

Abstract
Background:
Laminectomies with posterior cervical instrumented fusions often utilize bone graft expanders to supplement cervical lamina/iliac crest autograft/bone marrow aspirate (BMA). Here we compared posterior fusion rates utilizing two graft expanders; Vitoss (Orthovita, Malvern, PA, USA) vs. NanOss Bioactive (Regeneration Technologies Corporation [RTI: Alachua, FL, USA]).
Methods:
Two successive prospective cohorts of patients underwent 1-3 level laminectomies with 5-9 level posterior cervical fusions to address cervical spondylotic myelopathy (CSM) and/or ossification of the posterior longitudinal ligament (OPLL). The first cohort of 72 patients received Vitoss, while the second cohort or 20 patients received NanOss. Fusions were performed utilizing the Vertex/Rod/Eyelet System (Medtronic, Memphis, TN, USA) with braided titanium cables through the base of intact spinous processes (not lateral mass screws) cephalad and caudad to laminectomy defects. Fusion was documented by an independent neuroradiologist blinded to the study design, utilizing dynamic X-rays and two dimensional computed tomography (2D-CT) studies up to 6 months postoperatively, or until fusion or pseudarthrosis was confirmed at 1 year.
Results:
Vitoss and NanOss resulted in comparable times to fusion: 5.65 vs. 5.35 months. Dynamic X-ray and CT-documented pseudarthrosis developed in 2 of 72 Vitoss patients at one postoperative year (e.g. bone graft resorbed secondary to early deep wound infections), while none occurred in the 20 patients receiving NanOss.
Conclusion:
In this preliminary study combining cervical laminectomy/fusions, the time to fusion (5.65 vs. 5.35 months), pseudarthrosis (2.7% vs. 0%), and infection rates (2.7% vs. 0%) were nearly comparable sequentially utilizing Vitoss (72 patients) vs. NanOss (20 patients) as bone graft expanders.
Keywords: Autograft, beta-tricalcium phosphate, fusion/pseudarthrosis rates, instrumented fusion, NanOss bioactive, posterior cervical surgery, Vitoss
INTRODUCTION
Two successive prospective cohorts of patients underwent 1-3 level cervical laminectomies with 5-9 level posterior cervical fusions to address cervical spondylotic myelopathy (CSM) and/or ossification of the posterior longitudinal ligament (OPLL) [Figures 1–9]. Instrumentation included the Vertex/Rod/Eyelet System (Medtronic, Memphis, TN, USA) utilizing braided titanium cables (not lateral mass screws) placed through the base of remaining intact spinous processes. The postero-lateral fusion mass included: Lamina autograft, iliac crest autograft, bone marrow aspirate (BMA), and one of two sequentially administered bone graft expanders. The first cohort of 72 patients received Vitoss (Orthovita, Malvern, PA, USA), while the next cohort of 20 patients received NanOss Bioactive (Regeneration Technologies Corporation [RTI: Alachua, FL, USA]) [Figures 1–9]. We asked whether the two bone graft supplements would demonstrate comparable times to fusion, fusion rates (vs. pseudarthrosis), and infection rates [Table 1].
Figure 1.

This classical midline sagittal T2-weighted MR study showed a marked hyperintense signal in the cervical cord opposite the C5-C6 level and multilevel ventral and dorsolateral compression (shingling of laminae/ossification of the yellow ligament) particularly involving the C4-C5 and C5-C6 levels. This patient successfully underwent a laminectomy of C4, C5, C6 with posterior fusion C2-T2
Figure 9.
