

Abstract
Background:
The patients that are subjects to oral-surgical interventions produce large amounts of steroids in comparison with healthy patients which are not a subject to any dental intervention. The aim of research was to determine the level of stress hormone cortisol in serum, arterial blood pressure and arterial pulse, and to compare the effectiveness of the usage of lidocaine with adrenalin in comparison with lidocaine without adrenalin during the tooth extraction.
Patients and methods:
This clinical research includes patients with indication of tooth extraction divided in hypertensive and normotensive patients.
Results:
There is no important statistical distinction between groups, for the cortisol levels before, during and after tooth extraction regardless of the type of anesthetic used, while we registered higher values of systolic and diastolic values at hypertensive patients, regardless of the type of anesthetic
Conclusion:
There is significant systolic and diastolic blood pressure rise in both groups of patients hypertensive and normotensive patients, (regardless of anesthetic used with or without vasoconstrictor), who underwent tooth extraction. The special emphasize is attributed to hypertensive patients where these changes are more significant. As per cortisol level and pulse rate, our results indicate no significant statistical difference in between groups.
Keywords: stress, local anesthesia, cortisol, hypertensive patients
1. INTRODUCTION
Stress is defined as the body’s response to external factors or pressures. (American Institute of Stress). Stress factors are diverse and the pain as single agent is one of those, moreover stress intensifies the pain. (1-4). The first reaction of the human body to the stress is the alarm reaction, where impulses are transmitted to the brain through sensory pathways that furthermore stimulate adrenal cortex to produces cortisol and other glucocorticoids (2, 4). Apart from affecting the adrenal cortex, stress factors at the same time stimulate the sympathetic nervous system causing the reaction “fight” or “flight”, increasing the blood pressure and blood volume, reducing digestion due to the blood distribution from digestive tract to the muscles and other active organs and increasing the glucose concentration (3). The reaction of the adrenal stress related to tooth extraction is much greater than the stress that occurs during any other routine dental intervention (5, 6). Patients undergoing oral surgery interventions produce larger amounts of steroids compared with healthy patients who are not undergoing any dental intervention (1).
Special attention is addressed to hypertensive patients. Hypertensive systolic and diastolic pressure is with higher values in reference to the patient’s age. One adult with increased arterial pressure values over 135/85 mmHg in general, is considered as hypertensive (7).
2. PATIENTS AND METHODS
The research is carried out in the Oral Surgery Clinic in Prishtina Clinical University Stomatological Center, Kosovo. This prospective clinical study included patients with indication of teeth extraction divided into 2 groups: Group 1- normotensive patients (40 patients) and Group 2- hypertensive patients (40 patients). Group 1 and 2 were divided in further two subgroups. Patients in Subgroup 1 were treated with a local anesthetist lidocaine with adrenaline (anesthetic lidocaine 2 ml in a solution of 2% with 1: 100,000 adrenaline), while the patients of subgroup 2 were treated with local anesthetist lidocaine without adrenaline (2% without adrenaline in an amount of 2 ml was used). Each patient underwent a detailed anamnestic data and classification. Several samples of blood were taken, as follows:
-
♦
First blood sample is taken 30 minutes prior to administration of anesthesia;
-
♦
Second blood sample is taken during the intervention (i.e. extraction of tooth or debridement
-
♦
Third blood sample is taken 30 minutes after the intervention.
The blood samples are taken to determine the level of the stress derived from hormone cortisol using RIA method. Accumulated amount of blood in 2 ml of each sample (sample) was put in a test tube. Centrifugation of blood is carried out to separate serum from plasma. Samples are stored at -18C and analyzed in Endocrinology laboratories at the Clinical Institute of University Clinical Center of Kosova. The obtained results for cortisol level were analyzed by standard curves. The results are calculated using semi-logarithm curve with B / TB / B0 (%) in the vertical axis and the concentration of cortisol standard horizontal axis (nmol / L). Converted the results from nmol / L (nM) in mg / L were made by multiplying the coefficient of 0.326. To analyze data at the same time we performed quality control data, so that the control samples are used for security quality results. These samples are made in the same way as research samples and analyzed using the same statistical methods. Normal values of cortisol are: morning from 260 to 720 nM, and 50-350 nM at night. Measuring blood pressure was completed with manual device Sprengler Official. 7, while the pulse and oxygen saturation of the c NONIN Onyx 9500 device.
