

Abstract
Background:
Knee osteoarthritis is one of the most prevalent chronic disorders. Several pharmacological and non pharmacological approaches are used to treat this disease. Today, the effect of B and E vitamins on rheumatology diseases is being discussed. In this study, the efficacy of B and E vitamins accompanied with diclofenac on pain relief in patients with knee osteoarthritis was investigated and compared.
Methods:
In this double-blinded clinical trial, 120 patients with knee osteoarthritis referring training Rheumatology and Orthopedics Clinic of Shahrekord University of Medical sciences were investigated. Of these patients, 12 were excluded throughout the study. The patients underwent treatment in three groups (oral diclofenac + oral B vitamin, oral diclofenac + oral vitamin E, and oral diclofenac + placebo). Pain relief was assessed by visual analogue scale (VAS) questionnaire and morning stiffness and physical function were assessed by WOMAC standard questionnaire at three times; the first examination, two weeks, and three weeks after referring.
Results:
The mean score of WOMAC questionnaire at VASs of knee pain, total pain severity, knee joint stiffness, and function of the last 48 hours decreased significantly in all three groups (diclofenac, E and B vitamins) from the first to third examination (P<0.001). Decrease in VAS of knee pain and function of the last 48 hours was higher in B vitamin group than the diclofenac and E vitamin group (P=0.008) and decrease in total pain severity was reported higher in B vitamin group than E vitamin and diclofenac group (P=0.019). Decrease in knee joint stiffness underwent a similar trend in the three groups.
Conclusion:
In view similar analgesic and anti-inflammatory properties, as well as very few, non prevalent complications of B and E vitamins, use of two or more drugs with a different mechanism of effect seems necessary to enhance their effect on osteoarthritis treatment.
Keywords: Osteoarthritis, pain, B vitamin, E vitamin, diclofenac
1. INTRODUCTION
Osteoarthritis or arthrosis is one of the most prevalent types of arthritis and chronic joint disorder in human, which could lead to severe pain and chronic disability particularly in hip and knee (1-3). Studies have indicated that approximately 1/3 of above 45-year-old population of the USA suffer from osteoarthritis and it will become the fourth reason for increased worldwide due to increased life expectancy, sedentary lifestyle, and increased obesity rate (4, 5). In Iran, the prevalence of knee osteoarthritis in the ages over 15 years old was reported approximately 15.34%, which is considered a high prevalence (6). The treatment of this disease includes relieving pain and dealing with lack of physical function by means of multi-faceted, non pharmacological approaches. Today, the most commonly used drugs for pain relief in these patients are nonsteroidal anti-inflammatory drugs (NSAIDs) such as diclofenac. Diclofenac is an analgesic, anti-inflammatory drug and one of the most efficient inhibitors of prostaglandins which is used in treatment of rheumatic diseases (7, 8). Diclofenac could lead to headache, dizziness, rash, edema, and kidney and liver damage. The complications caused by this drug restrict its clinical usage (9, 10). Today, various supplements are used for osteoarthritis treatment. B vitamins are water-soluble vitamins, have been used as analgesic drug and promoter of analgesic effect of diclofenac in many studies, and cause a decrease in duration of treatment (11-13). Vitamin B complex (thiamine [B1], niacin [B3], cobalamin [B12]) is used not only for treatment of pain and inflammation but also, alone or accompanied with diclofenac, for various diseases such as polyneuropathy, spinal degenerative disease, rheumatic diseases and the pain following tonsillectomy (9,14). Medina-Santillan et al study indicated that consumption of diclofenac decreased by 30% in the patients who received vitamin B complex (7). B vitamin is one of the lipid-soluble vitamins in cell membrane. This vitamin neutralizes hydrogen peroxide and protects cell membrane against peroxidation (15). Alpha-tocopherol is a form of E vitamin which has the highest biological activity and its most abundant form exists in the body. Although all tocopherol homologues are absorbed similarly, alpha form is mainly found in blood and tissue (16). Clinical trial studies on comparison between E vitamin and placebo (17-19) have not reported definite findings on this vitamin. However, these works have recommended that 400-1200 mg tocopherol be used in view of various parameters including pain at pressure, relaxation, and motion. Since administration of NSAIDs have significantly increased in recent years and these drugs, as with most drugs, lead to deleterious side effects if administered for long term (7, 20), various studies on use of therapies that decrease consumption of sedatives, cause satisfaction in patients, and decrease costs are important. Today, use of some vitamins and other supplements for pain relief and other symptoms of osteoarticular diseases including osteoarthritis is being challenged. The purpose of the present study is to determine the efficacy of B and E vitamins on pain relief in the patients with knee osteoarthritis and compare it with diclofenac as a type of NSAID.