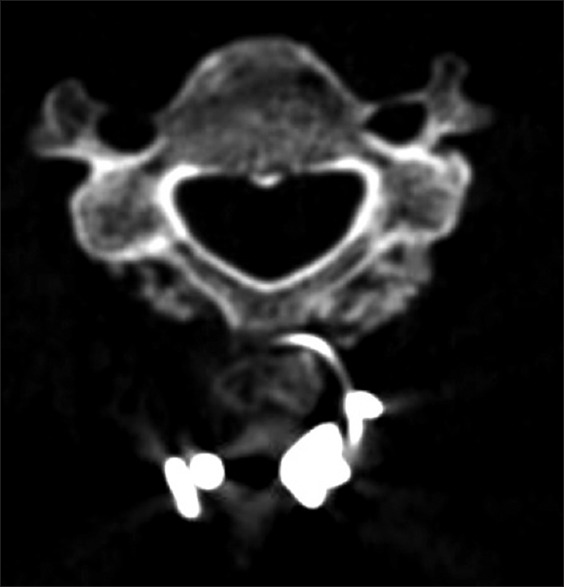
Six-month bone window 2D-CT study showing posterolateral fusion mass overlying the laminae and facet joints at the C6 level. Note the wire/rod complex involving the spinous process of C6
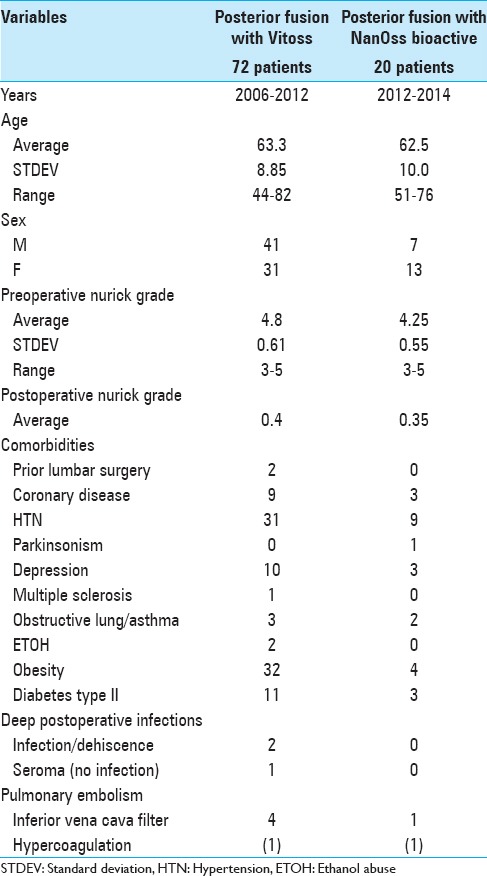
Table 1.
Surgical data for posterior cervical fusions utilizing Vitoss vs. NanOss bioactive
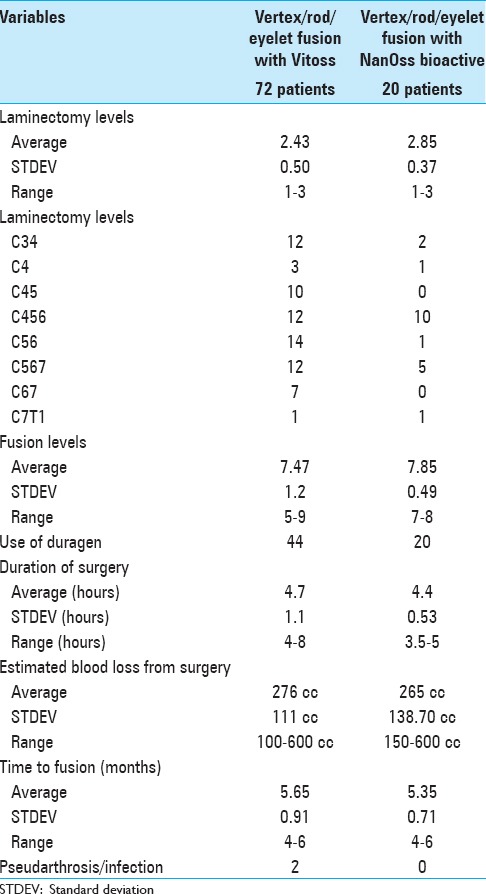
Figure 3.
