

Abstract
Background
This study aimed to identify the systemic and cerebral hemodynamic characteristics and their roles in high-altitude headache (HAH) among young Chinese men following acute exposure.
Methods
The subjects (n = 385) were recruited in June and July of 2012. They completed case report form questionnaires, as well as heart rate (HR), blood pressure, echocardiogram and transcranial Doppler examinations at 3700 m following a two-hour plane flight. A subgroup of 129 participants was examined at two altitudes (500 and 3700 m).
Results
HAH was characterized by increased HR and cardiac output (CO) and lower saturation pulse oxygen (SpO2) (all p < 0.05). The change in tricuspid regurgitation was also different between the HAH positive (HAH+) and HAH negative (HAH-) subjects. Furthermore, the HAH+ subjects exhibited faster mean (Vm), systolic (Vs) and diastolic (Vd) velocities in the basilar artery (BA; all p < 0.05) and a faster Vd ( 25.96 ± 4.97 cm/s vs. 24.76 ± 4.76 cm/s, p = 0.045) in the left vertebral artery (VA). The bilateral VA asymmetry was also significantly different between the two groups. The pulsatility index (PI) and resistance index (RI) of left VA were lower in the HAH subjects (p < 0.05) and were negatively correlated with HAH (p < 0.05). Baseline CO and Vm in left VA (or right MCA in different regressions) were independent predictors for HAH, whereas CO/HR and ΔVd (Vd difference between bilateral VAs) were independent risk factors for HAH at 3700 m.
Conclusions
HAH was characterized, in part, by increased systemic hemodynamics and posterior cerebral circulation, which was reflected by the BA and left VA velocities, and lower arterial resistance and compliance. Furthermore, baseline CO and Vm in left VA or right MCA at sea level were independent predictors for HAH, whilst bilateral VA asymmetry may contribute to the development of HAH at high altitude.
Electronic supplementary material
The online version of this article (doi:10.1186/s10194-015-0527-3) contains supplementary material, which is available to authorized users.
Keywords: Systemic circulation, Cerebral circulation, Hemodynamic characteristics, High-altitude headache, Acute exposure
Background
High-altitude headache (HAH) is the primary critical complaint after high altitude exposure [1]. It is defined as a headache that occurs within 24 hours after ascending to 2500 m or higher [2]. HAH affects tourists’ and labor workers’ daily life and work due to its high incidence and discomfort experience [3]. HAH has also been defined as the primary symptom in diagnosis of acute mountain sickness [4].
Over the past several decades, epidemiology, clinical characteristics, risk factors, prevention and treatment aspects of HAH have been systematically studied in mountaineers [5, 2, 6, 7]. Clinical characteristics studies have showed that HAH presents as a sudden attack of migraine that is accompanied by nausea [6]. Previous studies have demonstrated that increased heart rate (HR) and self-anxiety scores, lower saturation pulse oxygen (SpO2) and a history of primary headache are all independent risk factors for HAH [8, 9]. Though oxygen inhalation, acetaminophen and aspirin have been used to treat HAH, the effects are quite often inconsistent [10, 11]. Despite accumulating evidence regarding HAH and related issues, the underlying mechanisms remain elusive [12, 13, 1].
HAH exhibits an impulsivity property [14], which may be related to the hemodynamics (or blood flow in artery) of patients. While most previous studies have focused on the risk factors and epidemiology of HAH, few of them give proper attentions to the hemodynamic characteristics of HAH [8, 9, 7]. Furthermore, most of these studies have been conducted in mountaineers, which may not reflect representative properties of HAH [5, 9, 12].
To the best of our knowledge, the hemodynamic characteristics of and their roles in HAH has not been fully uncovered. Thus, we postulate that hemodynamics especially cerebral hemodynamic parameters are related HAH and they may be predictors for HAH. Therefore, we performed this large sample size cohort study to explore the hemodynamic characteristics of HAH via examinations of the systemic and cerebral hemodynamic parameters using echocardiogram and transcranial Doppler sonography, respectively, following acute high altitude exposure (within 24 h after arrival at 3700 m) to facilitate our understanding of the disease process and provide insight into the specific phenotypes associated with the disease course.