Blood pressure measurements, arterial pulse and oxygen saturation on the day of extraction carried out as follows:
-
♦
First measurement was carried out 30 minutes before application of the anesthetic;
-
♦
Second measurement was carried out during the intervention (i.e. tooth extraction, wound rinse, debridement)
-
♦
Third measurement was carried out 30 minutes after the extraction of the tooth.
Given results for all measurements are compared by normal values of each parameter.
Statistical analysis
The tests used for statistical analysis are Kruskal Wallis test and Dunn’s Multiple Comparison test, One Way ANOVA and Bonferroni Multiple Comparison Test.
3. RESULTS
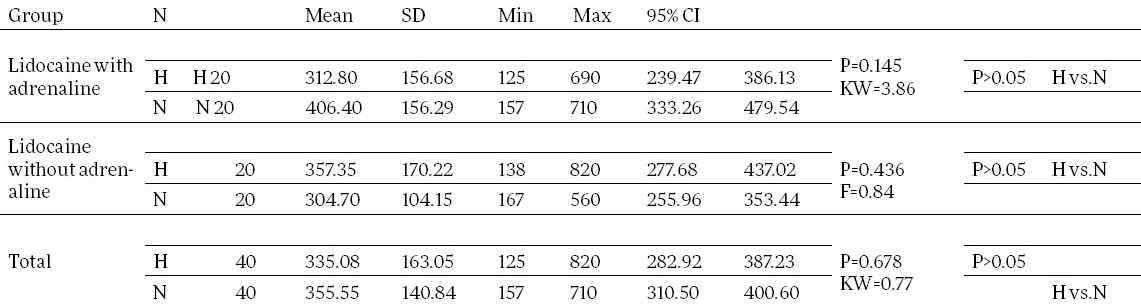
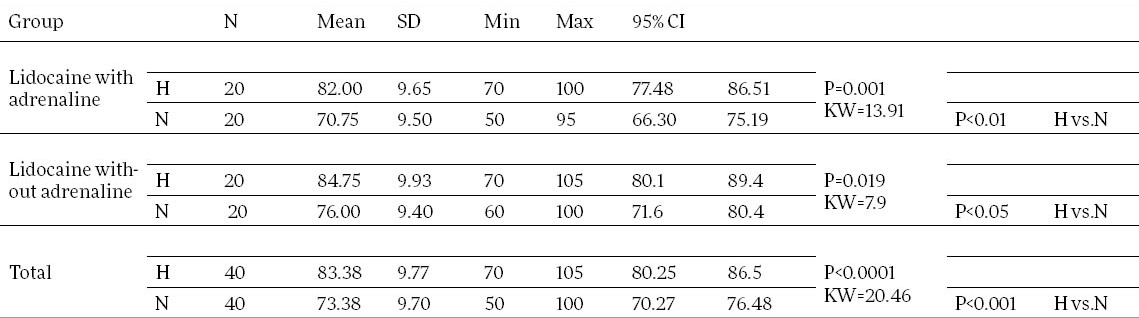
Based on the test that we used, for the cortisol level before tooth extraction, regardless of the type of the anesthetic used we haven’t found important statistical distinction between groups -hypertensive and normotensive patients, H vs. N, P>0.05. (Table 1).
Table 1.