2. PATIENTS AND METHODS
This double-blinded clinical trial was conducted in 2013-2014 on 120 patients referring training Rheumatology and Orthopedics Clinic of Shahrekord University of Medical Sciences with confirmed diagnosis of primary knee osteoarthritis. The inclusion criteria were the age of 30 to 60 years, diagnosis of primary knee osteoarthritis by an orthopedics (per descriptions, clinical symptoms, physical examinations, radiologic and relevant diagnostic criteria of this disease. The exclusion criteria were secondary knee osteoarthritis, primary infection or inflammatory disease in knee joint, arthritis due to crystal, intra-articular tumors, knee ligament instability, previous intra-articular fracture, knee joint surgery (arthroscopic or otherwise) in the past 12 months, intra-articular injection, visual analogue scale (VAS) score less than 3 for the knee under treatment at treatment initiation, concomitant severe diseases such as metabolic diseases, history of some diseases like stroke, uncontrolled hypertension, gastritis, infectious diseases, kidney failure, ulcer, and sensitivity to vitamin B complex, vitamin E, and vitamin B, and other contraindications of vitamins B and E administration. In case of development of the complications due to the drugs, lack of regular consumption of the drug (vitamin B complex and vitamin E), sensory impairment in the lower limbs, use of an additional sedative, lack of patient’s cooperation, and pregnancy, the patient was excluded from the study. After being enrolled and completing consent form, the patients were randomly assigned to three groups of 40 each: one control group and two intervention groups. All three groups were administered with oral diclofenac 50 mg twice a day. For intervention 1 group, intervention 2, and control groups, respectively vitamin B complex tablet, vitamin E tablet 100 mg, and diclofenac plus a placebo tablet was daily administered. The patients were examined three times (on the first day, day 14, and day 21) and the relevant questionnaire was completed for them. First section: Demographic variables including age, gender, occupation, education, marital status, and body mass index (BMI); second section: VAS questionnaire ticked by the patients using a 100-mm horizontal line in the three steps; and the third section: WOMAC standard questionnaire used for assessment of morning stiffness and physical performance in the patients. WOMAC questionnaire has been studied in several studies and its validity and reliability have been confirmed (21-23). The questionnaire items have been codified as Likert scale (painless, mild pain, moderate pain, severe pain, very severe pain) and assessment is done in three sections: 1. Pain assessment (5 items); 2. Joint stiffness (2 items); and 3. Physical function (17 items). The pain which is examined in the present study is assessed by the five first items of this questionnaire (pain section) and VAS at the end of the questionnaire. After gathering the data, we analyzed the data by SPSS 17 using descriptive statistics, chi square, analysis of variance (ANOVA), and repeated measures ANOVA.