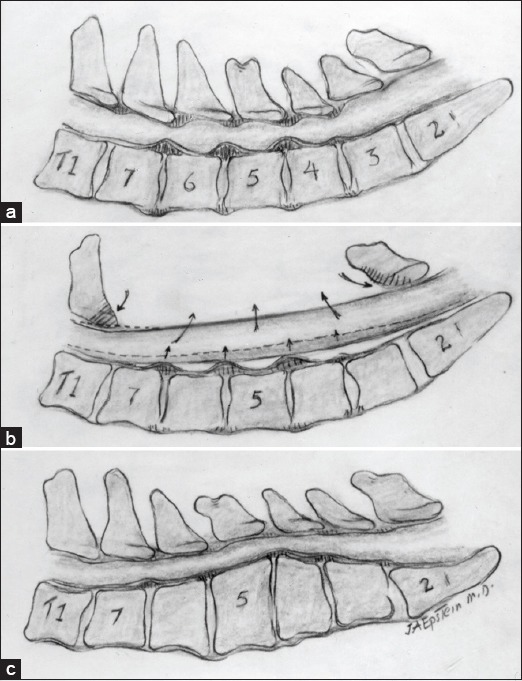
(a) A midline sagittal illustration of multilevel C3-C7 CSM accompanied by both ventral and dorso-lateral compression. (b) Cervical laminectomy C3-C7 for multilevel CSM in the presence of lordosis allows for dorsal cord migration away from ventrally situated osteophytes/pathology.(c) A laminectomy is contraindicated with kyphosis as the cord will fail to migrate posteriorly away from marked ventral compression
Figure 4.
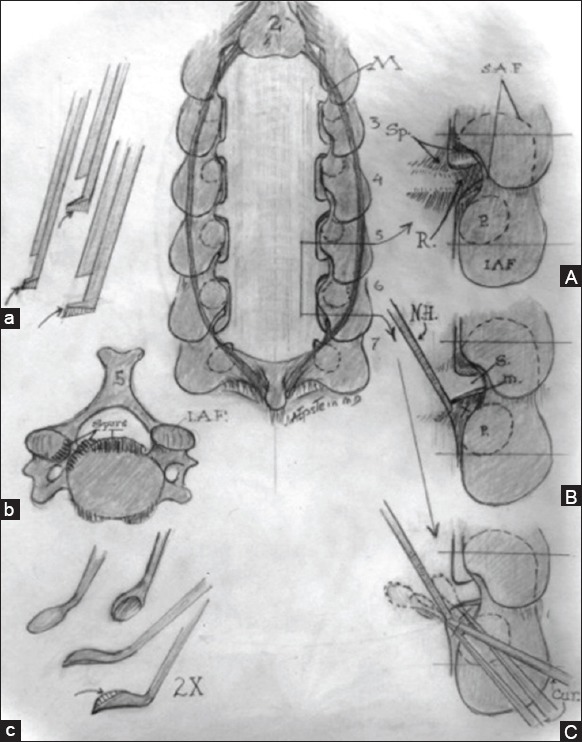
Midline Image: Cervical laminectomy C3-C7 is illustrated with medial facetectomy/foraminotomy performed at each intervening level. (a) Filed-down Kerrison punches for posterior cervical surgery. (b). Axial image of ventral cervical osteophyte (c). Down-biting curettes utilized for postero-lateral spur excision (A). Medial facetectomy/foraminotomy for exposure of the nerve root exiting at each level. (B). Use of a nerve hook to dissect/ gently retract the nerve root cephalad/medially in preparation for resection of underlying spur. (C). Use of down-biting curette to remove ventral spur
Figure 7.

This 6-month postoperative 2D-CT demonstrated the fusion mass dorsolateral to the facet joints/laminae of C7, T1, and T2
Figure 8.

Six-month parasagittal postoperative 2D-CT scan showing the fusion mass/facet fusion from C2-T2
MATERIALS AND METHODS
Vitoss
Vitoss, a form of beta tri-calcium phosphate (B-TCP), is synthetic cancellous bone graft substitute/bone void filler that is comprised of 39% calcium and 20% phosphorous, in a 1:5 ratio.[1,2,3,5] Vitoss’ porous, low-density construct is prepared by fusing nano particles of 100 nm in diameter that result in its increased microporosity (e.g. a scaffold that is 90% interconnected; pores ranging from 1 to 1000 microns) that increases fusion rates by facilitating infiltration, bone ingrowth, resorption, dissolution, and new bone formation [Figure 5].
Figure 5.