Cortisol values before tooth extraction. H-Hypertensive; N-Normotensive
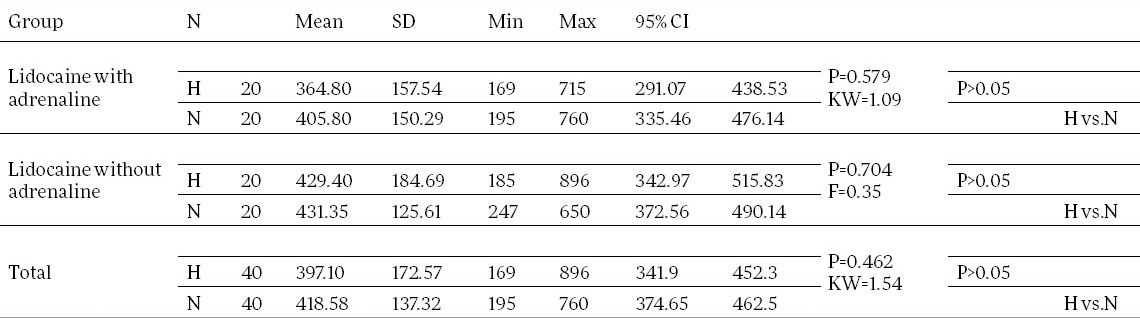
The same resulted for the cortisol level during (H vs. N, P>0.05) and after (H vs. N, P>0.05) tooth extraction, regardless of the type of the anesthetic used (Table 2, Table 3).
Table 2.
Cortisol values during tooth extraction
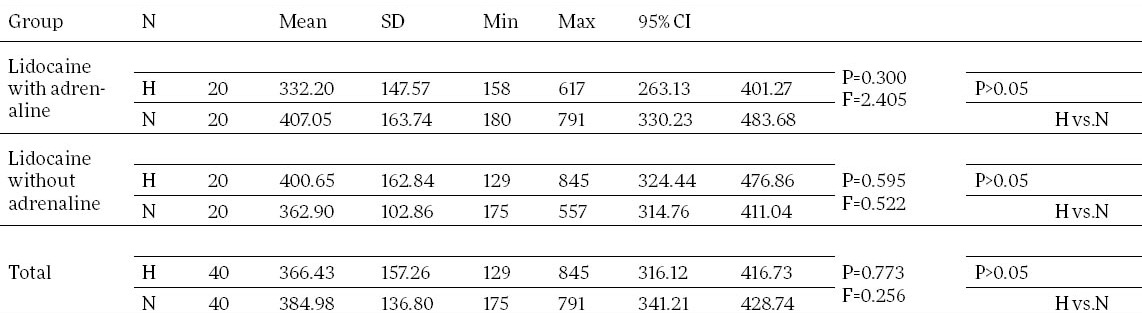
Table 3.
Cortisol values 30 minutes after tooth extraction
The values of systolic blood pressures resulted with significant statistical difference between the values of systolic blood pressure before, during and after tooth extraction in hypertension patients group (H) and Normotensive patient group (N), (P<0.0001) regardless of type of anesthetic used (Table 4, Table 5, Table 6).
Table 4.
Systolic blood pressure 30 minutes before tooth extraction
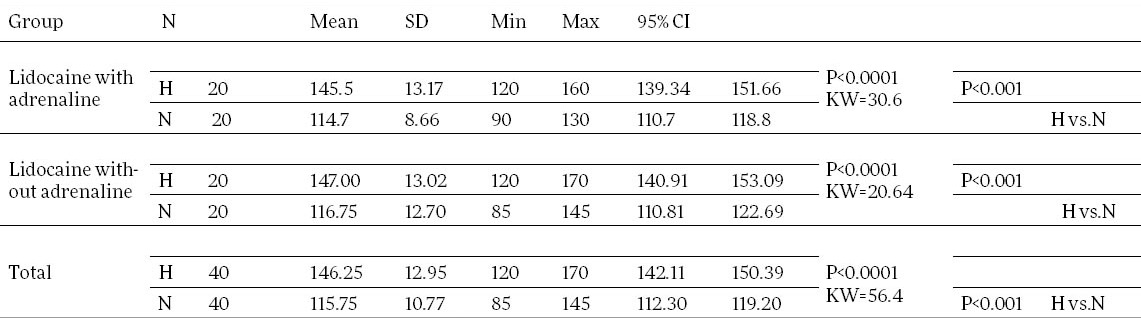
Table 5.
