

Highlights
-
•
We performed a subscapular muscle flap surgery to cover a chest wall defect.
-
•
No previous study has reported this technique for chest wall reconstruction.
-
•
The subscapular muscle flap technique can be conducted using the same incision as a lobectomy.
-
•
The subscapular muscle flap technique does not require plastic surgery support.
-
•
During the technique, the lower third of the scapula needs to be excised.
Keywords: Chest wall reconstruction, Subscapularis muscle, Muscle flap, Lung cancer
Abstract
Introduction
Chest wall skeletal defects are usually closed using muscle flaps or prosthetic materials. Postoperative prosthetic infections are critical complications and often require plastic surgery support. We report a new surgical technique, involving a subscapular muscle flap, for covering posterior chest wall defect.
Presentation of case
A 75-year-old man was admitted to our hospital. We performed a right upper lobectomy with posterior chest wall resection between the third and sixth ribs. The resulting chest wall defect was covered with a polytetrafluoroethylene mesh that became infected postoperatively. We removed the infected mesh and used the subscapularis muscle, the nearest muscle to the defect, to cover the chest wall defect. The scapular tip was lifted and the lower half of the muscle was dissected. The free end of the flap was sutured to the stumps of the anterior serratus and rhomboid major muscles. Computed tomography, 1 month later, revealed that the flap was engrafted to the chest wall.
Discussion
No previous study has reported the use of a subscapularis muscle flap for chest wall reconstruction. The lower third of the scapula was excised since blood supply to the scapula tip may be reduced after dissection of the subscapularis muscle, and to prevent the scapula tip from falling into the thoracic cavity.
Conclusion
The use of a subscapularis muscle flap to repair chest wall defect is a simple and safe technique that can be conducted in the same surgical field as the initial reconstruction surgery and does not require plastic surgery support.
1. Introduction
Chest wall skeletal defects are usually closed using muscle flaps, other autogenous tissue, or prosthetic materials [1,2]. However, reconstruction procedures involving typical muscle flaps, such as the pectoralis major, latissimus dorsi, serratus anterior, and rectus abdominis, need additional incisions and plastic surgery support [1]. Further, postoperative complications after prosthetic reconstruction reportedly occur in 46.2% of cases, with infection being a critical complication that occurs in 4.6% of cases [2], necessitating emergency surgery. No further reconstruction may be needed after healing from the initial surgery has occurred and the infected prosthetic material has been removed, since the lung may be adherent to the chest wall. However, in most cases, additional autogenous tissue flaps are needed [1,2].
Here, we report the use of a subscapular muscle flap to cover posterior chest wall defect after removal of infected prosthetic material. Our technique is simple, safe, and can be performed in the same surgical field as the initial surgery, without the need for plastic surgery support.
2. Presentation of case
A 75-year-old man was admitted to our hospital for lung cancer surgery. He underwent a right upper lobectomy with posterior chest wall resection, from the third to sixth ribs, via posterior lateral thoracotomy. The chest wall defect was covered with a 17 × 22 cm polytetrafluoroethylene mesh. The patient developed fever and back pain on postoperative day 10. Chest computed tomography showed an abscess around the mesh, along with empyema. Emergency surgery was performed on the same day.
The wound created during the initial surgery was incised, the infected mesh was removed, and the thoracic cavity was washed using a large quantity of saline. The subscapularis muscle, the nearest muscle to the defect area, was used to cover the chest wall defect.
The scapular tip of the subscapularis muscle was lifted and its lower half was dissected using electric cautery. The pedicle was attached to the upper half of the scapula (Fig. 1A). The same parts of the infraspinatus and teres major muscles were also dissected from the scapula. Subsequently, the lower third of the scapula was excised using a sternum saw. The size of the subscapularis muscle flap was adequate to cover the defect. The free end of the flap was sutured to the stumps of the anterior serratus and rhomboid major muscles, which had been cut during the initial surgery (Fig. 1B).
Fig. 1.
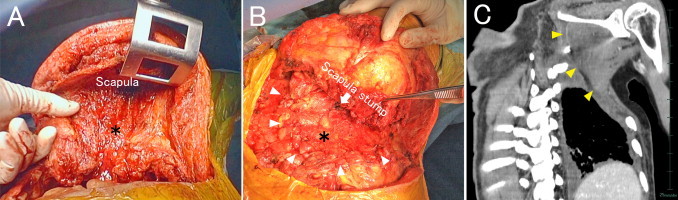
A: The lower half of the subscapularis muscle was dissected from the scapula. *subscapularis muscle flap. B: The subscapularis muscle flap was sutured to the serratus anterior and rhomboid major muscles (white arrowhead). The lower third of the scapula was excised (arrow). *subscapularis muscle flap. C: Computed tomography image 1 month after reconstruction. The flap is engrafted to the chest wall (yellow arrowhead).