3. RESULTS
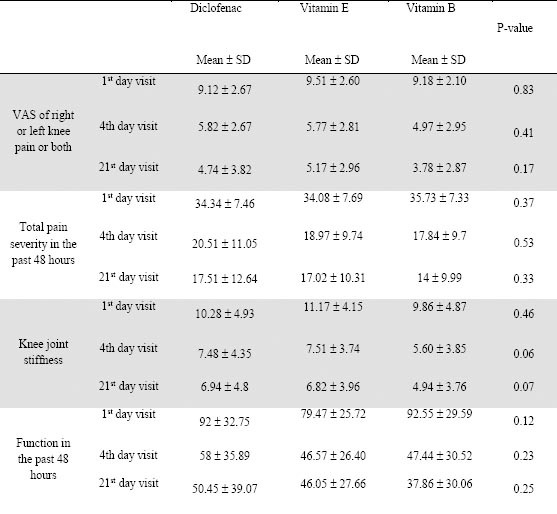
Of 120 patients participating in this study. 12 (5 in diclofenac and vitamin E groups and 4 in vitamin B group) declined to continue participating and finally the data of 108 patients were analyzed. In diclofenac group (n=37) 57.1% (n=20) were female, 42.9% (n=15) were male, and the patients were 30 to 63 years old. In vitamin E group (n=35) 62.9% (n=22) were female, 37.1% (n=15) were male, and the patients were 30 to 60 years old. In vitamin B group (n=38) 55.3% (n=21) were female, 44.71% (n=17) were male, and the patients were 33 to 60 years old. Mean age was 46.40±8.7 years in diclofenac group, 47.54±8.97 in vitamin E group, and 46.78±8.31 in vitamin B group. In addition, the mean BMI was 26.31±3.09 in diclofenac group, 26.40±1.97 in vitamin E group, and 27.51±3.76 in vitamin B group. Most patients in the diclofenac group, the vitamin E group, and the vitamin B group were respectively public servant, housewife, and housewife (51.4%, 34.3%, and 39.15%, respectively). Also, most patients in the diclofenac group (62.4%) were holders of associate degree and higher and in the vitamin E and vitamin B groups (respectively 37.1% and 36.8%) were illiterate. Chi square indicated no statistically significant difference in age, gender, and occupation among the groups (p>0.05) (Table 1). ANOVA indicated no statistically significant difference in BMI among the groups (p=0.17). By ANOVA, mean score of WOMAC (knee pain VAS, total pain severity, knee joint stiffness, and the past 48-hour function) was not significantly different prior to and after the first examination among the three groups (p>0.05). In addition, in the second examination only the past 48-hour function was lower in the vitamin E group than in the vitamin B and diclofenac groups and other variables of study (knee pain VAS, total pain severity, and knee joint stiffness) were reported lower in the vitamin B group than in the vitamin E and diclofenac groups (p>0.05). In the third examination, the mean score of all WOMAC sections was lower in the vitamin B group than in the vitamin E and diclofenac groups with no statistically significant difference (p>0.05) (Table 2). By repeated measures ANOVA, decrease in knee pain VAS, total pain severity, knee joint stiffness, and the past 48-hour function changed significantly from the first to the third examination (p=0.001). Except for knee joint stiffness with a similar decreasing trend in all three groups, other variables including knee pain VAS, total pain severity, knee joint stiffness, and the past 48-hour function changed differently in the three groups so that decrease in knee pain VAS and the past 48-hour function was reported higher in the vitamin B group than in the diclofenac and vitamin E groups (p=0.008) and the decrease in total pain severity was reported higher in the vitamin B group than in the diclofenac and vitamin E groups (p=0.019). On satisfaction with treatment, by chi square test the patients in the vitamin B group reported a higher satisfaction than those in the diclofenac and vitamin E groups so that 29 (76.3%) patients in the vitamin B group, 25 (71.4%) patients in the diclofenac group, and 24 (68.6%) patients in the vitamin E group had a high and very high satisfaction, but generally the difference was not reported as statistically different (p=0.45).
Table 1.