Systolic blood pressure during tooth extraction
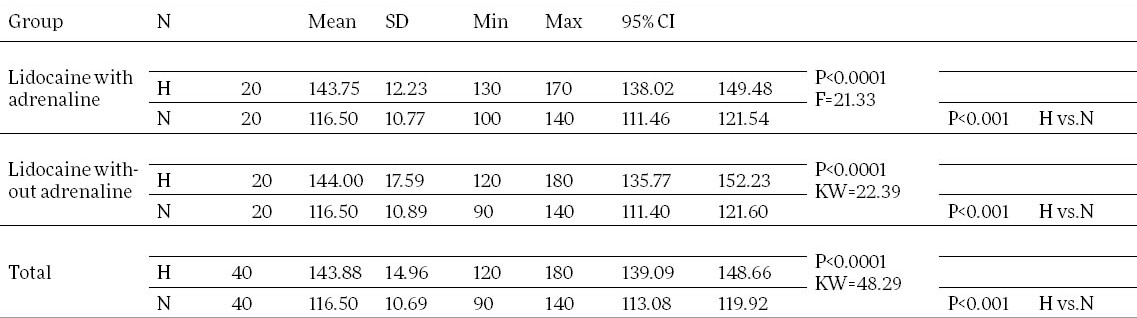
Table 6.
Systolic blood pressure 30 minutes after tooth extraction
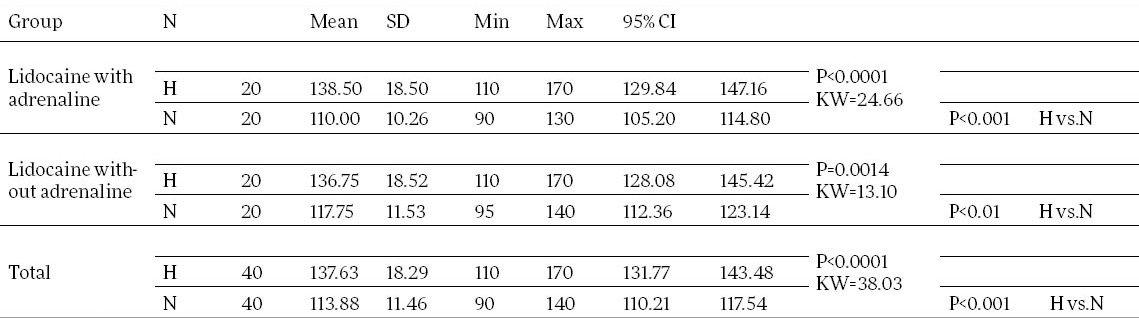
We registered a significant statistical difference where systolic arterial pressure is higher in hypertensive patients compared with patients with normal blood pressure, regardless of the type of anesthetic used.
Also the values of diastolic blood pressures resulted with significant statistical difference between the values of systolic blood pressure before, during and after tooth extraction in hypertension patients group (H) and Normotensive patient group (N), (P<0.0001) regardless of type of anesthetic used (Table 7, Table 8, Table 9).
Table 7.
Diastolic blood pressure 30 minutes before tooth extraction
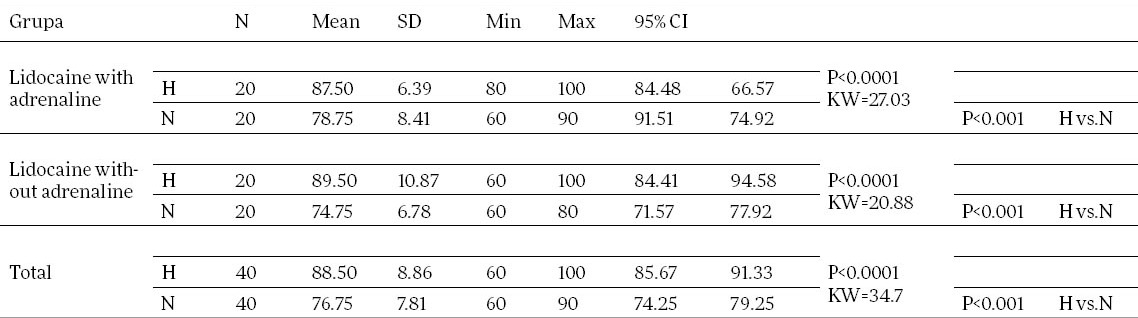
Table 8.