This 6-month postoperative posterior cervical 2D-CT documented the large fusion mass surrounding the distal intact laminae and spinous processes following the laminectomy of C4 with posterior fusion C2-T2
NanOss bioactive
NanOss’ nano-crystalline conformation (15–100 nm) mimics normal human bone crystals (25–500 nm) along with bone's composition/shape, while other calcium phosphate crystals are typically 1000–10,000 nm in size.[6,7] It is comprised of a highly purified porcine collagen that is ‘unwound’ to produce an extremely high surface area for the attachment of osteoclasts and osteoblasts. Its manufactured extracellular matrix-bioscaffold facilitates cell infiltration/ostoconduction, and fusion, and the open scaffold optimizes bone mineralization/remodeling [Figures 6–9].
Figure 6.

This parasaggital 2D-CT scan obtained 6 months postoperatively documented bone deposition extending posterolaterally from C2-T2. Also noted was the instrumentation affixed to the spinous processes of C2, C3; this was extended to involve the C7, T1, and T2 spinous processes as well
Cervical laminectomy and posterior cervical fusions sequentially utilizing two bone graft supplements
In this series, one surgeon performed 92 consecutive 1-3 level laminectomies with posterior Vertex/Rod/Eyelet fusions (5-9 levels). These procedures utilized titanium cables placed through intact cephalad/caudad spinous processes, but no lateral mass screws (e.g. not Food and Drug Administration approved at the time) [Table 1]. The fusion mass for the first sequential cohort of 72 patients included lamina autograft, iliac crest autograft, BMA, and Vitoss (2006-2011) [Figure 5]. The second sequential cohort of 20 patients underwent the same procedures, but instead received the alternate bone graft supplement, NanOss Bioactive (2012–2014) [Figures 6–9].
Similar clinical parameters for the patient populations receiving vitoss vs. NanOss
Clinical parameters were similar for both patient populations undergoing cervical laminectomies/posterior cervical fusions with Vitoss or NanOss to address multilevel CSM and/or OPLL documented on both magnetic resonance (MR) imaging and computed tomography (CT) studies [Figures 1 and 2 and Table 2]. The average ages were, respectively, 63.3 (Vitoss) and 62.5 (NanOss), and they had similar preoperative Nurick Grades (4.8 vs. 4.25) consistent with moderate/severe myelopathy, and postoperative neuorological improvement. Although the latter NanOss patients required slightly more extensive surgery (e.g. laminectomy [2.43 vs. 2.85 levels] and fusion [7.47 vs. 7.85 levels]), the average duration of surgery and average estimated blood loss (EBL) were nearly comparable [Table 2].
Figure 2.

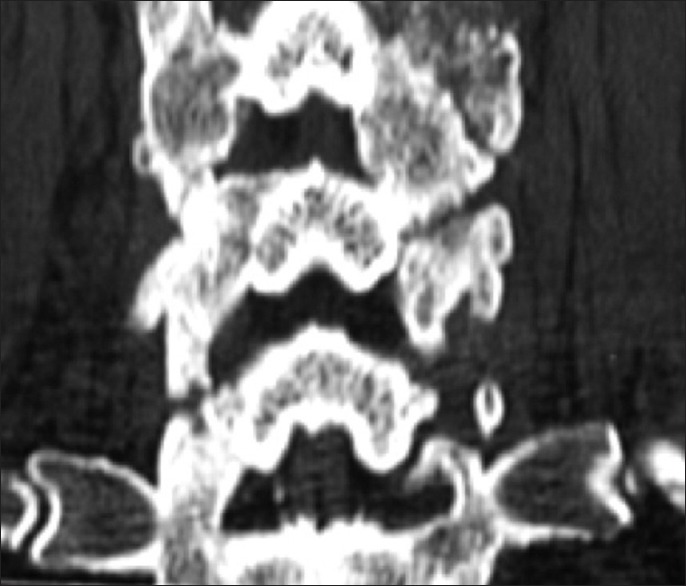
This classical midline sagittal 2D-CT study documents marked spinal stenosis with CSM accompanied by ventral OPLL (segmental behind the vertebral bodies of C4, C5, C6 with punctate ossification) and marked dorsolateral laminar shingling (e.g., C4, C5, C6 and the leading edge of C7). This patient's myelopathy resolved following a laminectomy of C4-C6 with undercutting of C3 and C7 and posterior C2-T2 fusion
Table 2.
