

Abstract
Introduction:
There are no controlled studies dedicated to research of side effects of antidepressants. It is a well known fact that antidepressants reciprocally differ according to their type, intensity and frequency of appearance of certain side effects. For example, cardiovascular and anticholinergic effects are essential feature of the tricyclics whereas gastrointestinal and sexual side effects are registered during the use of selective serotonin reuptake inhibitors. Interruptions of therapy or irregular use of drugs because of the appearance of side effects are not rare. Serious side effects of drugs are the fourth cause of death in the USA.
Aim:
The aim of this study is the evaluation of appearance of side effects comparing three different groups of antidepressants: venlafaxine, amitriptyline and paroxetine.
Material and methods:
The study included 90 in-patients as well as outpatients of both sexes aged 18-65 who were treated for major depressive disorder at Psychiatric Clinic in Banjaluka. 30 patients were treated with amitriptyline 75-250 mg, 30 patients were treated with paroxetine 20-40 mg and 30 patients were treated with venlafaxine 75-300 mg. The selection of patients was done on the basis of diagnosis of major depressive disorder.
Results:
Most patients did not have serious side effects. The study confirmed high efficiency of the mentioned drugs as well as the fact that paroxetine causes a bit more side effects in comparison with two other antidepressants.
Keywords: depression, antidepressants, side effects of drugs
1. INTRODUCTION
Depression is the second ranked health problem in women and the fourth ranked one for the whole population. According to the assessments of the World Health Organization, depression will become the second ranked world health problem and the first ranked health problem in women by 2020 (1).
It is estimated that depression in Europe has not been treated enough, and different treatment options have not been applied enough (2). Researches from our country indicate that depression is usually not recognized, that is, not treated (3), which has high social and economic price.
It is a well known fact that antidepressants reciprocally differ according to their type, intensity and frequency of appearance of certain side effects. For example, cardiovascular and anticholinergic effects are essential feature of the tricyclics whereas gastrointestinal and sexual side effects are registered during the use of selective serotonin reuptake inhibitors. New researches indicate that the frequency of appearance of some side effects of new antidepressants, such as weight gain and sexual dysfunctions, in randomized controlled studies is probably underestimated (4). Interruptions of therapy or irregular use of drugs because of the appearance of side effects are not rare. Meta-analyses showed that rates of interruptions of therapy for tricyclic antidepressants are between 19 and 31%, and between 15 and 25% for selective serotonin reuptake inhibitors. It is important to know side effects of antidepressants because of the choice of drug as well as their influence on compliance during the acute phase of treatment as well as continuous and prophylactic therapy. Besides that, serious side effects of drugs are the fourth cause of death in the USA (5).
Side effects of the tricyclic antidepressants: cardiovascular side effects, anticholinergic effects, sedation, weight gain, neurological side effects (4, 6). Side effects of selective serotonin reuptake inhibitors: gastrointestinal side effects, activation syndrome, sexual side effects, neurological side effects, influence on body weight, serotonin syndrome (7, 8, 9, 10). Side effects of venlafaxine: gastrointestinal effects, activation/insomnia, sexual side effects as well as rise in arterial pressure (11).
2. AIM OF THE STUDY
The aim of the study is comparison of side effects of three groups of antidepressants – venlafaxine, paroxetine and amitriptyline in depression therapy.
3. MATERIAL AND METHODS
The study included 90 in-patients as well as outpatients of both sexes aged 18-65 who were treated for major depressive disorder at Psychiatric Clinic in Banjaluka. The disorder was defined according to MKB-10 criterion and diagnosed as F 32.2 (for major depressive episode).
The main criterion for including patients in the study was minimal score of 14 according to HAMD scale of 21questions (Hamilton Depression Rating Scale) and mark >2 according to HAMD item 1- depressive mood. The research was open. 30 patients were treated with amitriptyline 75-250 mg, 30 patients were treated with paroxetine 20-40 mg and 30 patients were treated with venlafaxine 75-300 mg. The selection of patients was done on the basis of diagnosis of major depressive disorder.
Every group was tested at the beginning of the therapy, after 30 days of treatment, after 12 weeks of treatment and after 6 months of treatment.
Every group of examinees follows patients’ initials, disease diagnosis, sex, age, education, employment, marital status, place of living.
4. RESULTS
The results presented on Table 1-3 and Figure 1-3 were obtained by this study.
Table 1.
Side effects during the first month