Diastolic blood pressure during tooth extraction
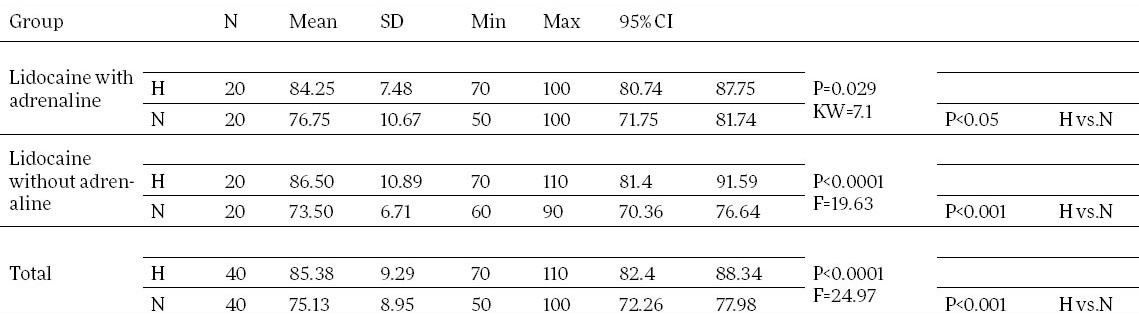
Table 9.
Diastolic blood pressure 30 minutes after tooth extraction
We registered a significant statistical difference where diastolic arterial pressure is higher in hypertensive patients compared with patients with normal blood pressure, regardless of the type of anesthetic used.
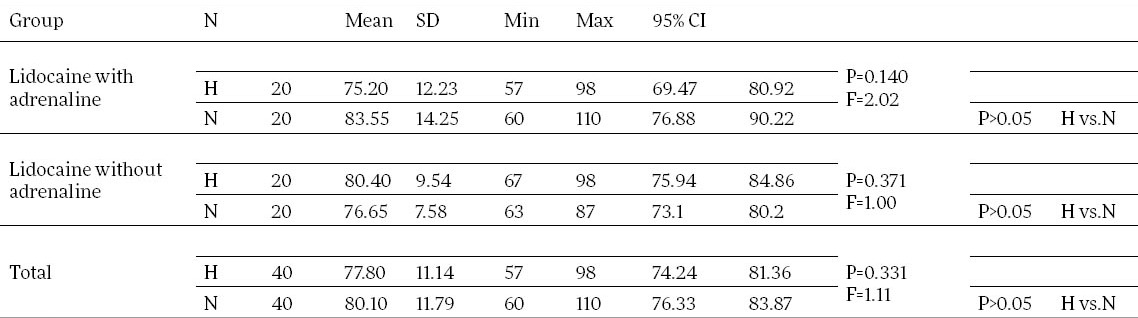
We haven’t found statistical significant difference in the values of the arterial pulse before, during and after the extraction of the tooth between the groups of patients with normal pressure, and hypertensive patients, regardless of the type of anesthetic used, H vs. N, P>0.05 (Table 10, Table 11, Table 12).
Table 10.
Puls rate 30 minutes before tooth extraction
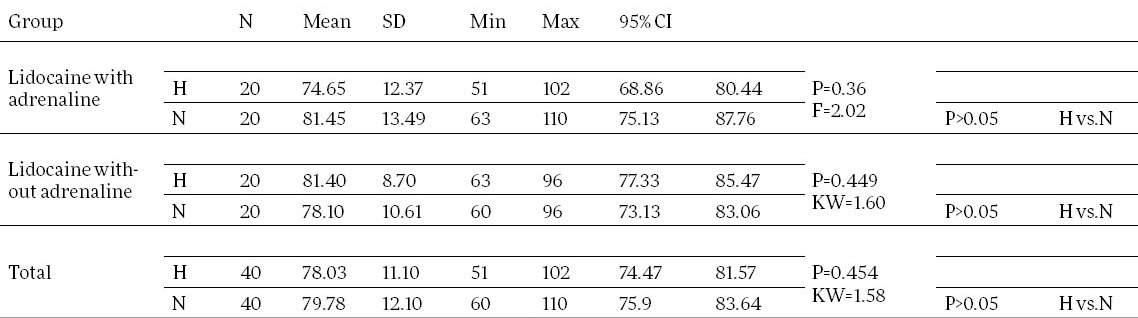
Table 11.
