

Abstract
Background
A better understanding of factors associated with adopting leisure-time physical activity among people with chronic vascular conditions can help policy-makers and health care professionals develop strategies to promote secondary prevention among older Canadians.
Data and methods
Cross-sectional data from the 1994/1995 National Population Health Survey (NPHS), household component, and the 2007/2008 Canadian Community Health Survey were used to estimate the prevalence of inactivity. Longitudinal data from eight cycles (1994/1995 through 2008/2009) of the NPHS, household component, were used to examine the adoption of leisure-time physical activity, intentions to change health risk behaviours, and barriers to change.
Results
Over half (54%) of the population aged 40 or older were inactive during their leisure time in 2007/2008. A new vascular diagnosis was not associated with initiating leisure-time physical activity. Among the newly diagnosed, those with no disability or a mild disability had higher odds of undertaking leisure-time physical activity.
Interpretation
The majority of Canadians in mid- to late life are inactive. They tend to remain so when diagnosed with a vascular condition.
Keywords: aged, chronic disease, elderly, exercise, health promotion, lifestyle, middle age, public health, social environmnent
Inactive lifestyles have been recognized as a threat to good health and a contributor to higher health care costs and premature death.1–4 A lack of regular physical activity is associated with the development of chronic conditions including heart disease, hypertension and diabetes.5,6 Physical activity may help prevent these conditions—directly, through improved vascular health,6,7 or indirectly, through mechanisms such as weight control, stress reduction and quality of sleep.8 The benefits extend to secondary prevention, whereby active lifestyles help those who have already developed chronic conditions limit the progress or complications of the disease.8
Despite the highly promoted benefits of physical activity, most Canadians are relatively inactive. Fewer than 15% of adults aged 40 or older meet Canada’s new physical activity guidelines.9 An estimated 40% of Canadians aged 40 to 59 average more than the recommended 10,000 steps per day; at ages 60 to 79, the figure is 20%.9
While never a positive experience, developing a chronic vascular disease may ultimately yield health benefits if it is a “wake-up call,” prompting inactive individuals to become more physically active. In fact, changes in health behaviour after the onset of chronic conditions are well documented. For example, smoking cessation is more common among people newly diagnosed with conditions such as heart disease, stroke, cancer, diabetes and hypertension than among people without a new diagnosis.10–14 Intentional weight loss, dietary changes, lowering low density lipoprotein (LDL) cholesterol, and reduced alcohol consumption following adverse health events have also been reported.10,11,15,16
Findings about changes in physical activity after the diagnosis of a chronic condition are less clear. Newsom et al.16 reported no significant increase in the percentage of people who became active after being diagnosed; on the contrary, following a diagnosis of cancer, stroke or lung disease, people were less likely to report regular vigorous exercise. Neutal12 found a small decrease in inactive behaviour after a hypertension diagnosis, whereas van Gool et al.17 reported increases in the likelihood of inactive behaviour after diagnosis of chronic conditions. Allegrante et al.11 found significant positive changes in overall physical activity and strength training among people with coronary artery disease.
This study uses a large, population-based, longitudinal sample of adults to examine: 1) whether inactive Canadians aged 40 or older who are free of vascular disease become active after a new vascular diagnosis; 2) factors associated with becoming active during leisure time; and 3) changes or intentions to change health behaviours, including physical activity, among the newly diagnosed.
Methods
Data source
The “inactive” percentage of the population was estimated from the 1994/1995 cross-sectional file of the National Population Health Survey (NPHS) and from the Canadian Community Health Survey (CCHS) - Annual component 2007/2008. Data on changes in physical activity are from eight cycles (1994/1995 through 2008/2009) of the longitudinal household file of the NPHS. Descriptions of the NPHS and CCHS methodologies are available in published reports.18–20 Further details about the NPHS and CCHS are available from the respective survey documentation at: www.statcan.gc.ca.
Definitions
To measure leisure-time physical activity, respondents were asked to report the frequency and duration of their participation in a variety of activities over the past three months (Appendix Table A).21,22 Average daily energy expenditure (EE) for all activities was calculated as:
where:
Ni = number of times respondent engaged in activityi over a 12-month period;
Di = average duration in hours of activityi;
MET = energy cost of activity expressed as kilocalories expended per kilogram of body weight per hour of activity (kcal/kg/hour).
MET values are typically expressed in three intensity levels (low, medium, high). Because NPHS respondents were not asked to specify the intensity of their activities, MET values corresponding to the low intensity value of each activity were used, an approach adopted from the Canadian Fitness and Lifestyle Research Institute. Respondents were classified as either inactive (EE<1.5) or active (EE≥1.5). Those who were inactive at baseline and active two years later were classified as became active.
Respondents reported if a health professional had diagnosed them with chronic conditions that had lasted or were expected to last six months or more. Those with high blood pressure, heart disease, and/or diabetes were classified as having a vascular disease. Those who took insulin in the past month were considered to have diabetes. Once a vascular condition was reported, respondents were considered to have the condition in every subsequent cycle.
Level of disability accounted for the presence and severity of chronic conditions that interfere with physical activity but were not included in the models (for example, arthritis). Level of disability was based on the Health Utility Index (HUI3) developed at McMaster University.23–25 Functional health, based on vision, hearing, speech, mobility, dexterity, cognition, emotion, pain and discomfort, was scored and categorized into levels of disability: none (1.00), mild (0.89 to 0.99), moderate (0.70 to 0.88) or severe (less than 0.70), and then dichotomized to no/mild disability versus moderate/severe disability.
Earlier work,26,27 confirmed using the 1994/1995 NPHS longitudinal sample, identified two distinct factors within the mastery scale: fatalism and control. The first five statements from the mastery module loaded onto fatalism (Eigenvalue 2.9; Cronbach’s alpha 0.8):
-
1
You have little control over the things that happen to you.
-
2
There is really no way you can solve some of the problems you have.
-
3
There is little you can do to change many of the important things in your life.
-
4
You often feel helpless in dealing with problems of life.
-
5
Sometimes you feel that you are being pushed around in life.
Responses were scaled from 0 (strongly agree) to 4 (strongly disagree) and summed for a potential range of 0 to 20. Individuals with a total below the median (less than 14) were considered to be more fatalistic.
The final two statements loaded onto control (Eigenvalue 1.1; Cronbach’s alpha 0.5):
-
6
What happens to you in the future mostly depends on you.
-
7
You can do just about anything you really set your mind to.
Responses were scaled from 0 (strongly disagree) to 4 (strongly agree) and summed for a potential range of 0 to 8. Individuals who scored below the median (less than 6) were classified as having a low sense of control. Cycles 2 and 3 of the NPHS excluded the mastery module; analyses that included fatalism and control were based on the remaining cycles.
Perceived social support was based on four yes/no questions in the first two NPHS cycles (Appendix Table B). Respondents who answered “yes” to all four questions had high social support. For the remaining cycles, perceived social support was measured using the Emotional or Informational Support - MOS Subscale.28 The eight questions were answered on a five-point scale: none of the time (score 1), a little of the time (2), some of the time (3), most of the time (4), or all of the time (5). People who responded “some,” “most,” or “all of the time” to all eight questions were classified as having high social support.