Clinical data for posterior cervical fusions utilizing Vitoss vs. NanOss bioactive
Surgery
One to three level laminectomies (e.g. including bilateral medial facetectomy/foraminotomies) were performed under an operating microscope utilizing diamond drills and small 1–2 mm Kerrison rongeurs to remove lateral bone. This was followed by 5-9 level (e.g. typical C2-T2) Vertex/Rod/Eyelet fusions performed utilizing braded titanium cables (no lateral mass screws) passed through the base of intact cephalad/caudad spinous processes.
Similar techniques for applying 2.5 × 10 cm strips of vitoss vs. Nanoss over residual/intact laminae/facets to complete the fusion
Each product comes in a 10 × 2.5 cm sheet, which is soaked in 10 cc of iliac crest BMA. Each sheet is then cut into ¼ longitudinal strips. Next, decortication is performed over the lateral aspect of the facets and residual laminae at the laminectomy site, followed by decortication of the cephalad/caudad intact laminae/facet joints. Next, very small (morcellated) cancellous iliac crest bone chips are applied laterally at the laminectomy site (over the residual laminae and facets); dorsal to the autograft, 1/4 to 1/8 inch longitudinal strips of Vitoss or NanOss are placed to supplement the bone graft but avoid dural impingement. Finally, cancellous and cortical bone chips are applied over the intact laminae/facet joints, and followed by application of the remaining 1/4-inch strips. The dura is then covered with Duragen, and a medium Hemovac drain is placed in the epidural compartment.
Dynamic X-rays and two dimensional computed tomography documentation of fusion
All patients underwent dynamic X-rays at 3, 4.5, and 6 months postoperatively (or until fused) along with two dimensional computed tomography (2D-CT) (e.g. performed at 3 postoperative months and repeated later if needed) [Figures 5–9]. Studies were independently analyzed by two neuroradiologists blinded to the study design.
RESULTS
Fusion and pseudarthrosis rates
Patients in both the Vitoss and NanOss Groups demonstrated comparable times to fusion; 5.65 vs. 5.35 months postoperatively [Figures 5–9 and Tables 1 and 2]. Pseudarthrosis was only observed in 2 (2.8%) of 72 Vitoss patients who developed early deep wound infections resulting in graft resorption; both required operative debridement within a month of the original surgery. Later on (e.g. 6 months later), neither patient was sufficiently symptomatic from the pseudarthrosis to warrant secondary surgery. None in the NanOss group developed pseudarthrosis.
No other complications directly related to either bone graft expander
No other complication observed in either group was uniquely attributable to Vitoss or NanOss [Tables 1–3]. One patient who received Vitoss developed a sterile seroma 3 weeks postoperatively and required debridement; none were observed among those receiving NanOss. Three of the 72 Vitoss patients required inferior vena cava (IVC) filters for deep venous thrombosis (DVT)/pulmonary embolism (PE) vs. none in the NanOss group. Certainly the disparate size of the two populations must account for the variations for these two parameters.
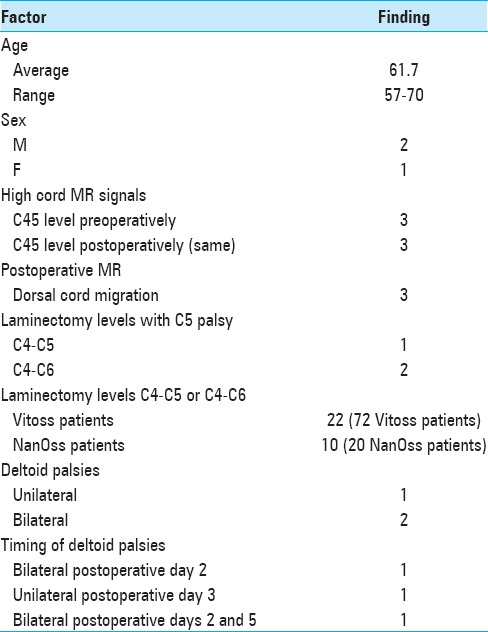
Table 3.
