/0021-9290(94)00114-j. [DOI] [PubMed] [Google Scholar]
- 28.Lieber RL, Friden J. Musculoskeletal balance of the human wrist elucidated using intraoperative laser diffraction. J Electromyogr Kinesiol. 1998;8(2):93–100. doi: 10.1016/s1050-6411(97)00025-4. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.