Puls rate during tooth extraction
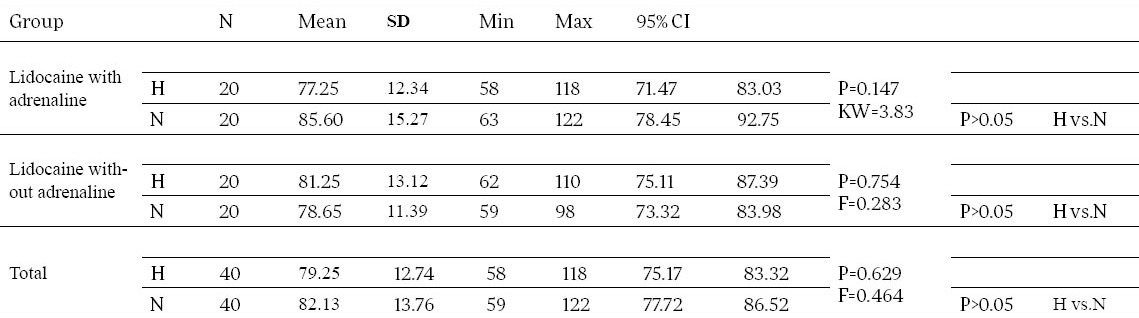
Table 12.
Puls rate 30 minutes after tooth extraction
4. DISCUSSION
Dental procedure such as tooth extraction is usually manifested with noticeable fear compared with other dental procedures (2, 5). Patients undergoing oral surgery interventions produce larger amounts of steroids compared to healthy patients who are not undergoing any dental intervention (1). The author Banks (1), investigated cortisol level during oral surgical procedures, and showed that it remained elevated 7 hours after oral surgery intervention. While the author Walker (8) demonstrate the link with the cortisol and pain through electronic stimulation of the pulp and states raised cortisol level 10 minutes after stimulation.
The research data of Miller (9) show an obvious increase in cortisol level in saliva after completion of extraction in 80% of cases as a result of stress produced after the extraction, which is more than a routine dental procedure. Similar results are given by Chamani (10) too.
Author Hill (11) concluded the cortisol increase level on the day of the tooth extraction and showed reduced cortisol level after intervention.
As per hemodynamic changes; In earlier studies by various authors regarding the evaluation of changes in blood pressure during dental treatments, special emphasis is placed on the cases of extraction of teeth, where authors appear with different results.
Tsutchihashi (12) results indicates that it cannot be prejudicial to raised blood pressure in the extraction of teeth based on baseline blood pressure or mental stress, but is caused by the tooth extracted and the amount of anesthetic that is used to control pain. The stress caused by pain is the most determinant factor to raised blood pressure during oral surgery interventions.
Similar results are found by the author Abraham (13) who proves rise in blood pressure from 10 to 70 mmHg as in normotensive and hypertensive patients during tooth extraction, while author Nakamura (14) in his study concluded measurable increase in systolic pressure during tooth extraction. (+10.8 +/- 3.5 mmHg).
As for the impact of catecholamine in changes of hemodynamic parameters, particularly blood pressure, various authors suggested the connection between the presence of catecholamine and blood pressure increase.
Application or use of vasoconstrictors in local anesthetics do not have significant hemodynamic changes in normotensive patients, although one observes an increase in systolic arterial pressure, especially after tooth extraction. This is attributed to the existence of anxiety that persists in extracting some time after extraction (13, 14). The blood pressure can rise during administration of local anesthetic, as well as fast and easy cut after removal of the needle from the mouth (17).
Stress caused by pain is the most influential factor to raise blood pressure during oral surgery interventions. Also the psychological factor may be the reason for the increase in blood pressure during tooth extraction. But, anxiety score or the impact of mental stress can imply changes in arterial pressure during the extraction of teeth (12). Significant hemodynamic changes are found in patients with controlled hypertension who underwent extraction of teeth regardless of anesthetic used with or without vasoconstrictor (15). Hypertensive patients who are administered a local anesthetic with vasoconstrictor show similar hemodynamic changes like at normotensive patients undergoing the same procedures and conditions (16).
