

Abstract
Understanding more about the clinical presentations encountered in veterinary practice is vital in directing research towards areas relevant to practitioners. The aim of this study was to describe all problems discussed during a convenience sample of consultations using a direct observation method. A data collection tool was used to gather data by direct observation during small animal consultations at eight sentinel practices. Data were recorded for all presenting and non-presenting specific health problems discussed. A total of 1901 patients were presented with 3206 specific health problems discussed. Clinical presentation varied widely between species and between presenting and non-presenting problems. Skin lump, vomiting and inappetence were the most common clinical signs reported by the owner while overweight/obese, dental tartar and skin lump were the most common clinical examination findings. Skin was the most frequently affected body system overall followed by non-specific problems then the gastrointestinal system. Consultations are complex, with a diverse range of different clinical presentations seen. Considering the presenting problem only may give an inaccurate view of the veterinary caseload, as some common problems are rarely the reason for presentation. Understanding the common diagnoses made is the next step and will help to further focus questions for future research.
Keywords: Clinical practice, Companion animals, Epidemiology, Evidence-based medicine, Veterinary profession, Small animals
Introduction
When prioritising topics for future clinical veterinary research, it is vital to understand which problems veterinary surgeons spend their time trying to diagnose and manage. Various studies have looked at the nature of the problems with which small animal patients are presented to the veterinary surgeon. Lund and others (1999) analysed data extracted from clinical records and found that dental calculus, followed by gingivitis, were the most common clinical presentations. Other studies have found skin and ear problems to be amongst the most common problems (Evans and others 1974, Robotham and Green 2004, O'Neill and others 2014), suggesting some inconsistency in the most common problems identified. The methods used during these studies included questionnaires (Evans and others 1974, Robotham and Green 2004) and clinical coding alongside extraction of data from the clinical records (Lund and others 1999, O'Neill and others 2014) and it is currently unclear whether these methods are able to capture data on all problems addressed during the consultation. Previous research has suggested discussion of multiple different problems during a single consultation is common and that a direct observation method is well equipped to capture this complexity (Robinson and others 2014). Considering all problems discussed is crucial, as this will ensure problems which are common yet rarely the reason for presentation are not neglected when setting research priorities. Examining the veterinary caseload in more depth may also have implications for veterinary curricula, as the results could be used to ensure graduates are adequately prepared for the clinical presentations they will encounter in first opinion practice. Understanding common presentations will also be useful for veterinary practices when making decisions surrounding in-house training, continuing professional development (CPD), designated clinics (eg, weight clinics) and which equipment to invest in. Veterinary practitioners could use the results to structure history-taking and clinical examination in each species based on the most common clinical signs and clinical examination findings.
The aim of this study was to describe the clinical presentation of all specific health problems (presenting and non-presenting) discussed during a convenience sample of small animal consultations using a direct observation method.
Materials and methods
Practice selection
A convenience sample of eight first opinion veterinary sentinel practices was recruited to the study. These were practices which had either been involved in a previous practice-based research project (Dean and others 2013) or who had expressed an interest in being involved in practice-based research with the Centre for Evidence-based Veterinary Medicine (CEVM).
Data collection tool
Development of the tool
A data collection tool was developed to allow the collection of complex data by direct observation during small animal consultations at participating practices. The tool consisted of a series of open and closed questions on a paper form and was able to gather data on signalment of the animal(s) presented, clinical signs reported, clinical examination findings, body system(s) affected, diagnoses made and outcome of the consultation. The tool was initially developed in Microsoft Office Word 2010 then transferred to Cardiff Teleform V.10.5.1 (Verity, Cambridge). Completed forms could then be scanned and verified in Teleform, then exported to a Microsoft Office Access 2010 database for analysis. Following initial development of the tool, pretest and pilot studies were conducted between August 2010 and March 2011, to ensure that the methods used were feasible in a first opinion practice setting. The pretest consisted of a single half day each at two of the sentinel practices, while the pilot study involved a full day at each of the eight practices. An inter-rater reliability study of the tool was carried out in May 2012. Development, testing and utilisation of the data collection tool have been previously reported (Robinson and others 2014). Data were collected during two separate one week periods at each of the eight sentinel practices between April 2011 and June 2012. The primary investigator directly observed consultations by a number of different vets during regular weekday consulting hours. Where multiple veterinary surgeons were consulting simultaneously, selection of the consultation stream to observe was based on convenience and feasibility (eg, consult room size), however an effort was made to ensure some time was spent observing each veterinary surgeon during the data collection period. Animals which presented more than once during the data collection period were included each time they presented. Due to their sensitive nature, elective euthanasia consultations were often not fully observed, so data from these consultations were often incomplete.