Table 2.
Side effects during three months

Table 3.
Side effects during six months

Figure 1.
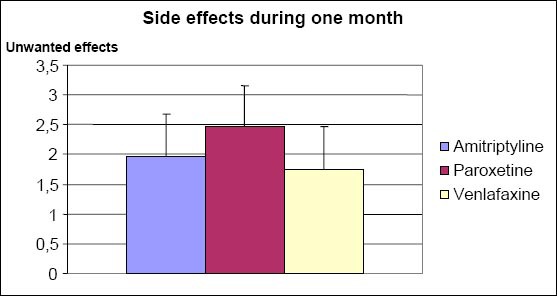
Side effects of drugs after one month
Figure 2.
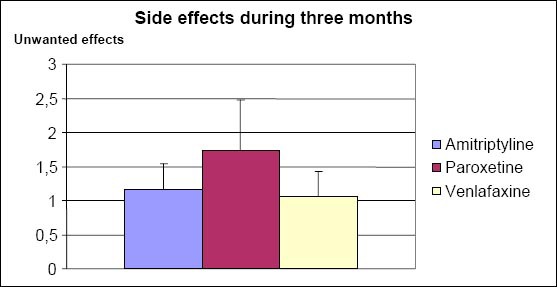
Side effects of drugs after three months
Figure 3.
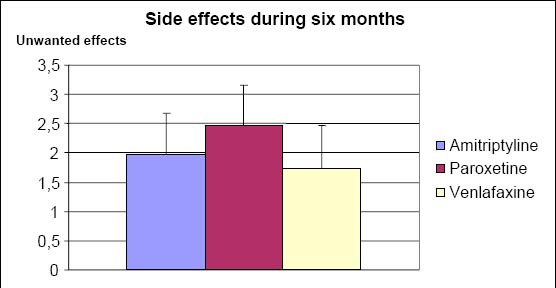
Side effects of drugs after six months
Kruskal-Wallis test shows that the differences of side effects among drugs during the first month are statistically important (p = 0,000). Paroxetine has the largest number of side effects.
Kruskal-Wallis test shows that the differences of side effects among drugs during the first three months are statistically important (p = 0,000). Paroxetine has the largest number of side effects.
Kruskal-Wallis test shows that the differences of side effects among drugs during the first six months are statistically important (p = 0,000). Paroxetine has the largest number of side effects in comparison with two other antidepressants.
5. DISCUSSION
There are no controlled studies dedicated to research of side effects of antidepressants which was the main reason of this research. The study explored three different groups of antidepressants in depression treatment. Majority of patients did not have any major side effects.
During a six-month treatment, it was proved that paroxetine had the largest number of side effects in comparison with two other antidepressants. Venlafaxine, a bicyclic antidepressant, inhibits re-uptake of noradrenaline and serotonin (as well as less amount of dopamine) without blocking andrenergic, serotonergic, cholinergic and histamine receptors. Basic antidepressant activity is based on mechanisms identical to mechanisms of activity of the classical tricyclics. There are not any known side effects of these drugs what was proved by this study.
When we choose an adequate antidepressant, a profile of side effects which influence use of medicine is important as well as co-operation of a patient. The purpose of clinical researches is the detection of efficient antidepressants with the profile of side effects which do not influence quality of patient’s life.
6. CONCLUSION
Comparing side effects of three different groups of antidepressants during first six months, it was found that the difference of side effects among drugs during the first six months is statistically important (p = 0,000). The study justified the aim of this research work in regard with comparison of side effects of three different groups of antidepressants. It confirmed that paroxetine has a bit more side effects in comparison with two other antidepressants.
Side effects of the three antidepressants in this research are mild and rare. They slightly more often accompany use of paroxetine in comparison with two other antidepressants.
Footnotes
CONFLICT OF INTEREST: NONE DECLARED
REFERENCES
- 1.Lam RW, Mok H. Depression, Oxford University Press, Lundbeck Institute; 2008. [Google Scholar]
- 2.Henriksson S, Asplund R, Boethius G, Hällström T, Isacsson G. Infrequent use of antidepressants in depressed individuals (an interview and prescription database study in a defined Swedish population 2001-2002. Eur Psychiatry. 2006;21:355–360. doi: 10.1016/j.eurpsy.2006.04.003. [DOI] [PubMed] [Google Scholar]
- 3.Lisulov R, Nedić A. Novi Sad: University of Novi Sad, Faculty of Medicine; 2006. Problems of diagnostics and treatment of depressive disorders in primary care institutions in Autonomous Region Vojvodina. [Google Scholar]
- 4.Kenedi SH, Lam RW, Cohen NL, Ravindran AV. Clinical guidelines for the treatment of depressive disorders. IV. Medications and other biological treatments. Can J Psychiatry. 200;46:38–58. [PubMed] [Google Scholar]
- 5.Lazarou J, Pomeranz BH, Corey PN. Incidence of adverse drug reactions in hospitalized patients: a meta-analysis of prospective studies. JAMA. 1998;279:1200–1205. doi: 10.1001/jama.279.15.1200. [DOI] [PubMed] [Google Scholar]
- 6.Garvey MJ, Tollefson GD. Occurrence of myoclonus in patients treated with cyclic antidepressants. Arch Gen Psychiatry. 1987;44:269–272. doi: 10.1001/archpsyc.1987.01800150081010. [DOI] [PubMed] [Google Scholar]
- 7.Daghty MJ, Lyle WM. Medications used to prevent migraine headaches and their potential ocular adverse effects. Optom Vis Sci. 1995;72:879–891. doi: 10.1097/00006324-199512000-00006. [DOI] [PubMed] [Google Scholar]
- 8.Frazer A. Antidepressants. J Clin Psychiatry. 1997;58:9–25. [PubMed] [Google Scholar]
- 9.Michelson D, Amsterdam JD, Quitkin FM, Reimherr FW, Rosenbaum JF, Zajecko J, et al. Changes in weight during a 1-year trial of fluoxetine. Am J Psychiatry. 1999;156:1170–1176. doi: 10.1176/ajp.156.8.1170. [DOI] [PubMed] [Google Scholar]
- 10.Walker PW, Cole JO, Gardner EA, Hughes AR, Johnston JA, Batey SR, et al. Improvement in fluoxetine-associated sexual dysfunction in patients switched to bupropion. J Clin Psychiatry. 1993;54:459–465. [PubMed] [Google Scholar]
- 11.Thase ME. Effects of venlafaxine on blood pressure: a meta-analysis of original data on 3744 depressed patients. J Clin Psychiatry. 1998;59:502–508. doi: 10.4088/jcp.v59n1002. [DOI] [PubMed] [Google Scholar]