Methods
Participants and procedures
Participants
Three hundred eighty-five participants were recruited in June and July of 2012 according to specific inclusion and exclusion criteria. The inclusion criteria were as follows: healthy males between the ages of 18 and 60 years who had no high-altitude exposure in recent two years. Individuals with any of the following conditions were excluded: neuropsychosis, cerebrovascular diseases, cardiovascular diseases, respiratory diseases, malignant tumors and liver or kidney disorders.
The study was reviewed and approved by the Ethics Committee of Xinqiao Hospital of Third Military Medical University. The study was thoroughly explained to all subjects who agreed to participate, and all volunteers signed informed consent forms prior to study participation.
Procedures
The subjects were transported to an altitude of 3700 m by plane over two hours of travel in June and July of 2012. None of the subjects drinks coffee regularly. The coffee, tea, and other caffeine-containing drinks as well as alcohol were avoided before the examinations. Baseline measurements of systemic and cerebral hemodynamic parameters were examined one week prior to the departure at sea level (Chengdu, 500 m) in a subgroup of 129 participants. The participants will receive regular training after a three days’ rest. They did the daily life activities and avoided any heavy exercises or physical labor in the first 72 hours at 3700 m. The field trials were performed within 18 to 24 hours after their arrivals at 3700 m. Structured case report questionnaires were used to record the subjects’ demographic information (i.e., age, body mass index (BMI), smoking and alcohol consumption), primary headache history [None of them takes medication regularly due to primary headache. However, severe headache (HAH) subjects were treated with NSAIDs or Sanlietong (Taiji medicine, Xi’an, China) as necessary at 3700 m] and HAH symptoms (0 = no headache; 1 = mild headache; 2 = moderate headache; 3 = severe headache).
Measurements of systemic hemodynamic parameters
The subjects’ systolic blood pressure (SBP), diastolic blood pressure (DBP), HR and SpO2 were measured using a sphygmomanometer (HEM-6200, OMRON, China) and a pulse oximeter (NONIN-9550, Nonin Onyx, USA) after the subjects had sat at rest for 30 min. Each subject received an echocardiogram examination (ultrasonography system, CX50, Philips, USA) that involved measurements of the end-diastolic internal diameters of the left atrium (LA), left ventricle (LV), right atrium (RA), right ventricle (RV) and pulmonary artery (PA), in addition to the stroke volume (SV), cardiac output (CO) and ejection fraction (EF).
Measurements of cerebral hemodynamic parameters
The examinations at both altitudes were performed in the morning after an overnight fast and caffeine containing drinks were avoided.
Transcranial Doppler sonography examinations were performed by the same technician using an ultrasonography system with a 2 Hz probe (EME TC2021-III, NICOLET, USA). For each subject, the following parameters were recorded: the mean velocity (Vm), systolic velocity (Vs), diastolic velocity (Vd), pulsatility index (PI) and resistance index (RI). These measurements were taken in the bilateral middle cerebral artery (MCA) for anterior circulation and in the vertebral artery (VA) and basilar artery (BA) for posterior circulation.
The asymmetry of the MCA and VA was calculated as ΔV = left velocity - right velocity for each lateral MCA or VA, whereas the asymmetry index (AI) was calculated as AI = ΔV/ [(left Vm + right Vm)/2]. The cerebrovascular conductance index was calculated as the Vm_MCA/mean arterial blood pressure.
Statistical analysis
The case report forms were excluded if the demographic information was not completed, the velocity could not be identified at the depths previously described or the systemic hemodynamic parameters were not measured.
The normally distributed measurement variables (age, BMI, SBP, DBP, SpO2, HR, echocardiography parameters and velocities, PIs and RIs of the BA, MCAs and VAs) were expressed as the mean ± standard deviation (SD). The non-normally distributed variables were presented as the medians (interquartile range). The enumerated data are expressed as the rate of occurrence (%).
The normally distributed variables for the systemic and cerebral circulation measurements were compared using a paired Student’s t-test between the 500 and 3700 m altitudes and were analyzed using an independent samples t-test between the HAH positive (HAH+) and HAH negative (HAH-) groups at both altitudes. The asymmetries, AIs and tricuspid regurgitation measurements were compared using a Mann–Whitney U test. The relationships between HAH and the previously described parameters at 500 m and 3700 m were analyzed using Spearman’s correlations. Variables with a p < 0.05 in correlation analyses or significant difference between HAH+ and HAH- groups were included in univariate logistic regression. Adjusted logistic analyses were used to identify independent predictors or risk factors for HAH after univariate logistic regression (Fig 1). Variables with colinearity were analyzed in different models (adjusted by primary variables or calculated variables respectively) to reduce the bias.