Factor common for 3 patients with C5 palsies
Three patients exhibiting delayed c5 root palsies
All procedures utilized intraoperative neural monitoring that included somatosensory-evoked potentials (SEP), electromyography (EMG), and motor-evoked potentials (MEP); no significant intraoperative changes occurred in any of the three cases where patients had delayed C5 palsies. Two C5 palsies occurred among the 72 receiving Vitoss, and one for the 20 patients receiving NanOss; none of these deficits were attributed to the bone graft expanders [Table 3]. In two patients, C5 palsies were bilateral (both on day 2 in one patient, on postoperative days 2 and 5, in the second patient); one was unilateral occurring on postoperative day 3. All patients had surgery involving the C4-C5 level; 1 patient had a C4-C5 laminectomy, while 2 had C4-C6 laminectomies; note that 22 of the 72 Vitoss patients and 10 of the 20 NanOss patients had laminectomies at the C4-C5 or C4-C6 levels [Table 3]. Immediate postoperative MR studies in all three patients demonstrated hyperintense cord signals noted opposite the C45 or C4-C6 levels similar to the preoperative studies, plus the anticipated dorsal cord migration (also seen comparably in patients without C5 palsies). The use of Vitoss vs. NanOss did not differentially impact the frequency of C5 palsies.
DISCUSSION
Data for vitoss bone graft expander for lumbar posterolateral fusions
Two series documenting instrumented posterolateral lumbar fusion rates utilizing vitoss
Epstein documented the frequency of successful instrumented posterolateral lumbar fusions (PLF) utilizing Vitoss to supplement autograft/BMA.[1] Epstein's 2006 study preliminarily evaluated the efficacy of Vitoss combined with lamina autograft (50:50 mix) and BMA to perform 40 multilevel lumbar laminectomies (average 3.7 levels) with one (27 patients) or two level (13 patients) instrumented fusions. Dynamic X-rays and 2D-CT studies documented fusion at six postoperative months in 26 of 27 single level fusions (1 pseudarthrosis), and 11 of 13 two level fusions (L4-S1) (2 pseudarthroses); only one of the latter patients required a secondary arthrodesis. Subsequently, in 2009, Epstein again utilized Vitoss with lamina autograft and BMA to perform 100 posterolateral lumbar-instrumented fusions similarly documented with both dynamic X-rays and 2D-CT (e.g. from 3 to 12 months postoperatively).[3] For 79 patients undergoing one-level instrumented fusions, 74 (93.7%) fused “early” (average 6.5 postoperative months), 2 (2.5%) fused “late” (average 6.5–12 months), while 3 (3.8%) exhibited pseudarthrosis. Two-segment arthrodesis in 21 patients yielded 14 (66.7%) “early” fusions, 5 (23.8%) “late” fusions, and 2 (9.5%) pseudarthroses. Chi-square analyses revealed a significant increase in the number of “late” radiographic fusions for two-level arthrodeses, but no significant difference in pseudarthrosis rates between the two groups.
Fusion rates utilizing vitoss for non-instrumented posterolateral lumbar fusion
In 2008, Epstein utilized Vitoss with lamina autograft and BMA to perform 60 multilevel laminectomies (average 5.8 levels) with 1- to 2-level noninstrumented PLF) in patients averaging 70 years of age.[2] Pseudarthrosis was documented in nine (15%) patients utilizing both dynamic X-rays and 2D-CT studies performed from 3 to 12 months postoperatively. Only one patient required secondary surgery; he was one of the youngest in the series with moderate osteoporosis and extensive cardiovascular disease that had previously required long-term aspirin use along with the early reinstitution of postoperative aspirin prophylaxis.
Level-1 pilot evaluation of vitoss/B-TCP as graft extender for posterior adolescent idiopathic scoliosis surgery
Lerner et al. compared the clinical/radiographic results for utilizing Vitoss/B-TCP vs. autogenous iliac crest bone graft (ICBG) in a prospective randomized scoliosis pilot study (EBM-Level 1).[5] Forty patients with adolescent idiopathic scoliosis (AIS) were randomized into: 20 ICBG vs. 20 Vitoss/B-TCP. With an average postoperative follow-up of 20 postoperative months, only one patient in the Vitoss group had a pseudarthrosis. The authors concluded that Vitoss with local bone graft resulted in equal fusion rates when compared with the utilization of local bone graft and ICBG.