Frequency distribution for demographic variables of the patients in three diclofenac, vitamin E, and vitamin B groups
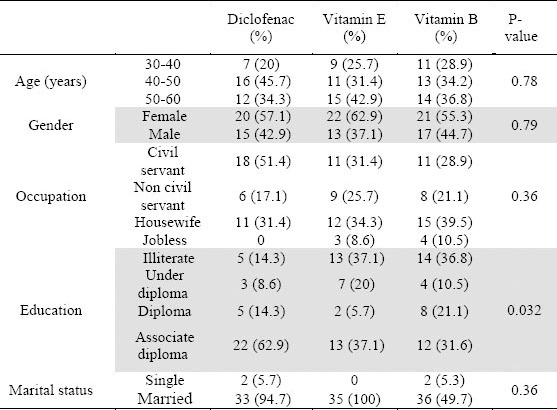
Table 2.
Comparison of mean WOMAC questionnaire scales of the patients in three diclofenac, vitamin E, and vitamin B groups
4. DISCUSSION
Osteoarthritis is one of the most prevalent diseases which involves many joints in the body including knee joint. NSAIDs including diclofenac are considered as the first line drugs for this disease. Administration of these drugs has become restricted because of their complications and risks with upper gastrointestinal tract toxicity, edema, and renal failure as the most prevalent. The present study was conducted to compare B and E vitamins with diclofenac in osteoarthritis treatment. In this study, the patients underwent treatment for three weeks (day 1, day 14, and day 21). By the findings of this study, the treatment led to pain relief in all three (vitamin B, vitamin E, and diclofenac) groups according to WOMAC questionnaire and the symptoms recovered significantly in all three groups after the third examination (day 21).
Mean VAS of knee pain was 9.18 in the first examination and 3.78 in the third examination in the vitamin B group, 9.51 in the first examination and 5.17 in the third examination in the vitamin E group, and 8.82 in the first examination and 4.74 in the third examination in the diclofenac group. Totally, the decrease in knee pain VAS was significantly higher in the vitamin B group than in the vitamin E and diclofenac groups. Mean total pain severity was 35.73 in the first examination and 14 in the third examination in the vitamin B group, 34.08 in the first examination and 17.02 in the third examination in the vitamin E group, and 33.34 in the first examination and 17.51 in the third examination in the diclofenac group. Totally, the decrease in total pain severity was significantly higher in the vitamin B group than in the vitamin E and diclofenac groups. In a similar study, Magana-Villa et al indicated that diclofenac combined with vitamin B groups had better analgesic effects in the interval under study and a better understanding of pain relief by the patients compared with diclofenac alone. This study was some clinical support for improvement of diclofenac analgesic effect after combination with vitamin B in osteoarthritis patients (24). Also, in Bruggemann et al study, promotion of analgesic effect of diclofenac by vitamin B complex was reported for recovery of low back pain (25). In Hector et al study, the analgesic effect of B complex was demonstrated and combined administration of diclofenac and B complex was highlighted as a suitable, cheap approach to relieving the pain before and after surgery (26).
Various mechanisms have been recommended to explain how vitamin B complex affects pain relief and inflammation in laboratory experiments. For example, this vitamin could lead to enhanced effect and/or availability of norepinephrine and also increased activity of 5-HT that contributes to pain transmission as an inhibitory pain transmitter (27). In an in vitro study Reyes-Garcia reported analgesic and anti-inflammatory effects of B complex that were relevant to the mechanisms similar to opioids and mediated by releasing nitrite oxide (11,28). In Reyes-Garcia study the analgesic effect of B12 was higher than B6 and that of B6 was higher than B1 (28).