The arterial pulse values vary depending on which tooth is extracted, and the amount of the local anesthetic required to control pain during intervention (12). Also after the local application of 2% lidocaine with 1: 100000 adrenaline, there is found a rise in arterial pulse in 19% of cases and the arterial pressure in 30% of cases (18).
Based on the study of author Gungormus (19) there is no statistically significant changes in systolic and diastolic arterial pressure, arterial pulse in all measurements between normotensive and hypertensive patients. On the other hand Liau (20) concluded that there is an increase in arterial pulse during tooth extraction when local anesthetic containing vasoconstrictor is applied. The study of Paramaesvaran (21) concluded the opposite, the reduction of arterial pulse during tooth extraction.
Also, the author Laragnoil (22) do not report an increase in blood pressure in patients with heart disease during treatment with dental anesthetic containing a vasoconstrictor, while author Neves (23) in patients with ischaemic heart disease during dental restorative treatments described slight increase in systolic arterial pressure
Furthermore, author Meyer (24) compares the hemodynamic changes in hypertensive and normotensive patients during tooth extraction with application of anesthetic, with or without epinephrine and notes that these changes are almost the same.
Author Meyer (24) in his study measured the hemodynamic changes during the extraction of teeth in hypertensive and normotensive patients and concluded that the increase in blood pressure in hypertensive patients during oral surgery interventions was similar or slightly higher in comparison to normotensive patients.
5. CONCLUSION
Our results indicate significant systolic and diastolic blood pressure rise in both groups of patients (regardless of anesthetic used with or without vasoconstrictor), hypertensive and normotensive patients, who underwent tooth extraction. The special emphasize is attributed to hypertensive patients where these changes are more significant. As per cortisol level and pulse rate, our results indicate no significant statistical difference in between groups.
Footnotes
CONFLICT OF INTEREST: NONE DECLARED.
REFERENCES
- 1.Banks P. The adenocortical response to oral surgery. Br J Oral Surgery. 1970;8:32–44. doi: 10.1016/s0007-117x(70)80065-8. [DOI] [PubMed] [Google Scholar]
- 2.Bell WE. Orofacial pains, classifications, diagnosis, management. 4th edition. St Louis: Mosby Year book; 1989. [Google Scholar]
- 3.Cacioppo J T, Tassinary L G, Berntson GG. Handbook of psychophysiology. Edition: 2. Cambridge University Press; 2000. [Google Scholar]
- 4.Creager JG. Human anatomy and Physiology. Brown Publishers; WCB. Wm C; 1992. [Google Scholar]
- 5.Kleinknect RA, Bernstein DA. The assessment of dental fear. Behav Ther. 1998;9:626–634. [Google Scholar]
- 6.Kućer Z. The objective measurement of pain in orofacial surgery. Acta Stomatologica Naissi. 2003;19:41. [Google Scholar]
- 7.Abubaker AO, Benson KJ. Oral and maxillofacial surgery secrets. NC./Philadelphia: Hanley & Belfus; 2001. [Google Scholar]
- 8.Walker BR, Soderberg S, Lindahl B, et al. Independent effects of obesity and cortisol in predicting cardiovascular risk factors in men and women. J Intern Med. 2000 doi: 10.1046/j.1365-2796.2000.00609.x. [DOI] [PubMed] [Google Scholar]
- 9.Miller S, Dembo JF, Falace DA, Kaplan AL, Lexington KY. Salivary cortisol response to dental treatment of varying stress. Oral Surg Oral Med Oral Pathol. 1995;79:436–440. doi: 10.1016/s1079-2104(05)80123-4. [DOI] [PubMed] [Google Scholar]