Bone morphogenetic protein and calcium phosphate salts for posterolateral lumbar fusion
Kaiser et al. proposed the use of local laminectomy autograft, calcium-phosphate salts, and bone morphogenetic proteins (BMPs) to supplement iliac autograft/local autograft for lumbar interbody fusions.[4] Although they observed comparable fusion rates using this construct, they noted that the literature increasingly cites concern regarding BMPs reported risks of heterotopic bone formation.
NanOss: Nanocrystalline hydroxyapatite most comparable to normal bone vs. Vitoss
MacMillan et al. compared osteoblast and osteoclast activity for NanOss Bioactive (e.g. nanocrystalline hydroxyapatite [HA]; nanomaterials <100 nm; porous low crystalline nano-HA, B-TCP [RTI Surgical Corporation]) vs. other micron crystalline ceramics (e.g. calcium phosphate products; HA, and biphasic calcium phosphates [TCP/HA], porous micron-TCP [Vitoss; Stryker, Corporation, Kalamazoo MI, USA], various types of nanoceramics).[6] Focusing on improved bone formation utilizing nanoceramics (NanOss) vs. micron ceramics, they demonstrated similar osteoblast and osteoclast activity for NanOss and normal bone, while micron crystalline HA products were not as effective. They further observed that NanOss resulted not only in increased bone growth and reduced pseudarthrosis rates, but also correlated with lesser implant infection/inflammation rates.
A comparison of nanoss, autograft, and actifuse (baxter corporation franklin lakes, NJ, USA) in a rabbit posterolateral fusion model (nass meeting, 2009)
In 2009, Hill and Walsh (presentation North American Spine Society [NASS] Meeting 2009) observed that NanOss offers a high surface area for osteoblastic adhesions, proliferation, and bone mineralization in-vitro and in in-vivo animal models. They cited the surface areas of several different compounds: NanOss 70 m2/g, human bone 20–100 m2/g, Vitoss 0.3 m2/g, Actifuse 0.26 m2/g. While most collagen carriers utilize a triple helix structure, NanOss separates these strands providing more sites for cell infiltration/attachments and bone formation. They presented the data for PLF at the L5-L6 levels in rabbits and followed them with a combination of: Biomechanical testing, X-rays, CT, and histology. At 8 and 12 postoperative weeks, CT studies documented greater fusion for NanOss vs. Actifuse vs. Autograft, along with greater biomechanical strength/stiffness. Histology also revealed larger and more ossified/fused posterolateral fusion masses with NanOss vs. the other constructs. Again in 2012, Walsh et al. confirmed greater L5-L6 PLF in rabbits at 6, 12, and 26 weeks using similar testing parameters with comparable products (Orthopedic Research Society Meeting 2012) for NanOss with BMA/autograft vs. Vitoss BA/BMA vs. autograft/BMA.
Use of Nanocrystalline hydroxyapatite with autologous BMA and local bone in the lumbar spine. a retrospective CT of PLF
Robbins et al. performed a retrospective multicenter 1-year review of postoperative CT studies in 46 patients (average age 58.6) undergoing instrumented 1-3 segment PLF utilizing autograft, BMA, and NanOss.[7] Of interest, comorbid factors included: Obesity (19 patients), hypertension (HTN) (4 patients), Type II DM (2 patients), smoking (6 patients), steroid use (1 patient), and osteopenia (3 patients). Fusion (bridging bone) was documented over the transverse processes in 94% of patients either unilaterally/bilaterally; fusion rates for 1-3 segments were 88%, 93%, and 100%, respectively. Six percent of segments showed no fusion. Notably, there were no complications related to the use of NanOss. The authors concluded “arthrodesis rates after instrumented lumbar fusion using local autograft mixed with BMA and the NanOss hydroxyapatite (nHA) is equivalent to the rates reported for iliac crest autograft”.