Analytical techniques
The analysis was completed using SAS software Version 9.1 (Copyright, 2002–2003 SAS Institute Inc.). Data were weighted using age, sex, province, and non-response adjustments to ensure consistency with census-based estimates for the reference year of the survey. To account for survey design effects of the NPHS and CCHS, p-values were estimated, and significance tests were performed using the bootstrap technique.29,30
Cross-sectional analyses
Based on cycle 1 (1994/1995) of the NPHS household component and the 2007/2008 CCHS, weighted frequencies and cross-tabulations were calculated to estimate the percentage of the household population aged 40 or older who were inactive, by sex and age group.
Longitudinal analyses
Weighted frequencies were used to estimate the percentage of the household population aged 40 or older who were inactive or active at the first NPHS cycle. In the seven subsequent cycles (1996/1997 through 2008/2009), estimates were calculated of the percentage of the remaining cohort who, from one cycle to the next, remained inactive or active, or who became inactive or active.
The multivariate logistic regression was based on data from eight cycles of the NPHS. The data were pooled to create seven cohorts of observations with baseline years starting at 1994/1995 and follow-up two years later (Appendix Table C). The study sample was limited to respondents who, at each baseline year, were aged 40 or older, inactive and free of vascular disease, and who provided a full response at baseline and follow-up. Respondents continued to contribute records to the analyses for every cycle in which they met the baseline criteria.
The second cycle of the NPHS included questions about improvements in health behaviour, and barriers and intentions to improve health behaviour. The analysis of associations between a new vascular diagnosis and these variables was based on the first cohort of observations (1994/1995 to 1996/1997).
All analyses were stratified by gender.
Results
In 2007/2008, 54% of people aged 40 or older were inactive during their leisure time, down from 63% in 1994/1995. This change over time was evident across all age groups (Figure 1).
Figure 1. Percentage inactive during leisure time, by age group and sex, household population aged 40 or older, Canada excluding territories, 1994/1995 and 2007/2008.
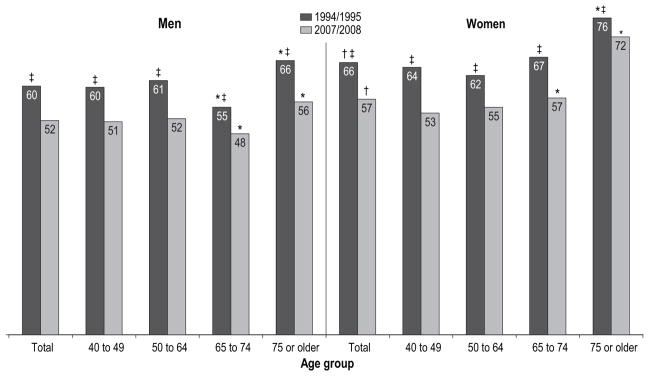
* significantly different from previous age group in same year (p<0.05)
†significantly different from men in same year (p<0.05)
‡significantly different from 2007/2008 (p<0.05)
Source: 1994/1995 National Population Health Survey, cross-sectional sample; 2007/2008 Canadian Community Health Survey.
Seniors aged 75 or older were more likely than younger adults to be inactive. However, men aged 65 to 74 were less likely than those aged 50 to 64 to be inactive. Overall, women were more likely than men to be inactive.
Between consecutive cycles of the NPHS, close to 30% of the cohort changed their leisure-time physical activity level, with approximately equal numbers becoming active if they were inactive, or becoming inactive if they were active (Figure 2). For men, a new diagnosis of a vascular condition was not associated with level of physical activity at follow-up (Table 1). On the other hand, newly diagnosed women had lower odds (0.8) of being active at follow-up, although this association lost significance when other factors were taken into account (Table 2). In the adjusted models, younger age and having no or mild disabilities were associated with higher odds of becoming active for women. Higher education was associated with becoming active for both sexes.
Figure 2. Percentage who maintained or changed leisure-time activity level over two-year period, household population aged 40 or older at baseline, Canada excluding territories, 1994/1995 to 2008/2009.

Source: 1994/1995 to 2008/2009 National Population Health Survey, longitudinal sample (square).
Table 1.
Odds ratios relating selected characteristics to becoming active, inactive male household population aged 40 or older free of vascular disease at baseline, Canada excluding territories, 1994/95 to 2008/2009
| Characteristics | Unadjusted odds ratio |
95% confidence interval |
Model 1
|
Model 2
|
Model 3
|
Model 4
|
|||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Adjusted odds ratio |
95% confidence interval |
Adjusted odds ratio |
95% confidence interval |
Adjusted odds ratio |
95% confidence interval |
Adjusted odds ratio |
95% confidence interval |
||||||||
| from | to | from | to | from | to | from | to | from | to | ||||||
| New vascular diagnosis | |||||||||||||||
| Yes | 0.9 | 0.7 | 1.1 | 0.9 | 0.7 | 1.1 | 0.9 | 0.7 | 1.1 | 0.9 | 0.7 | 1.1 | 0.9 | 0.7 | 1.2 |
| No† | 1.0 | … | … | 1.0 | … | … | 1.0 | … | … | 1.0 | … | … | 1.0 | … | … |
| Disability | |||||||||||||||
| No or mild | 1.2 | 1.0 | 1.4 | 1.1 | 1.0 | 1.4 | 1.1 | 1.0 | 1.4 | 1.1 | 0.9 | 1.4 | 1.1 | 0.9 | 1.3 |
| Moderate or severe† | 1.0 | … | … | 1.0 | … | … | 1.0 | … | … | 1.0 | … | … | 1.0 | … | … |
| At baseline | |||||||||||||||
| Socio-demographic | |||||||||||||||
| Age group | |||||||||||||||
| 40 to 49 | 1.3 | 1.0 | 1.9 | 1.1 | 0.8 | 1.6 | 1.2 | 0.9 | 1.7 | 1.2 | 0.8 | 1.8 | 1.2 | 0.9 | 1.8 |
| 50 to 64 | 1.3 | 0.9 | 1.9 | 1.2 | 0.8 | 1.7 | 1.3 | 0.9 | 1.8 | 1.3 | 0.9 | 2.0 | 1.2 | 0.9 | 1.8 |
| 65 to 74 | 1.4 | 1.0 | 2.0 | 1.4 | 1.0 | 1.9 | 1.4 | 1.0 | 2.0 | 1.5 | 1.0 | 2.4 | 1.4 | 1.0 | 2.0 |
| 75 or older† | 1.0 | … | … | 1.0 | … | … | 1.0 | … | … | 1.0 | … | … | 1.0 | … | … |
| Education | |||||||||||||||
| Postsecondary graduation | 1.3* | 1.1 | 1.6 | 1.3* | 1.1 | 1.6 | 1.3* | 1.1 | 1.6 | 1.3* | 1.0 | 1.6 | 1.3* | 1.1 | 1.5 |
| Less than postsecondary graduation† | 1.0 | … | … | 1.0 | … | … | 1.0 | … | … | 1.0 | … | … | 1.0 | … | … |
| Health behaviour | |||||||||||||||
| Smoking | |||||||||||||||
| Never | 1.3* | 1.0 | 1.6 | … | … | … | 1.2 | 1.0 | 1.6 | … | … | … | … | … | … |
| Former | 1.4* | 1.2 | 1.7 | … | … | … | 1.4* | 1.2 | 1.7 | … | … | … | … | … | … |
| Current smoker† | 1.0 | … | … | … | … | … | 1.0 | … | … | … | … | … | … | … | … |
| Personal characteristics | |||||||||||||||
| Fatalism‡ | |||||||||||||||
| High | 0.8* | 0.7 | 0.9 | … | … | … | … | … | … | 0.9 | 0.7 | 1.0 | … | … | … |
| Low† | 1.0 | … | … | … | … | … | … | … | … | 1.0 | … | … | … | … | … |
| Control‡ | |||||||||||||||
| Low | 0.8* | 0.6 | 1.0 | … | … | … | … | … | … | 0.8 | 0.6 | 1.0 | … | … | … |
| High† | 1.0 | … | … | … | … | … | … | … | … | 1.0 | … | … | … | … | … |
| Social resources | |||||||||||||||
| Has regular medical doctor | |||||||||||||||
| Yes | 1.3* | 1.0 | 1.6 | … | … | … | … | … | … | … | … | … | 1.2* | 1.0 | 1.5 |
| No† | 1.0 | … | … | … | … | … | … | … | … | … | … | … | 1.0 | … | … |
| High social support | |||||||||||||||
| Yes | 1.3* | 1.1 | 1.6 | … | … | … | … | … | … | … | … | … | 1.2 | 1.0 | 1.5 |
| No† | 1.0 | … | … | … | … | … | … | … | … | … | … | … | 1.0 | … | … |
| Married/Common-law/Living with partner | |||||||||||||||
| Yes | 1.2 | 1.0 | 1.4 | … | … | … | … | … | … | … | … | … | 1.1 | 0.9 | 1.3 |
| No† | 1.0 | … | … | … | … | … | … | … | … | … | … | … | 1.0 | … | … |
reference category
based on cycles 1 and 4 through 8
significantly different from reference category (p<0.05)
… not applicable
Note: Because of rounding, some odds ratios with lower or upper confidence limit of 1.0 were statistically significant.