Problems
A problem was defined as ‘any two-way discussion between owner/carer and vet regarding any aspect of the patient's health and wellbeing’ in order to include issues relating to preventive medicine as well as specific health problems. Preventive medicine problems included vaccination, preventive treatment for parasites, microchipping, neutering advice and routine health checks. Data on specific health problems only are reported in this paper and preventive medicine problems will be considered in a separate publication (Robinson 2014). The reason for presentation (or the first problem mentioned where this was not explicitly stated) as stated by the owner, was considered to be the ‘presenting problem’; each additional problem discussed after this was considered to be a ‘non-presenting problem’. For each patient, only one presenting problem could be recorded, however several non-presenting problems could be recorded.
A combination of closed and open fields was used by a single observer to record data on the clinical presentation for each problem discussed. Clinical presentation was defined as consisting of four different components: problem type; clinical signs; clinical examination findings; body system. Each specific health problem was summarised by coding to a problem type developed by the first author (one selected from: new problem; pre-existing problem; elective euthanasia (see online supplementary appendix 1)). This could usually be ascertained by direct observation of the consultation alone, however where there was uncertainty the clinical records were checked following the consultation. Where possible specific clinical sign terms (eg, cough, halitosis, etc) were recorded for each specific health problem discussed. These specific clinical signs were those which were mentioned by the owner during the consultation, either voluntarily or in response to questions from the veterinary surgeon. Multiple clinical signs could be recorded for each specific health problem discussed.
A closed field was used to record whether there were any clinical examination findings, with an option to select ‘not applicable’ for cases where no clinical examination was performed. An open field was used to record specific clinical examination findings and multiple findings could be recorded for each specific health problem discussed. The body system affected by each specific health problem was recorded and up to two body systems could be selected per specific health problem where necessary (see online supplementary appendix 1). Where more than two body systems were affected, for example by a systemic disease (eg, feline infectious peritonitis or obesity), or where the body system(s) affected were unclear (eg, a cat with pyrexia of unknown origin), the non-specific body system category was selected.
All coding of clinical signs and clinical examination findings at the data entry stage were carried out by the primary investigator. To ensure consistent coding, records were kept detailing how cases were coded, which could be referred back to when coding subsequent similar cases to ensure the same terminology was used. Where queries arose surrounding the categorisation and coding of data, discussions with colleagues in the CEVM and veterinary surgeons in sentinel practices were used to decide how data should be coded. A record was kept of these discussions to ensure similar cases were coded in the same way.
Statistical analysis
Descriptive statistics were generated using IBM SPSS V.21, with pivot tables used to generate frequency data for all variables analysed. For each variable, data were generated for all specific health problems discussed, presenting problems only, non-presenting problems only and for the three most frequently presented species (dog, cat and rabbit). The chi-square test was used to determine whether the body system affected varied between presenting and non-presenting problems and between the three most frequently presented species. Only the 10 most frequently affected body systems across all problems were included in this analysis. Statistical significance was set at the 0.05 level.
Ethical approval
Approval was obtained from the ethics committee at the School of Veterinary Medicine and Science, The University of Nottingham for the collection of data through direct observation, and subsequent analysis of this data. Details of how informed consent was obtained and data anonymised have been detailed in a previous paper (Robinson and others 2014).
Results
Over the 16 weeks of data collection, data were collected from 1720 consultations conducted by 62 veterinary surgeons involving 1901 patients. For the 1901 patients presented, data were collected on 3206 specific health problems of which 1211 were presenting problemsi and 1995 were non-presenting problems, giving a ratio of 1:1.65 (presenting: non-presenting specific health problems).