Fig. 1.
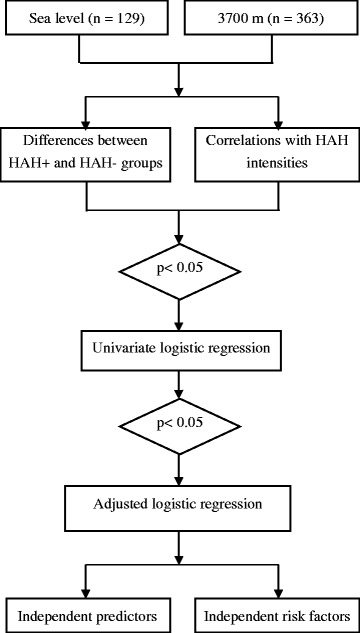
The fluidogram of the statistical analysis
The statistical analyses were performed using SPSS 19.0 software for Windows. P ≤ 0.05 was considered statistically significant. Statisticians from Third Military Medical University were consulted regarding the statistical methods and results.
Results
Clinical characteristics of the subjects
Three hundred eighty-five subjects received both echocardiography and transcranial Doppler examinations at 3700 m of elevation (363 subjects had completely valid transcranial Doppler and echocardiography parameters). Baseline measurements at 500 m were also recorded among 129 individuals. The subjects in this study were characterized by a mean age of 23.35 ± 4.37 years and a mean BMI of 21.81 ± 2.50 kg/m2. The ethnicity of the population was primarily Han Chinese (83.2%). Overall, in our study, the incidence of HAH following acute exposure to 3700 m was 75.2% (273 of 363).
Alterations in systemic and cerebral hemodynamics
Both systemic and cerebral circulations were dramatically altered following acute exposure to high altitude from sea level. However, the blood pressure parameters, including the SBP, DBP, pulse pressure and mean arterial blood pressure, did not significantly increase after the acute exposure. The SpO2 decreased from 98.34 ± 1.06% to 88.72 ± 2.71% (p < 0.001). The LA, RA and RV all significantly decreased (all p < 0.001). However, the EF and CO significantly increased, as well as the velocity in the bilateral MCAs. In VAs and BA, the Vd exhibited a significant increase. However, the VAs asymmetries did not dramatically change. The changes in the hemodynamic parameters are summarized in Table 1.
Table 1.
Alterations in systemic and cerebral hemodynamics (N = 129)
| Sea level | 3700 m | p value | |
|---|---|---|---|
| Systemic hemodynamics | |||
| SBP | 116.32 ± 15.24 | 115.84 ± 11.84 | 0.782 |
| DBP | 74.65 ± 10.93 | 76.24 ± 9.40 | 0.156 |
| ΔBP | 41.67 ± 11.71 | 39.61 ± 8.05 | 0.131 |
| MAP | 88.54 ± 11.25 | 89.44 ± 9.55 | 0.444 |
| HR | 63.58 ± 10.19 | 83.98 ± 11.90 | <0.001** |
| SpO2 | 98.34 ± 1.06 | 88.72 ± 2.71 | <0.001** |
| LA | 30.91 ± 1.73 | 30.00 ± 1.92 | <0.001** |
| LV | 46.47 ± 2.45 | 46.15 ± 2.04 | 0.184 |
| RA | 35.70 ± 2.23 | 34.21 ± 2.15 | <0.001** |
| RV | 35.49 ± 2.08 | 33.72 ± 2.42 | <0.001** |
| PA | 20.24 ± 1.60 | 19.92 ± 1.60 | 0.097 |
| EF | 62.94 ± 5.49 | 66.56 ± 3.92 | <0.001** |
| SV | 65.24 ± 12.22 | 67.30 ± 8.31 | 0.088 |
| CO | 4.16 ± 0.95 | 5.32 ± 1.09 | <0.001** |
| Tricuspid regurgitation | 0.500 (1.00) | 0.500(0.500) | 0.885 |
| Cerebral hemodynamics | |||
| Left side MCA | |||
| Vm | 62.08 ± 10.39 | 65.79 ± 11.78 | <0.001** |
| Vs | 95.95 ± 14.60 | 99.80 ± 15.93 | 0.002** |
| Vd | 42.69 ± 7.91 | 46.47 ± 9.07 | <0.001** |
| PI | 0.867 ± 0.133 | 0.817 ± 0.133 | <0.001** |
| RI | 0.554 ± 0.048 | 0.534 ± 0.048 | <0.001** |
| Left side VA | |||
| Vm_ | 32.77 ± 5.14 | 35.20 ± 5.83 | <0.001** |
| Vs_ | 50.70 ± 7.50 | 51.57 ± 7.91 | 0.233 |
| Vd_ | 21.91 ± 4.095 | 24.82 ± 4.86 | <0.001** |
| PI | 0.895 ± 0.181 | 0.770 ± 0.168 | <0.001** |