Source: 1994/1995 to 2008/2009 National Population Health Survey, longitudinal sample (square).
Table 2.
Odds ratios relating selected characteristics to becoming active, inactive female household population aged 40 or older free of vascular disease at baseline, Canada excluding territories, 1994/95 to 2008/2009
| Characteristics | Unadjusted odds ratio |
95% confidence interval |
Model 1
|
Model 2
|
Model 3
|
Model 4
|
|||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Adjusted odds ratio |
95% confidence interval |
Adjusted odds ratio |
95% confidence interval |
Adjusted odds ratio |
95% confidence interval |
Adjusted odds ratio |
95% confidence interval |
||||||||
| from | to | from | to | from | to | from | to | from | to | ||||||
| New vascular diagnosis | |||||||||||||||
| Yes | 0.8* | 0.6 | 1.0 | 0.9 | 0.7 | 1.1 | 0.9 | 0.7 | 1.1 | 0.8 | 0.6 | 1.0 | 0.9 | 0.7 | 1.1 |
| No† | 1.0 | … | … | 1.0 | … | … | 1.0 | … | … | 1.0 | … | … | 1.0 | … | … |
| Disability | |||||||||||||||
| No or mild | 1.8* | 1.6 | 2.1 | 1.7* | 1.5 | 2.0 | 1.7* | 1.4 | 2.0 | 1.7* | 1.4 | 2.0 | 1.6* | 1.4 | 1.9 |
| Moderate or severe† | 1.0 | … | … | 1.0 | … | … | 1.0 | … | … | 1.0 | … | … | 1.0 | … | … |
| At baseline | |||||||||||||||
| Socio-demographic | |||||||||||||||
| Age group | |||||||||||||||
| 40 to 49 | 2.5* | 1.9 | 3.4 | 1.9* | 1.4 | 2.6 | 1.9* | 1.4 | 2.6 | 2.1* | 1.4 | 3.1 | 1.8* | 1.3 | 2.4 |
| 50 to 64 | 2.8* | 2.1 | 3.8 | 2.3* | 1.7 | 3.1 | 2.3* | 1.7 | 3.1 | 2.4* | 1.6 | 3.5 | 2.2* | 1.6 | 3.0 |
| 65 to 74 | 2.4* | 1.8 | 3.3 | 2.1* | 1.5 | 2.9 | 2.1* | 1.5 | 2.8 | 2.3* | 1.5 | 3.5 | 2.0* | 1.5 | 2.8 |
| 75 or older† | 1.0 | … | … | 1.0 | … | … | 1.0 | … | … | 1.0 | … | … | 1.0 | … | … |
| Education | |||||||||||||||
| Postsecondary graduation | 1.4* | 1.2 | 1.6 | 1.3* | 1.1 | 1.5 | 1.3* | 1.1 | 1.5 | 1.2* | 1.0 | 1.4 | 1.3* | 1.1 | 1.5 |
| Less than postsecondary graduation† | 1.0 | … | … | 1.0 | … | … | 1.0 | … | … | 1.0 | … | … | 1.0 | … | … |
| Health behaviour | |||||||||||||||
| Smoking | |||||||||||||||
| Never | 1.0 | 0.9 | 1.2 | … | … | … | 1.0 | 0.9 | 1.2 | … | … | … | … | … | … |
| Former | 1.4* | 1.2 | 1.7 | … | … | … | 1.4* | 1.1 | 1.6 | … | … | … | … | … | … |
| Current smoker† | 1.0 | … | … | … | … | … | 1.0 | … | … | … | … | … | … | … | … |
| Personal characteristics | |||||||||||||||
| Fatalism‡ | |||||||||||||||
| High | 0.8* | 0.7 | 1.0 | … | … | … | … | … | … | 0.9 | 0.8 | 1.1 | … | … | … |
| Low† | 1.0 | … | … | … | … | … | … | … | … | 1.0 | … | … | … | … | … |
| Control‡ | |||||||||||||||
| Low | 0.8* | 0.6 | 0.9 | … | … | … | … | … | … | 0.9 | 0.7 | 1.1 | … | … | … |
| High† | 1.0 | … | … | … | … | … | … | … | … | 1.0 | … | … | … | … | … |
| Social resources | |||||||||||||||
| Has regular medical doctor | |||||||||||||||
| Yes | 1.2 | 0.9 | 1.5 | … | … | … | … | … | … | … | … | … | 1.2 | 0.9 | 1.5 |
| No† | 1.0 | … | … | … | … | … | … | … | … | … | … | … | 1.0 | … | … |
| High social support | |||||||||||||||
| Yes | 1.4* | 1.1 | 1.6 | … | … | … | … | … | … | … | … | … | 1.2 | 1.0 | 1.4 |
| No† | 1.0 | … | … | … | … | … | … | … | … | … | … | … | 1.0 | … | … |
| Married/Common-law/Living with partner | |||||||||||||||
| Yes | 1.4* | 1.2 | 1.7 | … | … | … | … | … | … | … | … | … | 1.3* | 1.1 | 1.5 |
| No† | 1.0 | … | … | … | … | … | … | … | … | … | … | … | 1.0 | … | … |
reference category
based on cycles 1 and 4 through 8
significantly different from reference category (p<0.05)
… not applicable
Note: Because of rounding, some odds ratios with lower or upper confidence limit of 1.0 were statistically significant.
Source: 1994/1995 to 2008/2009 National Population Health Survey, longitudinal sample (square).
Former smokers of both sexes had higher odds of becoming active than did current smokers. In the adjusted models, this relationship persisted, but no difference was apparent between those who had never smoked and current smokers.
People who were more fatalistic and those with a lower sense of control had lower odds of becoming active, although these associations did not persist when potential confounders were taken into account.