- 10.Chamani G, Gholamhoseinian A, Hedaja AT. Salivary Cortisol Response to Different Dental Treatments in Kermanian Patients. J Med Sci. 2006;6(1):55–58. [Google Scholar]
- 11.Hill CM, Walker RV. Salivary cortisol determination and self rating scales in the assessment of the stress in patients undergoing the extraction of the wisdom teeth. Oral Surg. 2001;191(9):513–515. doi: 10.1038/sj.bdj.4801220. [DOI] [PubMed] [Google Scholar]
- 12.Tsuchihashi T, Takata Y, Kurokawa H, Miura K, Maruoka Y, Kayijama M, Fujishima M. Blood pressure response during dental surgery. Hypertens Res. 1996 Sep;19(3):189–194. doi: 10.1291/hypres.19.189. [DOI] [PubMed] [Google Scholar]
- 13.Abraham IL, Borgmeijer-Hoelen A, Gortzak A. Changes in blood pressure, heart rate, and electrocardiogram during dental treatment with use of local anesthesia. J Am Dent Assoc. 1988:116. doi: 10.14219/jada.archive.1988.0318. [DOI] [PubMed] [Google Scholar]
- 14.Nakamura Y, Matsumura K, Miura K, Kurokawa H, Abe I, Takata Y. Cardiovascular and sympathetic responses to dental surgery with local anesthesia. Hypertens Res. 2001;24:209–214. doi: 10.1291/hypres.24.209. [DOI] [PubMed] [Google Scholar]
- 15.Silvestre FJ, Salvador MI, Bautista D, Silvestre RJ. Clinical study of hemodynamic changes during extraction in controlled hypertensive patients. Med Oral Patol Oral Cir Bucal. 2011;16(3):e354–8. doi: 10.4317/medoral.16.e354. [DOI] [PubMed] [Google Scholar]
- 16.Silvestre FJ, Verdú MJ, Sanchís JM, Grau D, Peñarrocha M. Effects of vasoconstrictors in dentistry upon systolic and diastolic arterial pressure. Med Oral. 2001;6:57–6. [PubMed] [Google Scholar]
- 17.Gortzak RA, Oosting J, Abraham IL. Blood pressure response to routine restorative dental treatment with and without local anesthesia: continuous noninvasive blood pressure registration with a finger manometer. Oral Surg Oral Med Oral Pathol. 1992;73(6):677–681. doi: 10.1016/0030-4220(92)90008-e. [DOI] [PubMed] [Google Scholar]
- 18.Dionne RA, Goldstein DS, Wirdzek PR. Effects of diazepam premedication and epinephrine containin local anesthetics on cardiovascular and plazma catecholamines responses to oral surgery. Anesth Analg. 1984;63:640–646. [PubMed] [Google Scholar]
- 19.Gungormus M, Buyukkurt MC. The evaluation of the changes in blood pressure and pulse rate of hypertensive patients during tooth extraction. Acta Med Austriaca. 2003;30(5):127–129. [PubMed] [Google Scholar]
- 20.Liau FL, Kok SH, Lee JJ, Kuo RC, Hwang CR, Yang PJ, et al. Cardiovascular influence of dental anxiety during local anesthesia for tooth extraction. Oral Surg Oral Med Oral Pathol Oral Radiol Endo. 2008;105:16–26. doi: 10.1016/j.tripleo.2007.03.015. [DOI] [PubMed] [Google Scholar]
- 21.Paramaesvaran M, Kingon AM. Alterations in blood pressure and pulse rate in exodontias patients. Oral Surgery. 1994;39(5):282–286. doi: 10.1111/j.1834-7819.1994.tb05563.x. [DOI] [PubMed] [Google Scholar]
- 22.Laragnoit AB, Neves RS, Neves IL, Vieira JE. Locoregional anesthesia for dental treatment in cardiac patients: a comparative study of 2% plain lidocaine and 2% lidocaine with epinephrine (1: 100,000) Clinics (Sao Paulo) 2009;64:177–182. doi: 10.1590/S1807-59322009000300005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Neves RS, Neves IL, Giorgi DM, Grupi CJ, Cesar LA, Hueb W, et al. Effects of epinephrine in local dental anesthesia in patients with coronary artery disease. Arq Bras Cardiol. 2007;88(5):545–551. doi: 10.1590/s0066-782x2007000500008. [DOI] [PubMed] [Google Scholar]
- 24.Meyer FU. Haemodynamic changes under emotional stress following a minor surgical procedure under local anesthesia. Int J Oral Maxillofac Surg. 1987;16:688–694. doi: 10.1016/s0901-5027(87)80054-1. [DOI] [PubMed] [Google Scholar]