| RI | 0.570 ± 0.067 | 0.516 ± 0.061 | <0.001** |
| Right side MCA | |||
| Vm | 58.79 ± 10.18 | 63.25 ± 11.58 | <0.001** |
| Vs | 90.50 ± 14.18 | 94.71 ± 15.01 | <0.001** |
| Vd | 40.35 ± 7.49 | 44.55 ± 9.04 | <0.001** |
| PI | 0.864 ± 0.150 | 0.804 ± 0.130 | <0.001** |
| RI | 0.556 ± 0.055 | 0.530 ± 0.050 | 0.293 |
| Right side VA | |||
| Vm | 34.33 ± 4.77 | 36.47 ± 5.73 | <0.001** |
| Vs | 50.60 ± 6.55 | 51.78 ± 7.83 | 0.058 |
| Vd | 23.24 ± 4.12 | 25.90 ± 4.55 | <0.001** |
| PI | 0.808 ± 0.162 | 0.715 ± 0.117 | <0.001** |
| RI | 0.539 ± 0.061 | 0.499 ± 0.048 | <0.001** |
| BA | |||
| Vm | 39.66 ± 7.75 | 41.85 ± 9.58 | 0.002** |
| Vs | 67.93 ± 13.57 | 66.19 ± 13.46 | 0.117 |
| Vd | 25.07 ± 5.85 | 28.59 ± 7.71 | <0.001** |
| PI | 1.093 ± 0.251 | 0.920 ± 0.220 | <0.001** |
| RI | 0.627 ± 0.068 | 0.567 ± 0.073 | <0.001** |
| Asymmetry of the bilateral VAs | |||
| ΔVs | 0.0 (11.0) | 0.0 (12.0) | 0.645 |
| ΔVd | −1.0 (6.0) | −1.0 (6.0) | 0.623 |
| ΔVm | −1.0 (7.0) | −2.0 (8.0) | 0.529 |
| AI% | −3.5 (20.2) | −2.9 (18.1) | 0.190 |
| Conduction | |||
| CVCi | 0.695 ± 0.145 | 0.730 ± 0.149 | 0.011* |
BA: basilar artery; CO: cardiac output; CVCi : cerebrovascular conductance index; DBP: diastolic blood pressure; EF: ejection fraction; HAH: high-altitude headache; HAH+: HAH positive or with HAH; HAH-: HAH negative or without HAH;HR: heart rate; LA: end-diastolic internal diameters of left atrium; LV: end-diastolic internal diameters of left ventricle; MCA: middle cerebral artery; PA: end-diastolic internal diameters of pulmonary artery; PI: pulsatility index; RA: end-diastolic internal diameters of right atrium; RI: resistance index; RV: end-diastolic internal diameters of right ventricle; SBP: systolic blood pressure;SpO2: saturation pulse oxygen; SV: stroke volume; VA: vertebral artery; Vs: systolic velocity; Vd: diastolic velocity; Vm: mean velocity;ΔVs: difference in systolic velocity between bilateral isonym cerebral arteries; ΔVd: difference in diastolic velocity between bilateral isonym cerebral arteries;ΔVm: Difference in mean velocity between bilateral isonym cerebral arteries. Cerebrovascular conductance index (CVCi) = Vm_MCA/MAP
#: N = 129;
*p is 0.05 or less, **p is 0.01 or less
Most of the cerebral hemodynamic parameters altered dramatically from sea level to 3700 m and systemic hemodynamic parameters altered dramatically in part
Clinical and hemodynamic characteristics of HAH at 3700 m
Only age (p = 0.044) was significantly higher in the HAH+ group as compared with the HAH- group regarding demographic data. The HAH+ patients were characterized by increased HR (87.96 ± 13.02 vs. 84.41 ± 13.11 beats per min, p = 0.026) and decreased SpO2 (87.94 ± 3.19 vs. 88.70 ± 2.98%, p = 0.048). Regarding blood pressure, there was no significant difference between the HAH+ and HAH- groups in the SBP, DBP, pulse pressure or mean arterial blood pressure. Although the LA, LV, RA, RV, PA, EF, SV and tricuspid regurgitation were not significantly different in the HAH+ subjects compared with the HAH- subjects (all p > 0.05), the CO was significantly increased in the HAH+ group (p = 0.001).