The results demonstrated sex-specific associations between social resources and leisure-time physical activity. Men with a regular medical doctor and high social support had higher odds of becoming active, although the significance of the latter was attenuated in the adjusted model. For women, having a partner and high social support were significant, but again, social support lost significance when other confounders were considered.
Although a vascular diagnosis was generally not associated with becoming active, some people who were newly diagnosed did undertake leisure-time physical activity. The analysis was repeated, based only on respondents with a new vascular diagnosis (Tables 3 and 4). Even when other confounders were taken into account, people with no disability or a mild disability had significantly higher odds of becoming active than did those with a moderate or severe disability. The odds of becoming active were lower for men who were fatalistic and higher for women with a partner, although both associations lost significance in the full models.
Table 3.
Odds ratios relating selected characteristics to becoming active, inactive male household population aged 40 or older with new vascular disease diagnosis, Canada excluding territories, 1994/95 to 2008/2009
| Characteristics | Unadjusted odds ratio |
95% confidence interval |
Model 1
|
Model 2
|
Model 3
|
Model 4
|
|||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Adjusted odds ratio |
95% confidence interval |
Adjusted odds ratio |
95% confidence interval |
Adjusted odds ratio |
95% confidence interval |
Adjusted odds ratio |
95% confidence interval |
||||||||
| from | to | from | to | from | to | from | to | from | to | ||||||
| New vascular diagnosis | |||||||||||||||
| Yes | … | … | … | … | … | … | … | … | … | … | … | … | … | … | … |
| No† | … | … | … | … | … | … | … | … | … | … | … | … | … | … | … |
| Disability | |||||||||||||||
| No or mild | 1.9* | 1.2 | 2.9 | 1.9* | 1.2 | 2.9 | 1.9* | 1.2 | 2.9 | 2.0* | 1.1 | 3.6 | 1.7* | 1.1 | 2.6 |
| Moderate or severe† | 1.0 | … | … | 1.0 | … | … | 1.0 | … | … | 1.0 | … | … | 1.0 | … | … |
| At baseline | |||||||||||||||
| Socio-demographic | |||||||||||||||
| Age group | |||||||||||||||
| 40 to 49 | 2.7* | 1.1 | 7.1 | 2.2 | 0.8 | 5.8 | 2.3 | 0.9 | 6.1 | 2.8 | 0.7 | 12.0 | 2.0 | 0.7 | 5.4 |
| 50 to 64 | 2.5 | 1.0 | 6.6 | 2.2 | 0.8 | 5.8 | 2.2 | 0.8 | 6.1 | 3.3 | 0.8 | 13.9 | 2.1 | 0.7 | 5.7 |
| 65 to 74 | 2.7 | 1.0 | 7.7 | 2.6 | 0.9 | 7.6 | 2.6 | 0.9 | 7.7 | 6.1* | 1.3 | 27.3 | 2.6 | 0.9 | 7.6 |
| 75 or older† | 1.0 | … | … | 1.0 | … | … | 1.0 | … | … | 1.0 | … | … | 1.0 | … | … |
| Education | |||||||||||||||
| Postsecondary graduation | 1.2 | 0.7 | 2.0 | 1.1 | 0.6 | 1.8 | 1.1 | 0.6 | 1.8 | 1.1 | 0.6 | 1.9 | 1.1 | 0.6 | 1.8 |
| Less than postsecondary graduation† | 1.0 | … | … | 1.0 | … | … | 1.0 | … | … | 1.0 | … | … | 1.0 | … | … |
| Health behaviour | |||||||||||||||
| Smoking | |||||||||||||||
| Never | 1.2 | 0.7 | 2.3 | … | … | … | 1.2 | 0.6 | 2.3 | … | … | … | … | … | … |
| Former | 1.1 | 0.7 | 1.9 | … | … | … | 1.2 | 0.7 | 2.0 | … | … | … | … | … | … |
| Current smoker† | 1.0 | … | … | … | … | … | 1.0 | … | … | … | … | … | … | … | … |
| Personal characteristics | |||||||||||||||
| Fatalism‡ | |||||||||||||||
| High | 0.5* | 0.3 | 1.0 | … | … | … | … | … | … | 0.6 | 0.3 | 1.1 | … | … | … |
| Low† | 1.0 | … | … | … | … | … | … | … | … | 1.0 | … | … | … | … | … |
| Control‡ | |||||||||||||||
| Low | 1.0 | 0.6 | 1.9 | … | … | … | … | … | … | 1.5 | 0.7 | 3.0 | … | … | … |
| High† | 1.0 | … | … | … | … | … | … | … | … | 1.0 | … | … | … | … | … |
| Social resources | |||||||||||||||
| Has regular medical doctor | |||||||||||||||
| Yes | 0.8 | 0.4 | 1.8 | … | … | … | … | … | … | … | … | … | 0.8 | 0.4 | 1.8 |
| No† | 1.0 | … | … | … | … | … | … | … | … | … | … | … | 1.0 | … | … |
| High social support | |||||||||||||||
| Yes | 1.2 | 0.7 | 2.2 | … | … | … | … | … | … | … | … | … | 1.0 | 0.6 | 1.9 |
| No† | 1.0 | … | … | … | … | … | … | … | … | … | … | … | 1.0 | … | … |
| Married/Common-law/Living with partner | |||||||||||||||
| Yes | 1.3 | 0.7 | 2.2 | … | … | … | … | … | … | … | … | … | 1.1 | 0.6 | 2.0 |
| No† | 1.0 | … | … | … | … | … | … | … | … | … | … | … | 1.0 | … | … |
reference category
based on cycles 1 and 4 through 8
significantly different from reference category (p<0.05)
… not applicable
Note: Because of rounding, some odds ratios with lower or upper confidence limit of 1.0 were statistically significant.
Source: 1994/1995 to 2008/2009 National Population Health Survey, longitudinal sample (square).
Table 4.