Problem type
The number of specific health problems to be considered are summarised in the flow chart in Fig 1, alongside the number of specific health problems for the three most frequently presented species. New problems accounted for over half of all specific health problems (n=1685/3206; 52.6 per cent), while pre-existing problems accounted for just under half (n=1492/3206; 46.5 per cent). Presenting problems had proportionally fewer new problems (n=480/1211; 39.6 per cent) and more pre-existing problems (n=704/1211; 58.1 per cent). For non-presenting problems the number of new problems (n=1205/1995; 60.4 per cent) exceeded the number of pre-existing problems (n=788/1995; 39.5 per cent). In total 29 problems related to elective euthanasia, all of which were presenting problems.
FIG 1:
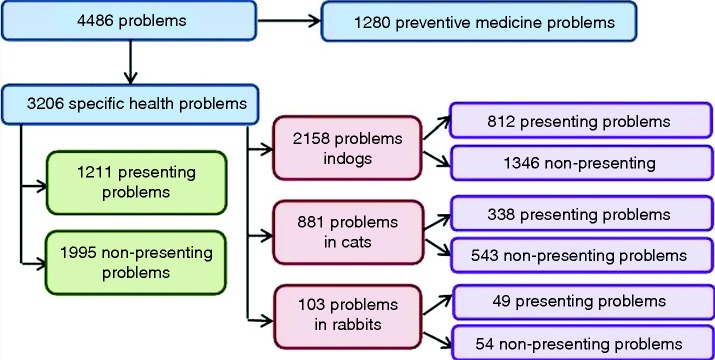
The total number of problems discussed and number of presenting and non-presenting specific health problems discussed for each species, during direct observation of small animal consultations
Clinical signs
The most common clinical signs overall were skin lump (n=151; 4.7 per cent) followed by vomiting (n=130; 4.1 per cent) then inappetence (n=124; 3.9 per cent) (Table 1a). The 10 most frequently recorded clinical signs varied between presenting and non-presenting problems. Some clinical signs, such as weight loss and lameness were common for both presenting and non-presenting problems. Others were common only for presenting problems (eg, pain and pruritus) or only for non-presenting problems (eg, overweight/obese and behavioural problem) (Table 1a). Clinical signs varied between species (Table 1b) with skin lump the most common sign in dogs (n=125; 5.8 per cent), vomiting in cats (n=54; 6.1 per cent) and inappetence in rabbits (n=13; 12.6 per cent). Some clinical signs, such as inappetence and overweight/obese, were commonly mentioned for all three of the most frequently presented species, but many, such as lameness in dogs, lethargy in cats and matted fur in rabbits, were only amongst the most common clinical signs for one species.
TABLE 1:
The 10 most frequently recorded clinical signs for (a) all problems, presenting problems and non-presenting problems and (b) the three most frequently presented species, during direct observation of small animal consultations
| (a) | ||||||||
|---|---|---|---|---|---|---|---|---|
| All problems (n=3206) |
Presenting problems (n=1211) |
Non-presenting problems (n=1995) |
||||||
| Clinical sign | n | Per cent * | Clinical sign | n | Per cent* | Clinical sign | n | Per cent* |
| Skin lump | 151 | 4.7 | Inappetence | 103 | 8.5 | Skin lump | 103 | 5.2 |
| Vomiting | 130 | 4.1 | Vomiting | 75 | 6.2 | Overweight/obese | 94 | 4.7 |
| Inappetence | 124 | 3.9 | Lameness | 75 | 6.2 | Vomiting | 55 | 2.8 |