Anterior circulation, which was assessed via measurements of velocities in MCAs, was similar in the HAH+ and HAH- groups in bilateral MCAs (all p > 0.05). The PIs and RIs in the right and left MCA were not different between the two groups. For posterior circulation, the velocities in BA, including Vs (65.46 ± 11.54 vs. 68.81 ± 14.84, p = 0.028), Vd (28.61 ± 7.46 vs. 30.47 ± 7.52, p = 0.042) and Vm (41.42 ± 8.64 vs. 44.18 ± 9.74, p = 0.017), were significantly different in the HAH- group as compared with the HAH+ group, respectively. Similar to the MCA, the PI (p = 0.151) and RI (p = 0.292) of the BA were not significantly different between the HAH+ and HAH- groups. Furthermore, the Vd in left VA was significantly increased in the HAH+ group compared with the HAH- group (25.96 ± 4.97 vs. 24.76 ± 4.76 cm/s, p = 0.045), whereas the Vs and Vm were not significantly different between the two groups. Additionally, the HAH+ patients also exhibited a lower RI and PI in the left VA (p = 0.040 and 0.025, respectively). However, in the right VA, the velocities and pulsate indexes showed no differences between HAH+ group and HAH- one (all p > 0.05, Table 2).
Table 2.
Differences between HAH+ and HAH- groups in demographics, systemic and cerebral hemodynamics (N = 363)
| Headachea | HAH- | HAH+ | HAH intensities | p (H+ vs. H-) | ||
|---|---|---|---|---|---|---|
| Cases(n) | (90) | (273) | Mild (215) | Moderate (52) | Sever (6) | |
| Demographic factors | ||||||
| Age | 22.59 ± 3.95 | 23.60 ± 4.48 | 23.12 ± 4.26 | 25.47 ± 4.99 | 25.00 ± 3.69 | 0.044* |
| BMI | 21.52 ± 2.11 | 21.90 ± 2.61 | 21.85 ± 2.55 | 21.96 ± 2.89 | 23.56 ± 2.09 | 0.199 |
| Smoking(yes) | 20(22.2%) | 66(24.2%) | 52(24.2%) | 11(21.2%) | 3(50.0%) | 0.705 |
| Alcohol consumption(yes) | 54(60.0%) | 159(58.2%) | 126 (58.6%) | 28(53.8%) | 5(83.3%) | 0.796 |
| Systemic hemodynamics | ||||||
| SBP | 117.28 ± 11.62 | 118.66 ± 12.03 | 118.84 ± 12.38 | 118.17 ± 11.04 | 116.67 ± 7.76 | 0.340 |
| DBP | 77.52 ± 10.83 | 78.86 ± 9.97 | 78.89 ± 10.21 | 78.92 ± 9.26 | 77.33 ± 8.43 | 0.279 |
| ΔBP | 39.76 ± 7.14 | 39.80 ± 6.59 | 39.94 ± 7.04 | 39.25 ± 4.54 | 39.33 ± 5.24 | 0.958 |
| MAP | 90.77 ± 10.57 | 92.13 ± 10.24 | 92.21 ± 10.47 | 92.01 ± 9.65 | 90.44 ± 7.83 | 0.280 |