Odds ratios relating selected characteristics to becoming active, inactive female household population aged 40 or older with new vascular disease diagnosis, Canada excluding territories, 1994/95 to 2008/2009
| Characteristics | Unadjusted odds ratio |
95% confidence interval |
Model 1
|
Model 2
|
Model 3
|
Model 4
|
|||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Adjusted odds ratio |
95% confidence interval |
Adjusted odds ratio |
95% confidence interval |
Adjusted odds ratio |
95% confidence interval |
Adjusted odds ratio |
95% confidence interval |
||||||||
| from | to | from | to | from | to | from | to | from | to | ||||||
| New vascular diagnosis | |||||||||||||||
| Yes | … | … | … | … | … | … | … | … | … | … | … | … | … | … | … |
| No† | … | … | … | … | … | … | … | … | … | … | … | … | … | … | … |
| Disability | |||||||||||||||
| No or mild | 2.5* | 1.6 | 3.9 | 2.5* | 1.6 | 3.8 | 2.5* | 1.6 | 3.8 | 2.8* | 1.6 | 4.9 | 2.3* | 1.5 | 3.6 |
| Moderate or severe† | 1.0 | … | … | 1.0 | … | … | 1.0 | … | … | 1.0 | … | … | 1.0 | … | … |
| At baseline | |||||||||||||||
| Socio-demographic | |||||||||||||||
| Age group | |||||||||||||||
| 40 to 49 | 3.6* | 1.7 | 7.5 | 2.5* | 1.1 | 5.2 | 2.5* | 1.1 | 5.4 | 1.6 | 0.7 | 3.9 | 2.1 | 0.9 | 4.5 |
| 50 to 64 | 2.4* | 1.2 | 5.0 | 1.9 | 0.9 | 4.1 | 2.0 | 0.9 | 4.2 | 1.1 | 0.5 | 2.6 | 1.7 | 0.8 | 3.7 |
| 65 to 74 | 2.4* | 1.1 | 5.4 | 1.8 | 0.8 | 4.1 | 1.8 | 0.8 | 4.1 | 1.3 | 0.5 | 3.3 | 1.7 | 0.7 | 3.7 |
| 75 or older† | 1.0 | … | … | 1.0 | … | … | 1.0 | … | … | 1.0 | … | … | 1.0 | … | … |
| Education | |||||||||||||||
| Postsecondary graduation | 1.3 | 0.9 | 2.1 | 1.2 | 0.8 | 1.9 | 1.2 | 0.8 | 1.9 | 1.5 | 0.9 | 2.6 | 1.2 | 0.8 | 1.9 |
| Less than postsecondary graduation† | 1.0 | … | … | 1.0 | … | … | 1.0 | … | … | 1.0 | … | … | 1.0 | … | … |
| Health behaviour | |||||||||||||||
| Smoking | |||||||||||||||
| Never | 1.0 | 0.6 | 1.7 | … | … | … | 1.0 | 0.6 | 1.8 | … | … | … | … | … | … |
| Former | 1.1 | 0.7 | 1.9 | … | … | … | 1.2 | 0.7 | 2.0 | … | … | … | … | … | … |
| Current smoker† | 1.0 | … | … | … | … | … | 1.0 | … | … | … | … | … | … | … | … |
| Personal characteristics | |||||||||||||||
| Fatalism‡ | |||||||||||||||
| High | 1.0 | 0.6 | 1.6 | … | … | … | … | … | … | 1.2 | 0.7 | 2.1 | … | … | … |
| Low† | 1.0 | … | … | … | … | … | … | … | … | 1.0 | … | … | … | … | … |
| Control‡ | |||||||||||||||
| Low | 0.7 | 0.4 | 1.3 | … | … | … | … | … | … | 0.9 | 0.5 | 1.8 | … | … | … |
| High† | 1.0 | … | … | … | … | … | … | … | … | 1.0 | … | … | … | … | … |
| Social resources | |||||||||||||||
| Has regular medical doctor | |||||||||||||||
| Yes | 0.6 | 0.3 | 1.3 | … | … | … | … | … | … | … | … | … | 0.8 | 0.3 | 1.7 |
| No† | 1.0 | … | … | … | … | … | … | … | … | … | … | … | 1.0 | … | … |
| High social support | |||||||||||||||
| Yes | 1.3 | 0.7 | 2.2 | … | … | … | … | … | … | … | … | … | 1.2 | 0.7 | 2.2 |
| No† | 1.0 | … | … | … | … | … | … | … | … | … | … | … | 1.0 | … | … |
| Married/Common-law/Living with partner | |||||||||||||||
| Yes | 1.5* | 1.0 | 2.3 | … | … | … | … | … | … | … | … | … | 1.2 | 0.8 | 1.9 |
| No† | 1.0 | … | … | … | … | … | … | … | … | … | … | … | 1.0 | … | … |
reference category
based on cycles 1 and 4 through 8
significantly different from reference category (p<0.05)
… not applicable
Note: Because of rounding, some odds ratios with lower or upper confidence limit of 1.0 were statistically significant.
Source: 1994/1995 to 2008/2009 National Population Health Survey, longitudinal sample (square).
Further analyses examined associations between a vascular diagnosis and actual changes and intentions to change health behaviours. The odds of having made any improvements in health over the past 12 months were no different between those with and without a new vascular diagnosis (Table 5). Among women who had actually improved their health behaviour, those with a new vascular diagnosis had lower odds of reporting that the most important change was increased exercise. Barriers to making efforts to improve health included being too tired (men) and disability or a health problem (women).
Table 5.
Odds ratios relating new vascular diagnosis to improvements in health behaviour, and barriers to and intentions to improve health behaviour, by sex, inactive household population aged 40 or older in 1994/1995, Canada excluding territories, 1996/97
| Men
|
Women
|
|||||
|---|---|---|---|---|---|---|
| Unadjusted odds ratios | 95% confidence interval
|
Unadjusted odds ratios | 95% confidence interval
|
|||
| from | to | from | to | |||
| Improvements | ||||||
| Attempted to improve health in past 12 months | ||||||
| New vascular diagnosis | ||||||
| Yes | 1.4 | 1.0 | 2.0 | 1.1 | 0.8 | 1.6 |
| No† | 1.0 | … | … | 1.0 | … | … |
| Increased exercise | ||||||
| New vascular diagnosis | ||||||
| Yes | 1.0 | 0.6 | 1.6 | 0.6* | 0.4 | 1.0 |
| No† | 1.0 | … | … | 1.0 | … | … |
| Barriers | ||||||
| Too tired | ||||||
| New vascular diagnosis | ||||||
| Yes | 5.9* | 1.5 | 22.9 | 1.4 | 0.4 | 4.8 |
| No† | 1.0 | … | … | 1.0 | … | … |
| Disability/Health problem | ||||||
| New vascular diagnosis | ||||||
| Yes | 3.1 | 1.0 | 10.3 | 5.1* | 2.2 | 11.7 |
| No† | 1.0 | … | … | 1.0 | … | … |
| Intentions | ||||||
| Intend to improve physical health in next year | ||||||
| New vascular diagnosis | ||||||
| Yes | 1.0 | 0.5 | 1.7 | 0.6* | 0.4 | 0.9 |
| No† | 1.0 | … | … | 1.0 | … | … |
| Intend to start/increase exercise | ||||||
| New vascular diagnosis | ||||||
| Yes | 0.8 | 0.4 | 1.5 | 1.0 | 0.5 | 1.8 |
| No† | 1.0 | … | … | 1.0 | … | … |
reference category
significantly different from reference category (p<0.05)
… not applicable
Note: Because of rounding, odds ratios with upper confidence limit of 1.0 was statistically significant.
Source: 1994/1995 and 1996/1997 National Population Health Survey, longitudinal sample (square).
Looking to the future, women with a new vascular diagnosis had lower odds of reporting that they intended to try to improve their physical health in the next year. For those who planned to make changes, having a vascular diagnosis was not associated with the intention to start or increase exercise.
Discussion
This study of a large population-based sample found that inactive adults in mid- to late-life who had a new vascular diagnosis (hypertension, heart disease or diabetes) did not become more active.
It was hypothesized that individuals’ sense of mastery (fatalism and control) may influence their behaviour following a new vascular diagnosis. The expectation was that those with higher mastery would be more inclined to adopt leisure-time physical activity. Earlier work has shown that a higher sense of mastery is associated with positive self-perceived health among people already experiencing chronic conditions,31,32 and that older individuals with a higher sense of mastery declined significantly less over time than did those with a lower sense of mastery.33 One of several possible explanations is that people with a greater sense of mastery would be more likely to engage in health-promoting behaviours and use preventive health services.34,35 Results from this study only weakly support this suggestion, as associations between mastery and becoming active were found only in unadjusted models.