| Lameness | 106 | 3.3 | Diarrhoea | 64 | 5.3 | Polydipsia | 49 | 2.5 |
| Diarrhoea | 104 | 3.2 | Lethargic | 57 | 4.7 | Weight loss | 46 | 2.3 |
| Weight loss | 100 | 3.1 | Weight loss | 54 | 4.5 | Diarrhoea | 40 | 2.0 |
| Overweight/obese | 94 | 2.9 | Pruritus | 53 | 4.4 | Ocular discharge | 39 | 2.0 |
| Polydipsia | 90 | 2.8 | Skin lump | 48 | 4.0 | Behavioural problem | 38 | 1.9 |
| Pruritus | 82 | 2.6 | Polydipsia | 41 | 3.4 | Weight gain | 33 | 1.7 |
| Ocular discharge | 73 | 2.3 | Pain | 40 | 3.3 | Lameness | 31 | 1.6 |
| (b) | ||||||||
|---|---|---|---|---|---|---|---|---|
| Dog (n=2158) |
Cat (n=881) |
Rabbit (n=103) |
||||||
| Clinical sign | n | Per cent* | Clinical sign | n | Per cent* | Clinical sign | n | Per cent* |
| Skin lump | 125 | 5.8 | Vomiting | 54 | 6.1 | Inappetence | 13 | 12.6 |
| Lameness | 85 | 3.9 | Weight loss | 53 | 6.0 | Ocular discharge | 9 | 8.7 |
| Diarrhoea | 78 | 3.6 | Inappetence | 51 | 5.8 | Matted fur | 6 | 5.8 |
| Vomiting | 76 | 3.5 | Polydipsia | 36 | 4.1 | Overweight/obese | 6 | 5.8 |
| Pruritus | 71 | 3.3 | Ocular discharge | 25 | 2.8 | Dragging limb | 5 | 4.9 |
| Overweight/obese | 65 | 3.0 | Lethargy | 23 | 2.6 | Overgrown incisors | 5 | 4.9 |
| Polydipsia | 52 | 2.4 | Overweight/obese | 23 | 2.6 | Ataxia | 4 | 3.9 |
| Licking feet | 50 | 2.3 | Diarrhoea | 21 | 2.4 | Dental abnormality | 3 | 2.9 |
| Inappetence | 47 | 2.2 | Fussy with food | 21 | 2.4 | Scabs | 3 | 2.9 |
| Weight loss | 43 | 2.0 | Haematuria | 21 | 2.4 | Weight loss | 3 | 2.9 |
*Percentages shown are based on the total number of problems for each problem type or species
Clinical examination findings
Data on clinical examination findings were recorded for 3042 (94.9 per cent) of the 3206 problems, of which 1098 were presenting problems and 1944 were non-presenting problems. Of the 164 problems for which clinical examination findings were not recorded, 153 were discussed during consultations where the animal did not receive a clinical examination and the remaining 11 were problems discussed during elective euthanasia consultations where not all data could be recorded.
Of the 3042 problems for which the patient did receive a clinical examination, 2134 (70.2 per cent) had at least one finding related to that problem on clinical examination. Overweight/obese was the most common finding overall (n=202; 6.6 per cent) followed by dental tartar (n=171; 5.6 per cent) then skin lump (n=159; 5.2 per cent). Overweight/obese (n=199; 10.2 per cent), dental tartar (n=162; 8.3 per cent) and skin lump (n=108; 5.6 per cent) were also the most common findings for non-presenting problems. For presenting problems, lameness was the most common finding (n=64; 5.8 per cent) followed by erythema (n=61; 5.6 per cent) and wound (n=61; 5.6 per cent) (Table 2a).