| HR | 84.41 ± 13.11 | 87.96 ± 13.02 | 87.35 ± 12.65 | 89.35 ± 13.26 | 98.00 ± 20.66 | 0.026* |
| SpO2 | 88.70 ± 2.98 | 87.94 ± 3.19 | 88.16 ± 3.01 | 87.06 ± 3.81 | 87.83 ± 3.06 | 0.048* |
| LA | 29.82 ± 2.12 | 29.70 ± 2.18 | 29.75 ± 1.99 | 29.40 ± 2.84 | 30.33 ± 2.50 | 0.632 |
| LV | 45.78 ± 2.27 | 46.00 ± 2.25 | 46.04 ± 2.21 | 45.85 ± 2.44 | 45.83 ± 2.32 | 0.425 |
| RA | 33.98 ± 2.04 | 34.10 ± 2.32 | 34.14 ± 2.27 | 34.06 ± 2.56 | 33.17 ± 2.32 | 0.661 |
| RV | 33.48 ± 2.24 | 33.70 ± 2.56 | 33.78 ± 2.56 | 33.50 ± 2.60 | 32.50 ± 2.07 | 0.469 |
| PA | 19.83 ± 1.14 | 19.95 ± 1.42 | 19.93 ± 1.42 | 19.98 ± 1.48 | 20.33 ± 1.03 | 0.452 |
| EF | 66.38 ± 4.28 | 67.16 ± 4.72 | 67.29 ± 4.82 | 66.87 ± 4.40 | 64.83 ± 3.31 | 0.165 |
| SV | 65.92 ± 8.96 | 67.32 ± 9.72 | 67.57 ± 9.79 | 66.66 ± 9.42 | 64.17 ± 10.63 | 0.230 |
| CO | 5.16 ± 1.14 | 5.60 ± 1.02 | 5.60 ± 1.03 | 5.65 ± 1.02 | 5.60 ± .663 | 0.001** |
| Tricuspid regurgitation | 0.50(0.80) | 0.50(0.60) | 0.50(0.60) | 0.50(0.80) | 0.40(0.68) | 0.135 |
| Cerebral hemodynamics | ||||||
| Left side MCA | ||||||
| Vm | 67.46 ± 12.18 | 67.41 ± 11.74 | 66.91 ± 10.87 | 69.35 ± 14.87 | 68.50 ± 11.47 | 0.973 |
| Vs | 102.17 ± 14.94 | 101.41 ± 15.91 | 100.79 ± 15.15 | 103.92 ± 18.83 | 102.00 ± 15.82 | 0.693 |
| Vd | 48.0 ± 10.12 | 47.96 ± 9.10 | 47.51 ± 8.37 | 49.46 ± 11.67 | 51.00 ± 8.60 | 0.964 |
| PI | 0.820 ± 0.169 | 0.800 ± 0.130 | 0.802 ± 0.127 | 0.799 ± 0.141 | 0.750 ± 0.130 | 0.260 |
| RI | 0.531 ± 0.063 | 0.527 ± 0.0490 | 0.528 ± 0.048 | 0.526 ± 0.051 | 0.499 ± 0.057 | 0.532 |
| Left side VA | ||||||
| Vm | 35.18 ± 5.57 | 36.38 ± 6.19 | 35.93 ± 5.66 | 37.63 ± 6.59 | 41.67 ± 14.40 | 0.103 |
| Vs | 51.28 ± 7.05 | 52.16 ± 8.49 | 51.75 ± 7.93 | 53.19 ± 9.20 | 57.83 ± 17.59 | 0.374 |
| Vd | 24.76 ± 4.76 | 25.96 ± 4.97 | 25.46 ± 4.49 | 27.35 ± 5.08 | 32.00 ± 11.93 | 0.045* |
| PI | 0.765 ± 0.159 | 0.727 ± 0.153 | 0.738 ± 0.153 | 0.690 ± 0.150 | 0.640 ± 0.102 | 0.040* |
| RI | 0.517 ± 0.065 | 0.500 ± 0.061 | 0.505 ± 0.058 | 0.482 ± 0.070 | 0.454 ± 0.053 | 0.025* |
| Right side MCA | ||||||
| Vm | 63.51 ± 13.67 | 64.46 ± 11.45 | 64.24 ± 11.26 | 64.87 ± 11.57 | 68.67 ± 17.61 | 0.518 |