It is understandable that inactive people remain so following the setback of a new chronic condition. The NPHS revealed barriers to improving physical health among those with a new diagnosis: being too tired (men) and a disability or health problem (women). These are common barriers among the general population,36 so it is not unexpected that they inhibit physical activity among people coping with new chronic conditions. Some studies have suggested that older people may fear that physical activity will be painful or cause injury.37
Smoking may be a key to other changes in health behaviour. This study and others show that former smokers have higher odds of becoming active than do current smokers.35 However, Allegrante et al.11 suggest that physical activity is a “gateway” behaviour; once changes are made in this domain, others follow. In contrast, Newsom et al.38 found that important health behaviours, including exercise and smoking, are largely independent, and therefore, a change in one would not necessarily lead to a change in others.
Social resources may influence the pursuit of more active lifestyles. This study demonstrated that having a regular doctor (men) and living with a spouse or partner (women) were significantly associated with becoming active. These are potential sources of support, which is important in helping older people become more active.39
Social norms may also play a role.37 The majority of Canadians are inactive, especially at older ages.9 Unlike changes such as smoking cessation (in Canada, where non-smokers are the majority,40 smokers conform by quitting), becoming active is contrary to the norm. Furthermore, stereotypes of older people as frail and disinclined to make and benefit from lifestyle changes create other barriers to becoming more active.41,42
It may also be that changes in physical activity were not detected in the NPHS. Respondents might have become more active, but not enough to change categories from “inactive” to “active.” However, this is unlikely. Preliminary analyses of changes in estimated energy expenditure between baseline and follow-up suggest that it was not a classification issue; inactive people really tended to remain that way.
Yet even while remaining inactive, respondents may have made progress in the “process” of becoming active. The Transtheoretical Model of Behaviour Change (TTM) outlines five stages: pre-contemplation, contemplation, planning, action, and maintenance.43,44 Diagnosis of a vascular condition could prompt movement through the early stages. Nonetheless, when respondents were asked about intentions to improve their physical health, diagnosis of a vascular condition was not associated with intentions to change. In fact, women newly diagnosed with a vascular condition had lower odds of intending to change. This is consistent with an earlier study of older Canadians.45
Limitations
Attrition due to non-response is a limitation in longitudinal research. Refusal to participate in the NPHS and loss to follow-up constitute non-response. Of the 17,598 observations that met the baseline inclusion criteria (40 or older, inactive, no vascular disease, and full response), 1,349 (7.7%) were excluded because of non-response at follow-up (Appendix Table C). A further 397(2.3%) were excluded because of death, and 109 (0.6%), because of institutionalization. Older people and those with less than postsecondary graduation were more likely to be non-responders; there was no difference between men and women (data not shown). Attrition introduces a potential selection bias, because younger and more educated respondents may differ in terms of physical activity.
Although the study design involved pooling of repeated measures to maximize sample size, relatively few records showed respondents becoming active over the two-year period, especially those newly diagnosed with a vascular condition (Appendix Table C). The small sample sizes increase the possibility of type II errors, whereby power may be insufficient to detect real associations between some independent variables and changes in physical activity.
The NPHS collects self-reported data, which are limited by recall and social desirability biases. Hypertension, heart disease, diabetes, and the use of insulin are not verified by any other source. Other health conditions that may be related to physical activity were not included in the study. However, the multivariate models controlled for disability in order to account for other conditions and for the severity of the vascular conditions.
The physical activity variable is limited to leisure-time activities; physical activity at work, during rehabilitation, and in other non-leisure domains was excluded. Consequently, respondents’ overall level of physical activity may be underestimated; some studies suggest that non-leisure activities, such as walking or cycling for transportation, account for a substantial share of total activity.46 Even so, older people are more likely than youth to be inactive in all domains of their life.46
No gold standard is available for measuring physical activity; potential problems and biases exist with both direct and indirect methods.48 Earlier work reported a relatively low correlation between directly measured and self-reported physical activity, and the direction of the differences was inconsistent—sometimes self-reports were higher; other times, lower.47 Despite the potential problems, self-report is an accepted method for collecting physical activity data in large population surveys such as the NPHS.
The list of physical activities varied slightly by NPHS cycle (Appendix Table A), so some “changes” may result from the inclusion or exclusion of particular activities. As well, between cycles, some respondents may have increased their leisure-time activity and then relapsed. Such changes would not be detected except perhaps in the sub-analysis when they were asked if they had done anything to improve their health in the past 12 months.
A wide range of factors that may influence whether a person becomes physically active after the diagnosis of a chronic condition are not collected by the NPHS. These include the attitudes and behaviours of family and friends, family history of disease and lifestyle, the availability and accessibility of rehabilitation programs, and the physical environment such as safe places to walk and recreational facilities.
Conclusion
Evidence from this study indicates that for Canadians in mid- to late life, a new diagnosis of a vascular condition was not associated with becoming more physically active during their leisure time. However, some people who were newly diagnosed did become active—those with no disability or a mild disability had higher odds of undertaking leisure-time physical activity. Further investigation is required to assess the extent to which older adults recognize physical activity as a viable approach to secondary prevention, the barriers older people, especially those with chronic conditions and disabilities, face in adopting more active lifestyles, and the support required to help this population become more active.
What is already known on this subject?
Relatively few older Canadians attempt to improve their health through exercise or other initiatives, often citing a lack of willpower as a barrier.
Despite some tendency for people to adopt better health risk behaviours such as smoking cessation, weight loss, dietary changes and reduced alcohol consumption when they face a new chronic condition, most individuals do not make needed changes.
Previous research has examined changes in physical activity following diagnosis of a new chronic condition, but the evidence is inconsistent.
What does this study add?
Among Canadians aged 40 or older, 57% of women and 52% of men were inactive in their leisure time in 2007/2008.
A new vascular diagnosis was not associated with becoming active among people in mid- to late-life.
Having a regular doctor (men) and living with a spouse/partner (women) were associated with adopting leisure-time physical activity.
Among people newly diagnosed with a vascular condition, level of disability was the main factor that accounted for whether they engaged in more leisure-time physical activity.
Acknowledgments
This study was supported in part by a grant from the National Institutes of Health: National Institute on Aging R01 AG034211, Newsom (PI).
Appendix
Table A.
Leisure-time physical activities included in longitudinal component of National Population Health Survey, by year
| Activity | 1994/1995 (cycle 1) | 1996/1997 (cycle 2) | 1998/1999 (cycle 3) | 2000/2001 (cycle 4) | 2002/2003 (cycle 5) | 2004/2005 (cycle 6) | 2006/2007 (cycle 7) | 2008/2009 (cycle 8) |
|---|---|---|---|---|---|---|---|---|
| Walking for exercise | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Gardening or yard work | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Swimming | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Bicycling | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Popular or social dance | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Home exercises | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Ice hockey | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Ice skating | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| In-line skating/Rollerblading | No | No | Yes | Yes | Yes | Yes | Yes | Yes |
| Jogging/Running | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Golfing | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Exercise class/Aerobics | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Cross-country skiing | Yes | Yes | No | No | No | No | No | No |
| Downhill skiing/Snowboarding | Yes/No | Yes/No | Yes/No | Yes/No | Yes | Yes | Yes | Yes |
| Bowling | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Baseball/Softball | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Tennis | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Weight-training | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Fishing | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Volleyball | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Yoga/Tai-chi | Yes | No | No | No | No | No | No | No |
| Basketball | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Other | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
Source: 1994/1995 to 2008/2009 National Population Health Survey, longitudinal sample, household component.
Table B.