TABLE 2:
The 10 most frequently recorded clinical examination findings for (a) all problems, presenting problems and non-presenting problems and (b) the three most frequently presented species, during direct observation of small animal consultations
| (a) | ||||||||
|---|---|---|---|---|---|---|---|---|
| All problems (n=3042) |
Presenting problems (n=1098) |
Non-presenting problems (n=1944) |
||||||
| Finding | n | Per Cent* | Finding | n | Per Cent* | Finding | n | Per Cent* |
| Overweight/obese | 202 | 6.6 | Lameness | 64 | 5.8 | Overweight/obese | 199 | 10.2 |
| Dental tartar | 171 | 5.6 | Skin erythema | 61 | 5.6 | Dental tartar | 162 | 8.3 |
| Skin lump | 159 | 5.2 | Wound | 61 | 5.6 | Skin lump | 108 | 5.6 |
| Weight loss | 152 | 5 | Pyrexia | 60 | 5.5 | Weight loss | 92 | 4.7 |
| Weight gain | 100 | 3.3 | Weight loss | 60 | 5.5 | Weight gain | 87 | 4.5 |
| Wound | 94 | 3.1 | Skin lump | 51 | 4.6 | Heart murmur | 81 | 4.2 |
| Skin erythema | 89 | 2.9 | Alopecia | 37 | 3.4 | Ocular discharge | 43 | 2.2 |
| Heart murmur | 87 | 2.9 | Ocular discharge | 36 | 3.3 | Alopecia | 35 | 1.8 |
| Ocular discharge | 79 | 2.6 | Inflamed ear | 35 | 3.2 | Waxy ear | 35 | 1.8 |
| Lameness | 77 | 2.5 | Thin | 32 | 2.9 | Gingivitis | 34 | 1.7 |
| (b) | ||||||||
|---|---|---|---|---|---|---|---|---|
| Dog (n=2056) |
Cat (n=832) |
Rabbit (n=97) |
||||||
| Finding | n | Per Cent* | Finding | n | Per Cent* | Finding | n | Per Cent* |
| Overweight/obese | 141 | 6.9 | Weight loss | 86 | 10.3 | Ocular discharge | 10 | 10.3 |
| Skin lump | 133 | 6.5 | Dental tartar | 58 | 7.0 | Overgrown incisors | 10 | 10.3 |
| Dental tartar | 110 | 5.4 | Overweight/obese | 48 | 5.8 | Overweight/obese | 10 | 10.3 |
| Skin erythema | 73 | 3.6 | Wound | 47 | 5.6 | Weight loss | 9 | 9.3 |
| Lameness | 65 | 3.2 | Weight gain | 42 | 5.0 | Matted fur | 7 | 7.2 |
| Weight loss | 56 | 2.7 | Heart murmur | 37 | 4.4 | Scurf | 6 | 6.2 |
| Weight gain | 55 | 2.7 | Thin | 26 | 3.1 | Molar spurs | 4 | 4.1 |
| Waxy ear | 52 | 2.5 | Ocular discharge | 25 | 3.0 | Wound | 4 | 4.1 |
| Heart murmur | 49 | 2.4 | Alopecia | 23 | 2.8 | Ataxia | 3 | 3.1 |
| Inflamed ear | 44 | 2.1 | Gingivitis | 23 | 2.8 | Weight gain | 3 | 3.1 |
*Percentages shown are based on the total number of problems for each species or problem type (shown in the Total n column)
After exclusion of problems where clinical examination findings were not recorded, data were available for 2056 problems in dogs, 832 problems in cats and 97 problems in rabbits. Specific findings on clinical examination varied between the species, with overweight/obese most common in dogs (n=141; 6.9 per cent), weight loss in cats (n=86; 10.3 per cent) and ocular discharge, overgrown incisors and obese/overweight in rabbits (all n=10; 10.3 per cent) (Table 2b). As with clinical signs, while some clinical examination findings were common in all three species, many were amongst the most common findings in only one species, such as skin lump in dogs, wounds in cats and molar spurs in rabbits.
Body system
Data were available on the body system(s) affected for 3194 (99.6 per cent) of the 3206 problems. A single body system was recorded for 3072 problems (96.2 per cent) and two body systems were recorded for 122 problems (3.8 per cent). Of the 122 problems with dual body systems recorded, the five most common combinations were musculoskeletal/neurological (n=25); musculoskeletal/skin (n=12); cardiovascular/respiratory (n=12); dental/gastrointestinal (n=6) and urinary/renal (n=6). Skin was the most frequently affected body system for both presenting and non-presenting problems (Fig 2). Gastrointestinal problems and musculoskeletal problems were more common as presenting than non-presenting problems. Conversely, dental, behavioural and non-specific problems were more common as non-presenting than presenting problems. Body system affected also varied between species (Fig 3). Skin and musculoskeletal problems were more common in dogs than in cats and rabbits. Respiratory, endocrine and urinary problems accounted for a higher proportion of problems in cats than other species while dental, neurological and non-specific problems accounted for a higher proportion of problems in rabbits than in other species. Body system affected varied significantly between presenting and non-presenting problems (P<0.001) and between species (P<0.001).