In a study in 2006-2007 the effects of vitamin E and glucosamine sulfate on pain relief were compared in the patients with knee osteoarthritis. After a six-month treatment, both groups exhibited a pronounced recovery by WOMAC scale and a considerable decrease in VAS in both standing and sitting positions with no significant difference. That study reported that oral vitamin E at 400 mg dose per day contributes potentially to decreasing symptoms in knee osteoarthritis patients with no serious side effects (29). In addition, Brand et al study in contrast to our study compared the effects of oral vitamin E and placebo on reducing symptoms of knee osteoarthritis. The two groups indicated no recovery by WOMAC and no significant decrease in knee pain, morning stiffness, and daily functioning by VAS, and no significant difference was observed between the two groups. The findings of this six-month study represented vitamin E as playing no role in recovery of knee osteoarthritis symptoms (30). No explanation has been yet offered for the mechanism of vitamin E effect on osteoarthritis and this has remained unknown. However, vitamin E effect seems to be related to alpha tocopherol activity against oxygen free radicals and lipids peroxidation. A study by Surapaneni et al compared serum levels of various compounds including vitamin E in the patients with and without osteoarthritis. Vitamin E level was lower in the patients than in the controls in that study arguing oxygen free radicals and oxidative reactions contributed to developing osteoarthritis (31). Also, the role of vitamin E in treating chronic polyarthritis symptoms was well demonstrated in Wittenborg et al study (32).
5. CONCLUSION
Since alternative therapies have been repeatedly studied in numerous works including those investigating the effect of vitamins B and E on osteoarthritis symptoms and in view of the present study findings, similar analgesic and anti-inflammatory effects of vitamins E and B, and their few and infrequent complications, use of both and/or other drugs with a different mechanism of effect is recommended to enhance their effect on treating osteoarthritis symptoms.
Footnotes
CONFLICT OF INTEREST: NONE DECLARED.
REFERENCES
- 1.Verkleij SP, Luijsterburg PA, Koes BW, Bohnen AM, Bierma-Zeinstra SM. Effectiveness of diclofenac versus acetaminophen in primary care patients with knee osteoarthritis: [NTR1485], DIPA-trial: design of a randomized clinical trial. BMC Musculoskelet Disord. 2010;11:7. doi: 10.1186/1471-2474-11-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Sutipornpalangkul W, Morales NP, Charoencholvanich K, Harnroongroj T. Lipid peroxidation, glutathione, vitamin E, and antioxidant enzymes in synovial fluid from patients with osteoarthritis. Int J Rheum Dis. 2009;12(4):324–328. doi: 10.1111/j.1756-185X.2009.01430.x. [DOI] [PubMed] [Google Scholar]
- 3.Harvey WF, Hunter DJ. The role of analgesics and intra-articular injections in disease management. Rheum Dis Clin North Am. 2008;34(3):777–788. doi: 10.1016/j.rdc.2008.05.006. [DOI] [PubMed] [Google Scholar]
- 4.Murray CJ, Richards MA, Newton JN, Fenton KA, Anderson HR, Atkinson C, et al. UK health performance: findings of the Global Burden of Disease Study 2010. Lancet. 2013;23(381) 9871:997–1020. doi: 10.1016/S0140-6736(13)60355-4. [DOI] [PubMed] [Google Scholar]
- 5.Woolf AD, Pfleger B. Burden of major musculoskeletal conditions. Bull World Health Organ. 2003;81(9):646–656. [PMC free article] [PubMed] [Google Scholar]