Social support questions in National Population Health Survey, by year and cycle
| Year/Cycle | Questions |
|---|---|
|
1994/1995 and 1996/1997 Cycles 1 and 2 |
Do you have someone…
|
|
1998/1999 to 2008/2009 Cycles 3 to 8 |
How often is support available to you if you need someone…
|
Health Statistics Division, Statistics Canada.
Sherbourne CD, Stewart AL. The MOS social support survey. Social Science and Medicine 1991; 32(6): 705–14.
Table C.
Sample sizes for longitudinal analysis: 40 or older, inactive, no vascular disease, and full response at baseline, household population
| Cohort | Baseline (time 1) | Follow-up (time 2) | Eligible at baseline | Exluded at follow-up
|
Study sample
|
Inactive at follow-up
|
Active at follow-up
|
Vascular diagnosis at follow-up
|
Inactive and vascular diagnosis at follow-up
|
Active and vascular diagnosis at follow-up
|
|||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Non-response | Dead | Institution | Total | Men | Women | Men | Women | Men | Women | Men | Women | Men | Women | Men | Women | ||||
| 1 | 1994/1995 | 1996/1997 | 3,341 | 204 | 95 | 25 | 3,017 | 1,290 | 1,727 | 938 | 1,336 | 320 | 378 | 135 | 194 | 99 | 148 | 30 | 45 |
| 2 | 1996/1997 | 1998/1999 | 3,097 | 191 | 79 | 22 | 2,805 | 1,229 | 1,576 | 838 | 1,156 | 361 | 409 | 98 | 148 | 64 | 115 | 29 | 33 |
| 3 | 1998/1999 | 2000/2001 | 2,682 | 198 | 52 | 18 | 2,414 | 1,065 | 1,349 | 746 | 998 | 261 | 321 | 79 | 142 | 51 | 97 | 21 | 41 |
| 4 | 2000/2001 | 2002/2003 | 2,576 | 229 | 51 | 17 | 2,279 | 994 | 1,285 | 655 | 873 | 312 | 390 | 95 | 109 | 63 | 86 | 28 | 21 |
| 5 | 2002/2003 | 2004/2005 | 2,137 | 202 | 50 | 12 | 1,873 | 827 | 1,046 | 589 | 767 | 226 | 267 | 84 | 87 | 59 | 62 | 25 | 23 |
| 6 | 2004/2005 | 2006/2007 | 2,075 | 137 | 38 | 10 | 1,890 | 816 | 1,074 | 492 | 662 | 277 | 361 | 69 | 70 | 44 | 44 | 19 | 22 |
| 7 | 2006/2007 | 2008/2009 | 1,690 | 188 | 32 | 5 | 1,465 | 623 | 842 | 424 | 555 | 183 | 269 | 43 | 57 | 36 | 40 | 6 | 14 |
| Total | 17,598 | 1,349 | 397 | 109 | 15,743 | 6,844 | 8,899 | 4,682 | 6,347 | 1,940 | 2,395 | 603 | 807 | 416 | 592 | 158 | 199 | ||
Note: Non-response is composed of refusal to participate in survey and loss to follow-up.
Source: 1994/1995 to 2008/2009 National Population Health Survey, longitudinal sample (square).
Contributor Information
Pamela L. Ramage-Morin, Email: Pamela.Ramage-Morin@statcan.gc.ca, Health Analysis Division at Statistics Canada, Ottawa, Ontario, K1A 0T6. 1-613-951-1760
Julie Bernier, Email: Julie.Bernier@statcan.gc.ca, Health Analysis Division at Statistics Canada, Ottawa, Ontario, K1A 0T6. 1-613-951-4556.
Jason T. Newsom, Portland State University
Nathalie Huguet, Portland State University.
Bentson H. McFarland, Oregon Health and Science University
Mark S. Kaplan, Portland State University
References
- 1.Lalonde M. A New Perspective of the Health of Canadians (Catalogue H31-1374) Ottawa: Minister of Supply and Services; 1981. [Google Scholar]
- 2.Romanow RJ. Building on Values: The Future of Health Care in Canada – Final Report. Saskatoon: Commission on the Future of Health Care in Canada; 2002. [Accessed May 4, 2010]. Available at: http://dsp-psd.pwgsc.gc.ca/Collection/CP32-85-2002E.pdf. [Google Scholar]
- 3.Craig CL, Russell SJ, Cameron C, et al. Twenty-year trends in physical activity among Canadian adults. Canadian Journal of Public Health. 2004;95(1):59–63. doi: 10.1007/BF03403636. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Sari N. A short walk a day shortens the hospital stay: physical activity and the demand for hospital services for older adults. Canadian Journal of Public Health. 2010;101(5):385–9. doi: 10.1007/BF03404858. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Baumen AE. Updating the evidence that physical activity is good for health: an epidemiological review 2000–2003. Journal of Science and Medicine in Sport. 2004;7(1 Suppl):6–19. doi: 10.1016/s1440-2440(04)80273-1. [DOI] [PubMed] [Google Scholar]
- 6.Thijssen DHJ, Maiorana AJ, O’Driscoll G, et al. Impact of inactivity and exercise on the vasculature in humans. European Journal of Applied Physiology. 2010;108:845–75. doi: 10.1007/s00421-009-1260-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Joyner MJ, Green DJ. Exercise protects the cardiovascular system: effects beyond the traditional risk factors. The Journal of Physiology. 2009;587(23):5551–8. doi: 10.1113/jphysiol.2009.179432. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Warburton DER, Nicol CW, Bredin SSD. Health benefits of physical activity: The evidence. Canadian Medical Association Journal. 2006;174(6):801–9. doi: 10.1503/cmaj.051351. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Colley RC, Garriguet D, Janssen I, et al. Physical activity of Canadian adults: Accelerometer results from the 2007 to 2009 Canadian Health Measures Survey. Health Reports. 2011;22(1):15–23. [PubMed] [Google Scholar]
- 10.Keenan PS. Smoking and weight changes after new health diagnosis in older adults. Archives of Internal Medicine. 2009;169(3):237–42. doi: 10.1001/archinternmed.2008.557. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Allegrante JP, Peterson JC, Boutin-Foster C, et al. Multiple health-risk behaviour in a chronic disease population: What behaviours do people choose to change? Preventive Medicine. 2008;46:247–51. doi: 10.1016/j.ypmed.2007.09.007. [DOI] [PubMed] [Google Scholar]
- 12.Neutel CI, Campbell NRC. Changes in lifestyle after hypertension diagnosis in Canada. Canadian Journal of Cardiology. 2008;24(3):199–204. doi: 10.1016/s0828-282x(08)70584-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Falba T. Health events and the smoking cessation of middle aged Americans. Journal of Behavioral Medicine. 2005;28(1):21–33. doi: 10.1007/s10865-005-2560-1. [DOI] [PubMed] [Google Scholar]
- 14.Shields M. The journey to quitting smoking. Health Reports. 2005;16(3):19–36. [PubMed] [Google Scholar]
- 15.Vandelanotte C, Reeves MM, Brug J, De Bourdeaudhuij I. A randomized trial of sequential and simultaneous multiple behavior change interventions for physical activity and fat intake. Preventive Medicine. 2008;46:232–7. doi: 10.1016/j.ypmed.2007.07.008. [DOI] [PubMed] [Google Scholar]
- 16.Newsom JT, Huguet N, McCarthy MJ, et al. Health behavior change following chronic illness in middle and late life. Journals of Gerontology: Psychological Sciences. 2011 doi: 10.1093/geronb/gbr103. in press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.van Gool CH, Kempen GIJM, Penninx BWJH, et al. Chronic disease and lifestyle transitions: Results from the Longitudinal Aging Study Amsterdam. Journal of Aging and Health. 2007;19(3):416–38. doi: 10.1177/0898264307300189. [DOI] [PubMed] [Google Scholar]