Comparable posterior cervical fusion rates utilizing vitoss vs. NanOss to supplement iliac crest bone graft and bone marrow aspirate
Posterior cervical instrumented fusion rates in this series were comparable for two sequential populations of patients undergoing 1-3 level cervical laminectomy with posterior instrumented fusions (5-9 levels). Fusion masses were comprised of lamina/iliac crest autograft (ICBG) and BMA supplemented with one of two bone graft expanders. The first cohort of 72 patients received Vitoss, while the second cohort of 20 patients received NanOss. The time to fusion for both groups, documented utilizing dynamic X-ray and 2D-CT studies were comparable (5.65 vs. 5.35 months) [Table 2]. The different size of the two populations (e.g. only 20 patients in the latter sample) likely accounted for the disparity in the number of infections and pseudarthroses; 2 (2.8%) of 72 Vitoss patients exhibited infection with pseudarthrosis vs. 0 infections or pseudarthroses for the 20 NanOss patients. The frequency of postoperative seromas (1 patient receiving Vitoss), 3 DVT/PE (all Vitoss patients), and C5 palsies (2 Vitoss, 1 NanOss patients) could not be attributed to either bone graft expander. Due to the preliminary documentation of the comparable efficacy of Vitoss vs. NanOss for performing posterior cervical fusions following multilevel laminectomies, and its easy handling (e.g. thinner sheets/easier packing), it will be utilized for these procedures in the future.
Contraindications for using NanOss
Contraindication to the use of NanOss include: Metabolic/systemic bone disorders negative impacting bone or wound healing, factures without stabilization, vascular impairment or graft site, infection (acute/chronic)/contamination, impaired calcium metabolism, steroid use, immunosuppression, use in open epiphyseal growth plates, and allergy to porcine collagen products.
Footnotes
Available FREE in open access from: http://www.surgicalneurologyint.com/text.asp?2015/6/5/164/156559
REFERENCES
- 1.Epstein NE. A preliminary study of the efficacy of Beta Tricalcium Phosphate as a bone expander for instrumented posterolateral lumbar fusions. J Spinal Disord Tech. 2006;19:424–9. doi: 10.1097/00024720-200608000-00009. [DOI] [PubMed] [Google Scholar]
- 2.Epstein NE. An analysis of noninstrumented posterolateral lumbar fusions performed in predominantly geriatric patients using lamina autograft and beta tricalcium phosphate. Spine J. 2008;8:882–7. doi: 10.1016/j.spinee.2007.11.005. [DOI] [PubMed] [Google Scholar]
- 3.Epstein NE. Beta tricalcium phosphate: Observation of use in 100 posterolateral lumbar instrumented fusions. Spine J. 2009;9:630–8. doi: 10.1016/j.spinee.2009.04.007. [DOI] [PubMed] [Google Scholar]
- 4.Kaiser MG, Groff MW, Watters WC, 3rd, Ghogawala Z, Mummaneni PV, Dailey AT, et al. Guideline update for the performance of fusion procedures for degenerative disease of the lumbar spine. Part 16: Bone graft extenders and substitutes as an adjunct for lumbar fusion. J Neurosurg Spine. 2014;21:106–32. doi: 10.3171/2014.4.SPINE14325. [DOI] [PubMed] [Google Scholar]
- 5.Lerner T, Bullmann V, Schulte TL, Schneider M, Liljenqvist U. A level-1 pilot study to evaluate of ultraporous beta-tricalcium phosphate as a graft extender in the posterior correction of adolescent idiopathic scoliosis. Eur Spine J. 2009;18:170–9. doi: 10.1007/s00586-008-0844-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.MacMillan AK, Lamberti FV, Moulton JN, Geilich BM, Webster TJ. Similar healthy osteoclast and osteoblast activity on nanocrystalline hydroxyapatite and nanoparticles of tri-calcium phosphate compared to natural bone. Int J Nanomedicine. 2014;9:5627–37. doi: 10.2147/IJN.S66852. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Robbins S, Lauryssen C, Songer MN. Use of Nanocrystalline Hydroxyapatite with Autologous BMA and Local Bone in the Lumbar Spine. A Retrospecrtive Ct Analysis of Posterolatearl Fusion Results. J Spinal Disord Tech. 2014 Feb 27; doi: 10.1097/BSD.0000000000000091. (EPUB ahead of print) [DOI] [PMC free article] [PubMed] [Google Scholar]