- 6.Hashemi SM, Madadi F, Razavi S, Nikooseresht M, Hassanzadeh Kiyabi F, Nasiripour S. Intra-articular hyaluronic acid injections Vs. dextrose prolotherapy in the treatment of osteoarthritic knee pain. Tehran Univ Med J. 2012;70(2):119–125. [Google Scholar]
- 7.Medina-Santillan R, Perez-Flores E, Mateos-Garcia E, Reyes-Garcia G, Granados-Soto V, Flores-Murrieta FJ. A B-vitamin mixture reduces the requirements of diclofenac after tonsillectomy: A double-blind study. Drug Development Research. 2005;66(1):36–39. [Google Scholar]
- 8.Beck A, Salem K, Krischak G, Kinzl L, Bischoff M, Schmelz A. Nonsteroidal anti-inflammatory drugs (NSAIDs) in the perioperative phase in traumatology and orthopedics effects on bone healing. Oper Orthop Traumatol. 2005;17(6):569–578. doi: 10.1007/s00064-005-1152-0. [DOI] [PubMed] [Google Scholar]
- 9.Mibielli MA, Geller M, Cohen JC, et al. Diclofenac plus B vitamins versus diclofenac monotherapy in lumbago: the DOLOR study. Curr Med Res Opin. 2009;25(11):2589–2599. doi: 10.3111/13696990903246911. [DOI] [PubMed] [Google Scholar]
- 10.Sena MM, Chaudhry ZF, Collins CH, Poppi RJ. Direct determination of diclofenac in pharmaceutical formulations containing B vitamins by using UV spectrophotometry and partial least squares regression. Journal of Pharmaceutical and Biomedical Analysis. 2004;36(4):743–749. doi: 10.1016/j.jpba.2004.08.001. [DOI] [PubMed] [Google Scholar]
- 11.Reyes-Garcia G, Medina-Santillan R, Teran-Rosales F, Castillo-Henkel C, Rodriguez-Silverio J, Torres-Lopez JE, et al. Analgesic effect of B vitamins in formalin-induced inflammatory pain. Proc West Pharmacol Soc. 2001;44:139–140. [PubMed] [Google Scholar]
- 12.Levin OS, Moseikin IA. [Vitamin B complex (milgamma) in the treatment of vertebrogenic lumbosacral radiculopathy] Zh Nevrol Psikhiatr Im S S Korsakova. 2009;109(10):30–35. [PubMed] [Google Scholar]
- 13.Kuhlwein A, Meyer HJ, Koehler CO. [Reduced diclofenac administration by B vitamins: results of a randomized double-blind study with reduced daily doses of diclofenac (75 mg diclofenac plus B vitamins) in acute lumbar vertebral syndromes] Klin Wochenschr. 1990 Jan 19;68(2):107–115. doi: 10.1007/BF01646857. [DOI] [PubMed] [Google Scholar]
- 14.Perez-Flores E, Medina-Santillan R, Reyes-Garcia G, Mateos-Garcia E. Combination of diclofenac plus B vitamins in acute pain after tonsillectomy: a pilot study. Proc West Pharmacol Soc. 2003;46:88–90. [PubMed] [Google Scholar]
- 15.Hashimoto A, Hayashi I, Murakami Y, Sato Y, Kitasato H, Matsushita R, et al. Antiinflammatory mediator lipoxin A4 and its receptor in synovitis of patients with rheumatoid arthritis. J Rheumatol. 2007 Nov;34(11):2144–2153. [PubMed] [Google Scholar]
- 16.Shalaby MA, Zorba EHY. Protective effect of celery oil, Vitamin E and their combination against testicular damage in male rats. Global Veterinaria. 2010;5(2):122–128. [Google Scholar]
- 17.Paredes S, Girona J, Hurt-Camejo E, Vallve JC, Olive S, Heras M, et al. Antioxidant vitamins and lipid peroxidation in patients with rheumatoid arthritis: association with inflammatory markers. J Rheumatol. 2002 Nov;29(11):2271–2277. [PubMed] [Google Scholar]