- 18.Swain L, Catlin G, Beaudet MP. The National Population Health Survey–its longitudinal nature. Health Reports. 1999;10(4):62–82. [PubMed] [Google Scholar]
- 19.Tambay J-L, Catlin G. Sample design of the National Population Health Survey. Health Reports. 1995;7(1):29–38. [PubMed] [Google Scholar]
- 20.Béland Y, Bélanger Y, Dufour J, et al. Comparaison méthodologique entre l’Enquête sur la santé dans les collectivités canadiennes (ESCC) et l’Enquête de surveillance de l’usage du tabac au Canada (ESUTC): Rapport interne du groupe de travail. Ottawa: Statistics Canada; 2002. [Google Scholar]
- 21.Ontario Ministry of Health. Ontario Health Survey 1990: Users’s Guide Volume 2, Microdata Manual. Toronto: Ontario Ministry of Health; 1992. [Google Scholar]
- 22.Statistics Canada. National Population Health Survey, Household Component: Documentation for the Derived Variables and the Constant Longitudinal Variables (Specifications), Cycles 1 to 8 (1994/1995 to 2008/2009) Ottawa: Statistics Canada; 2010. [Google Scholar]
- 23.Furlong W, Feeny D. Health Utilities Index Mark 2 (HUI2) and Mark 3 (HUI3) Disability Categories for Single- and Multi-Attribute Utility Scores. Oct 29, 2002. Unpublished. [Google Scholar]
- 24.Feeny D, Furlong W, Torrance GW, et al. Multiattribute and single-attribute utility functions for the Health Utilities Index Mark 3 System. Medical Care. 2002;40(2):113–28. doi: 10.1097/00005650-200202000-00006. [DOI] [PubMed] [Google Scholar]
- 25.Feng Y, Bernier J, McIntosh C, Orpana H. Validation of disability categories derived from Health Utilities Index Mark 3 scores. Health Reports. 2009;20(2):43–50. [PubMed] [Google Scholar]
- 26.Pearlin LI, Schooler C. The structure of coping. Journal of Health and Social Behavior. 1978;19(1):2–21. [PubMed] [Google Scholar]
- 27.Reich JW, Zautra AJ. Experimental and measurement approaches to internal control in at-risk older adults. Journal of Social Issues. 1991;47(4):143–58. [Google Scholar]
- 28.Sherbourne CD, Stewart AL. The MOS social support survey. Social Science and Medicine. 1991;32(6):705–14. doi: 10.1016/0277-9536(91)90150-b. [DOI] [PubMed] [Google Scholar]
- 29.Rao JNK, Wu CFJ, Yue K. Some recent work on resampling methods for complex surveys. Survey Methodology (Statistics Canada, Catalogue 12-001) 1992;18(2):209–17. [Google Scholar]
- 30.Rust KF, Rao JN. Variance estimation for complex surveys using replication techniques. Statistical Methods in Medical Research. 1996;5(3):283–310. doi: 10.1177/096228029600500305. [DOI] [PubMed] [Google Scholar]
- 31.Cott CA, Gignac MAM, Badley EM. Determinants of self rated health for Canadians with chronic disease and dsability. Journal of Epidemiology and Community Health. 1999;53:731–6. doi: 10.1136/jech.53.11.731. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Nguyen HQ, Donesky-Cuenco D, Carrieri-Kohlman V. Associations between symptoms, functioning, and perceptions of mastery with global self-rated health in patients with COPD: A cross-sectional study. International Journal of Nursing Studies. 2008;45(9):1355–65. doi: 10.1016/j.ijnurstu.2007.09.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Milaneschi Y, Bandinelli S, Corsi AM, et al. Personal mastery and lower body mobility in community-dwelling older persons: the InCHIANTI Study. Journal of the American Geriatric Society. 2010;58(1):98–103. doi: 10.1111/j.1532-5415.2009.02611.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Seeman M, Seeman TE. Health behavior and person autonomy: a longitudinal study of the sense of control in illness. Journal of Health and Social Behavior. 1983;24:144–60. [PubMed] [Google Scholar]
- 35.Chen J, Millar WJ. Starting and sustaining physical activity. Health Reports. 2001;12(4):33–43. [PubMed] [Google Scholar]
- 36.Brownson RC, Baker EA, Housemann RA, et al. Environmental and policy determinants of physical activity in the United States. American Journal of Public Health. 2001;91(12):1995–2003. doi: 10.2105/ajph.91.12.1995. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Garber CE, Blissmer BJ. The challenges of exercise in older adults. In: Burbank PM, Riebe D, editors. Promoting Exercise and Behavior Change in Older Adults: Interventions With the Transtheoretical Model. New York: Springer Publishing Company, Inc; 2002. pp. 29–55. [Google Scholar]
- 38.Newsom JT, McFarland BH, Kaplan MS, et al. The health consciousness myth: implications of the near independence of major health behaviors in the North American population. Social Science and Medicine. 2005;60(2):433–7. doi: 10.1016/j.socscimed.2004.05.015. [DOI] [PubMed] [Google Scholar]
- 39.Litt MD, Kleppinger A, Judge JO. Initiation and maintenance of exercise behaviour in older women: Predictors from the social learning model. Journal of Behavioral Medicine. 2002;25(1):83–97. doi: 10.1023/a:1013593819121. [DOI] [PubMed] [Google Scholar]
- 40.Leatherdale ST, Shields M. Smoking cessation: intentions, attempts and techniques. Health Reports. 2009;20(3):31–9. [PubMed] [Google Scholar]
- 41.Brawley LR, Rejeski WJ, King AC. Promoting physical activity for older adults: the challenges for changing behaviour. American Journal of Preventive Medicine. 2003;25(3 Suppl 2):172–83. doi: 10.1016/s0749-3797(03)00182-x. [DOI] [PubMed] [Google Scholar]
- 42.Wister AV. Editorial – It’s never too late: healthy lifestyles and aging. Canadian Journal on Aging. 2003;22(2):140–50. [Google Scholar]
- 43.Prochaska JO, Velicer WF. The Transtheoretical Model of Health Behavior Change. American Journal of Health Promotion. 1997;21(1):38–48. doi: 10.4278/0890-1171-12.1.38. [DOI] [PubMed] [Google Scholar]
- 44.Wister AV. Baby Boomer Health Dynamics: How Are We Aging? Toronto: University of Toronto Press; 2005. [Google Scholar]
- 45.Newsom JT, Kaplan MS, Huguet N, et al. Health behaviors in a representative sample of older Canadians: prevalences, reported change, motivation to change, and perceived barriers. The Gerontologist. 2004;44(2):193–205. doi: 10.1093/geront/44.2.193. [DOI] [PubMed] [Google Scholar]
- 46.Gilmour H. Physically active Canadians. Health Reports. 2007;18(3):45–65. [PubMed] [Google Scholar]
- 47.Prince SA, Adamo KB, Hamel ME, et al. A comparison of direct versus self-report measures for assessing physical activity in adults: a systematic review. International Journal of Behavioral Nutrition and Physical Activity. 2008;5(1):56. doi: 10.1186/1479-5868-5-56. [DOI] [PMC free article] [PubMed] [Google Scholar]