FIG 2:

Body system affected by all problems, presenting and non-presenting problems discussed for all patients presented during direct observation of consultations. The non-specific category was selected for both systemic diseases or where the body system(s) affected was unclear. Chi-square analysis only included the 10 most frequently affected body systems across all problems, excluding reproductive, endocrine, urinary, renal and haemopoietic
FIG 3:

Body systems affected by all problems discussed for the three most frequently presented species during direct observation of small animal consultations. The non-specific category was selected for both systemic diseases or diseases where it was unclear which body system(s) were affected. Chi-square analysis only included the 10 most frequently affected body systems across all problems, excluding reproductive, endocrine, urinary, renal and haemopoietic
Discussion
The broad range of clinical signs, examination findings and affected body systems among the consultations observed supports previous findings which highlighted the complexity of the consultation (Robinson and others 2014). Presenting problems appear to be fundamentally different from non-presenting problems and it is unclear which should take precedence when prioritising topics for future research and education.
An extensive range of clinical signs and clinical examination findings were identified in first opinion practice and these appear to vary widely between different species. The findings could be used to help to focus future research by identifying the types of problems veterinary surgeons frequently encounter for each commonly presented species. Interestingly, many of the common clinical examination findings were those which could potentially be identified by owners. Some of these findings, for example skin lumps and lameness, were often also stated by owners as clinical signs. Others were mentioned by owners far less frequently, for example dental tartar and overweight/obese, particularly when compared with how often they were identified on clinical examination. This seemed to be a particular issue for problems affecting rabbits, with overweight/obese, weight loss, overgrown incisors and scurf all commonly identified on clinical examination, yet mentioned much less frequently by the owner. This suggests there could be an opportunity to educate owners as to how to identify these clinical problems along with the potential consequences of leaving such problems untreated. For example, demonstrating how to identify dental problems and check body condition could allow owners to detect these findings at home. This could lead to animals being presented at an earlier stage, allowing better treatment and management of some problems.
Clinical presentation also varied widely between presenting and non-presenting problems. If the reason for presentation alone were considered when examining caseload, some of the most frequently encountered clinical signs, clinical examination findings and body systems, such as overweight/obese, dental problems and behavioural problems would be missed. Many previously unidentified problems would also be missed as over half of the non-presenting problems discussed were also new problems. Understanding why these types of problems tend to be raised as additional problems may help when deciding how they should be prioritised. It may be that owners do not recognise these problems or do not see them as important. Davies (2011) conducted an online survey of pet owners through a pet health website and asked which clinical signs would prompt them to present a geriatric pet to a veterinary surgeon. Only 54.4 per cent would take their animal to the vet for obesity and only 52.3 per cent would present their animal for halitosis (often associated with dental disease) suggesting owners may not recognise the consequences of these problems. However those responding to the survey were likely to be computer-literate owners with an active interest in pet health so the respondents may not have been representative of all UK pet owners. It is also unclear whether health problems are likely to be prioritised in the same way by veterinary surgeons as by owners, or even whether the presenting problem always represents the owner's main concern. The next step in setting future research priorities could engage both practitioners and owners to ensure the needs of both parties are met. This has been done with great success in medicine by the James Lind Alliance (2014), who involve a combination of clinicians, patients and carers in the research prioritisation process.