Postoperatively, the abscess and empyema resolved. The functionality of the upper extremity on the affected side was limited, but was restored with rehabilitation. The flap slightly atrophied, but remained engrafted to the chest wall (Fig. 1C).
3. Discussion
Although scapular and parascapular flaps are commonly used as free flaps in head and neck reconstructions [3], to our knowledge, no previous study has reported the use of a subscapularis muscle flap for chest wall reconstruction. The main advantage of this flap is that since dissection of the subscapularis muscle is simple, plastic surgery support is not required. Thoracic surgeons can preoperatively evaluate the muscle volume using computed tomography and obtain an adequate flap size.
In our experience, it is important to suture the subscapularis muscle flap to the serratus anterior and rhomboid major muscles for thoracic cavity closure and to ensure adequate blood supply to the free end of the flap. The subscapularis muscle and scapula are supplied by the dorsal scapular artery, suprascapular artery, and subscapular artery, which form an arterial plexus around the scapula [4]. A previous study identified the angular branch of the thoracodorsal artery to be the main vascular supply to the scapula tip [4]. In the present case, the lower third of the scapula was excised since blood supply to the scapula tip may be reduced after dissection of the subscapularis muscle, and to prevent the scapula tip from falling into the thoracic cavity (Fig. 2).
Fig. 2.
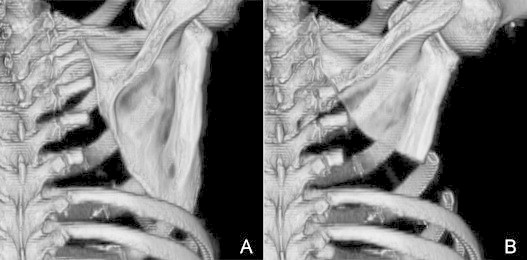
A: Computed tomography image after the initial lobectomy, with chest wall resection, showing that the scapula tip had fallen into the thoracic cavity. B: Excised scapula prevents it from falling into the thoracic cavity.
4. Conclusions
The subscapularis muscle flap surgery for reconstruction of chest wall skeletal defect, following removal of contaminated prosthetic material, is a simple and safe technique that can be conducted in the same surgical field as the initial reconstruction surgery and does not require plastic surgery support. Thus, this technique may be an option for posterior chest wall skeletal defect reconstruction.
Conflict of interest
We have no conflict of interest.
Funding
None.
Ethical approval
Written informed consent was obtained from this patient for publication of this case report and any accompanying figures.
Authors contributions
Mitsuaki Sakai was the surgeon of this work and wrote this case report. Masatoshi Yamaoka and Yukinobu Goto collected the data and assistant surgeons. Yukio Sato revised this report.
References
- 1.Arnold P.G., Pairolero P.C. Chest-wall reconstruction: an account of 500 consecutive patients. Plast. Reconstr. Surg. 1996;98:804–810. doi: 10.1097/00006534-199610000-00008. [DOI] [PubMed] [Google Scholar]
- 2.Deschamps C., Tirnaksiz B.M., Darbandi R. Early and long-term results of prosthetic chest wall reconstruction. J. Thorac. Cardiovasc. Surg. 1999;117:588–591. doi: 10.1016/s0022-5223(99)70339-9. [DOI] [PubMed] [Google Scholar]
- 3.Mitsimponas K.T., Iliopoulos C., Stockmann P. The free scapular/parascapular flap as a reliable method of reconstruction in the head and neck region: a retrospective analysis of 130 reconstructions performed over a period of 5 years in a single department. J. Craniomaxillofac. Surg. 2014;42:536–543. doi: 10.1016/j.jcms.2013.07.023. [DOI] [PubMed] [Google Scholar]
- 4.Seneviratne S., Duong C., Taylor G.I. The angular branch of the thoracodorsal artery and its blood supply to the inferior angle of the scapula: an anatomical study. Plast. Reconstr. Surg. 1999;104:85–88. [PubMed] [Google Scholar]