- 18.Karlson EW, Shadick NA, Cook NR, Buring JE, Lee IM. Vitamin E in the primary prevention of rheumatoid arthritis: the Women's Health Study. Arthritis Rheum. 2008 Nov 15;59(11):1589–1595. doi: 10.1002/art.24194. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Brand C, Snaddon J, Bailey M, Cicuttini F. Vitamin E is ineffective for symptomatic relief of knee osteoarthritis: a six month double blind, randomised, placebo controlled study. Annals of the rheumatic diseases. 2001;60(10):946–949. doi: 10.1136/ard.60.10.946. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Fiorucci S, Antonelli E, Morelli A. Mechanism of nonsteroidal anti-inflammatory drug-gastropathy. Digestive and Liver Disease. 2001;33(2):S35–S43. doi: 10.1016/s1590-8658(01)80157-2. [DOI] [PubMed] [Google Scholar]
- 21.Melzack R. Pain: past, present and future. Can J Exp Psychol. 1993 Dec;47(4):615–629. doi: 10.1037/h0078871. [DOI] [PubMed] [Google Scholar]
- 22.Moeini M, Zare Z, Hazrati M, Saghaei M. Effect of therapeutic touch on patients’ anxiety before coronary artery bypass graft surgery. Iran J Nurs Midwifery Res. 2008;13(2):47–51. [Google Scholar]
- 23.Abolhasani SH. The effect of sensory motivation on patient's anxiety in CCU. J Kurdistan Univ Med Sci. 2007;12:46–52. [Google Scholar]
- 24.Magana-Villa MC, Rocha-Gonzalez HI, Fernandez del Valle-Laisequilla C, Granados-Soto V, Rodriguez-Silverio J, Flores-Murrieta FJ, et al. B-vitamin mixture improves the analgesic effect of diclofenac in patients with osteoarthritis: a double blind study. Drug Res (Stuttg) 2013 Jun;63(6):289–692. doi: 10.1055/s-0033-1334963. [DOI] [PubMed] [Google Scholar]
- 25.Reyes-Garcia G, Medina-Santillan R, Teran-Rosales F, Mateos-Garcia E, Castillo-Henkel C. Characterization of the potentiation of the antinociceptive effect of diclofenac by vitamin B complex in the rat. J Pharmacol Toxicol Methods. 1999 Oct;42(2):73–77. doi: 10.1016/s1056-8719(00)00045-9. [DOI] [PubMed] [Google Scholar]
- 26.Ponce-Monter HA, Ortiz MI, Garza-Hernandez AF, Monroy-Maya R, Soto-Rios M, Carrillo-Alarcon L, et al. Effect of diclofenac with B vitamins on the treatment of acute pain originated by lower-limb fracture and surgery. Pain Res Treat. 2012;2012:104782. doi: 10.1155/2012/104782. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Medina-Santillan R, Perez-Flores E, Mateos-Garcia E, Reyes-Garcia G, Granados-Soto V, Flores-Murrieta F. A B-Vitamin mixture reduces the requirements of diclofenac after tonsillectomy: a double-blind study. Drug Develop Res. 2005;66(1):36–39. [Google Scholar]
- 28.Reyes-Garcia G, Castillo-Henkel C, Medina-Santillan R, Teran-Rosales F, Granados-Soto V. Mechanisms of analgesic action of B vitamins in formalin-induced inflammatory pain. Proc West Pharmacol Soc. 2002;45:144–146. [PubMed] [Google Scholar]
- 29.Haflah NH, Jaarin K, Abdullah S, Omar M. Palm vitamin E and glucosamine sulphate in the treatment of osteoarthritis of the knee. Saudi Med J. 2009 Nov;30(11):1432–1438. [PubMed] [Google Scholar]
- 30.Brand C, Snaddon J, Bailey M, Cicuttini F. Vitamin E is ineffective for symptomatic relief of knee osteoarthritis: a six month double blind, randomised, placebo controlled study. Ann Rheum Dis. 2001 Oct;60(10):946–949. doi: 10.1136/ard.60.10.946. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Surapaneni KM, Venkataramana G. Status of lipid peroxidation, glutathione, ascorbic acid, vitamin E and antioxidant enzymes in patients with osteoarthritis. Indian J Med Sci. 2007 Jan;61(1):9–14. [PubMed] [Google Scholar]
- 32.Wittenborg A, Petersen G, Lorkowski G, Brabant T. [Effectiveness of vitamin E in comparison with diclofenac sodium in treatment of patients with chronic polyarthritis] Z Rheumatol. 1998;57(4):215–221. doi: 10.1007/s003930050094. [DOI] [PubMed] [Google Scholar]