Skin, musculoskeletal, gastrointestinal and dental problems were all common presentations in the current study, which is consistent with the findings of previous studies (Evans and others 1974, Lund and others 1999, Robotham and Green 2004, Hill and others 2006, O'Neill and others 2014). A wide range of different methods, including questionnaires (Evans and others 1974, Robotham and Green 2004), use of electronic patient records (Lund and others 1999, O'Neill and others 2014) and direct observation (Hill and others 2006) were used in these studies. Therefore this consistency in the main findings is encouraging, and suggests they may provide an accurate picture of the clinical presentations commonly seen in first opinion practice. Examining the diagnoses made during these consultations will help pinpoint specific diseases which are frequently encountered; this will be considered in a separate paper. However there were some problems, such as behavioural problems, which were frequently discussed during the consultations observed, yet have been identified as common in only one previous study (O'Neill and others 2014). This could in part be because the majority of behaviour problems were raised as non-presenting problems, so may be missed when using methods which cannot capture the full complexity of the consultation. There may also be a difference in veterinary surgeon attitudes towards behavioural problems compared with other specific health problems, perhaps leading to differences in the way these types of problems are recorded. Previous research has suggested that veterinary surgeons acknowledge behavioural problems to be a component of their caseload but often feel unprepared for dealing with such problems and unable to meet client expectations (Roshier and McBride 2013). It should be remembered that when prioritising questions for future research, the frequency of a clinical presentation is not the only important factor to consider. Identifying knowledge gaps in the evidence surrounding a particular topic by looking at the amount and quality of existing literature is also important, as is taking into account the information needs of practitioners. Ebell and others (2013) recorded the clinical questions encountered by small animal veterinary surgeons, and found that the most common body system mentioned was endocrine, suggesting the information needs of practitioners was high for these types of problems. This is surprising as relatively few endocrine problems were recorded in the current study, though this could in part be due to the relatively small sample of practices and consultations observed. It may be that some health problems present a particular challenge to practitioners and so need to be prioritised over more common problems.
In addition to assisting researchers in prioritising research topics, awareness of the veterinary caseload will also be useful in directing undergraduate and postgraduate education, CPD and in-house training towards commonly encountered clinical presentations. The results may also have application in practice, for example when deciding on which designated clinics to run or equipment to invest in. Given the results, dental, obesity and behaviour clinics could provide an opportunity for practices to detect these common problems at an early stage and allow more time to educate owners in monitoring, managing and treating these problems. There was a particular disconnect between clinical signs and clinical examination findings in rabbits, so designated rabbit clinics would also be worthwhile and provide an opportunity to educate owners on health and husbandry in this species. Veterinary surgeons could also use the results to tailor history taking and clinical examination based upon the common clinical signs and examination findings in each species.
There are several limitations to the method used, some of which have been discussed in more depth in a previous paper (Robinson and others 2014). These include the use of a convenience sample of practices and demand characteristics, where a participant's knowledge of the purpose of a study unconsciously changes their behaviour (McCambridge and others 2012). However there are additional limitations which are specific to this study, including the validity of the categorisation of data, for example by body system. This could potentially be problematic as only one researcher collected and coded all data during the main study. While discussions with colleagues around categorisation of data and recording of such discussions helped ensure consistency of coding, there may be disagreement as to how some problems should be coded. For example, problems affecting the anal glands were consistently coded as gastrointestinal problems during this study, but it could be argued that these could be coded as skin problems. Clinical signs or examination abnormalities which are easily identifiable by owner or veterinary surgeon could also potentially be over-represented. Additionally, only the problems discussed verbally with the owner were recorded, and it may be that additional problems were identified on clinical examination but were not discussed during the consultation. Similarly, it could be that owners did not raise all problems which they were concerned about. A previous study (Roshier and McBride 2013) reported that owners of dogs with behavioural problems frequently did not mention these during the veterinary consultation, and this may apply equally to other types of specific health problem. Individual veterinary surgeon-owner communication is likely to heavily impact whether additional problems are raised by the owner and previous work by Dysart and others (2011) found that the use of open-ended questions significantly increased the number of problems raised by the client.
In conclusion, the results provide a detailed overview of the caseload that may be difficult to achieve using other methods. The findings further highlight the complexity of the consultation and emphasise the need to consider all problems discussed in order to gain an accurate view of the caseload. It is unclear whether other methods, such as use of clinical records, provide enough information about the complexity of a consultation and include all problems discussed during the consultation for each patient. Therefore data gathered using a direct observation may be a useful method to assess the reliability of other methods of data collection.
Supplementary Material
Acknowledgments
The authors thank the sentinel practices, their clients and patients for their involvement in the study. This study was supported by an unrestricted grant from Novartis Animal Health and The University of Nottingham.
Footnotes
Correction notice: This article has been corrected since it was published Online First. The graphs in Figures 2 and 3 were the wrong way round and have now been corrected.
The remaining 690 patients presented for preventive medicine, however specific health problems discussed in these patients would still be included as non-presenting problems.
References
- DAVIES M. (2011) Internet users’ perception of the importance of signs commonly seen in old animals with age-related diseases. Veterinary Record 169, 584 10.1136/vr.d5512 [DOI] [PubMed] [Google Scholar]
- DEAN R. S. PFEIFFER D. U. & ADAMS V. J. (2013) The incidence of feline injection site sarcomas in the United Kingdom. BMC Vet Res 9:17 10.1186/1746-6148-9-17 [DOI] [PMC free article] [PubMed] [Google Scholar]
- DYSART L.M.A. COE J.B. & ADAMS C.L. (2011) Analysis of solicitation of clients concerns in companion animal practice. Journal of the American Veterinary Medical Association 238, 1609–15 10.2460/javma.238.12.1609 [DOI] [PubMed] [Google Scholar]
- EBELL M. H. BUDSBERG S. CERVERO R. SHINHOLSER J. & CALL M. (2013) What are the clinical questions of practicing veterinarians? Journal of Veterinary Medical Education 40, 310–316 10.3138/jvme.0113-028R1 [DOI] [PubMed] [Google Scholar]
- EVANS J. M. LANE D. R. & HENDY P. G. (1974) Profile of Small Animal Practice. Journal of Small Animal Practice 15, 595–607 10.1111/j.1748-5827.1974.tb06504.x [DOI] [PubMed] [Google Scholar]
- HILL P. B. LO A. EDEN C. A. N. HUNTLEY S. MOREY V. RAMSEY S. RICHARDSON C. SMITH D. J. SUTTON C. TAYLOR M. D. THORPE E. TIDMARSH R. & WILLIAMS V. (2006) Survey of the prevalence, diagnosis and treatment of dermatological conditions in small animals in general practice. Veterinary Record 158, 533–539 10.1136/vr.158.16.533 [DOI] [PubMed] [Google Scholar]
- JLA (2014) The James Lind Alliance: Tackling treatment uncertainties together. JLA; www.lindalliance.org/. Accessed January 23, 2014 [DOI] [PubMed] [Google Scholar]
- LUND E. M. ARMSTRONG P. J. KIRK C. A. KOLAR L. M. & KLAUSNER J. S. (1999) Health status and population characteristics of dogs and cats examined at private veterinary practices in the United States. Journal of the American Veterinary Medical Association 214, 1336–1341 [PubMed] [Google Scholar]
- MCCAMBRIDGE J. DE BRUIN M. & WITTON J. (2012) The effects of demand characteristics on research participant behaviours in non-laboratory settings: a systematic review. PLoS ONE 7, e39116 10.1371/journal.pone.0039116 [DOI] [PMC free article] [PubMed] [Google Scholar]
- O'NEILL D.G. CHURCH D.B. MCGREEVY P.D. THOMSON P.C. & BRODBELT D.C. (2014) Prevalence of disorders recorded in dogs attending primary-case veterinary practices in England. PLoS ONE 9, 1–16 [DOI] [PMC free article] [PubMed] [Google Scholar]
- ROBINSON N. J. (2014) Use of sentinel practices to obtain data regarding common clinical conditions and presentations in small animal consultations [PhD Thesis]. The University of Nottingham [Google Scholar]
- ROBINSON N. J. BRENNAN M. L. COBB M. & DEAN R. S. (2014) Capturing the complexity of first opinion small animal consultations using direct observation. Veterinary Record, Published Online First: 26 September 2014 doi:10.1136/vr.102548 10.1136/vr.102548 [DOI] [PMC free article] [PubMed] [Google Scholar]
- ROBOTHAM J. & GREEN L. E. (2004) Pilot study to investigate the feasibility of surveillance of small animals in the UK. Journal of Small Animal Practice 45, 213–218 [PubMed] [Google Scholar]
- ROSHIER A. L. & MCBRIDE E. A. (2013) Veterinarians’ perceptions of behaviour support in small animal practice. Veterinary Record 172, 267 10.1136/vr.101124 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.