| Vs | 95.59 ± 17.61 | 96.24 ± 15.67 | 96.17 ± 15.55 | 96.13 ± 15.65 | 99.83 ± 22.29 | 0.740 |
| Vd | 45.11 ± 10.96 | 45.75 ± 8.73 | 45.53 ± 8.52 | 46.12 ± 8.95 | 50.67 ± 13.74 | 0.573 |
| PI | 0.812 ± 0.144 | 0.792 ± 0.124 | 0.796 ± 0.121 | 0.780 ± 0.125 | 0.734 ± 0.190 | 0.191 |
| RI | 0.530 ± 0.053 | 0.526 ± 0.051 | 0.527 ± 0.051 | 0.521 ± 0.047 | 0.493 ± 0.076 | 0.440 |
| Right side VA | ||||||
| Vm | 37.27 ± 6.18 | 37.27 ± 6.02 | 37.00 ± 5.80 | 38.63 ± 6.89 | 35.17 ± 4.66 | 0.991 |
| Vs | 52.51 ± 7.69 | 52.26 ± 8.29 | 52.11 ± 8.09 | 53.42 ± 9.21 | 47.50 ± 6.06 | 0.800 |
| Vd | 26.72 ± 5.09 | 26.55 ± 4.74 | 26.26 ± 4.56 | 27.75 ± 5.33 | 26.33 ± 4.89 | 0.764 |
| PI | 0.716 ± 0.208 | 0.693 ± 0.117 | 0.702 ± 0.117 | 0.669 ± .114 | 0.606 ± 0.056 | 0.202 |
| RI | 0.500 ± 0.119 | 0.491 ± 0.053 | 0.494 ± 0.052 | 0.480 ± .053 | 0.448 ± 0.037 | 0.317 |
| BA | ||||||
| Vm | 41.42 ± 8.64 | 44.18 ± 9.74 | 43.80 ± 9.42 | 46.33 ± 10.91 | 38.83 ± 8.06 | 0.017* |
| Vs | 65.46 ± 11.54 | 68.81 ± 14.84 | 68.60 ± 14.32 | 70.81 ± 16.13 | 59.17 ± 19.63 | 0.028* |
| Vd | 28.61 ± 7.46 | 30.47 ± 7.52 | 30.07 ± 7.31 | 32.29 ± 8.31 | 28.83 ± 6.27 | 0.042* |
| PI | 0.914 ± 0.224 | 0.879 ± 0.193 | 0.890 ± 0.192 | 0.844 ± 0.183 | 0.760 ± .262 | 0.151 |
| RI | 0.564 ± 0.078 | 0.554 ± 0.068 | 0.559 ± 0.066 | 0.542 ± 0.069 | 0.496 ± .086 | 0.292 |
| Asymmetry of the bilateral VAs | ||||||
| ΔVs | −1.00 (8.00) | 0. 00 (9.00) | 0.00(9.00) | 0.00 (10.50) | 5.00 (28.5) | 0.126 |
| ΔVd | −3.00 (6.25) | −1.00 (6.00) | −1.00(7.00) | −1.00 (3.75) | 2.00 (18.5) | 0.010* |
| ΔVm | −2.50 (8.00) | −1.00 (6.00) | −1.00(6.00) | −1.00 (4.75) | 1.00 (23.75) | 0.046* |
| AI% | −6.6(22.0) | −2.7 (18.0) | −2.9(18.4) | −2.1(13.8) | 2.8 (52.2) | 0.040* |
| Conduction | ||||||
| CVCi | 0.729 ± 0.145 | 0.724 ± 0.140 | 0.719 ± 0.135 | 0.737 ± 0.153 | 0.767 ± 0.191 | 0.758 |
*p is 0.05 or less, **p is 0.01 or less
HAH was characterized with higher velocity in posterior cerebral circulation and higher HR but lower SpO2
The asymmetry of the bilateral VAs, including the ΔVd (p = 0.010), ΔVm (p = 0.046) and AI (p = 0.040), in the HAH patients was significantly different than the HAH- subjects. The cerebrovascular conductance index (0.724 ± 0.140 vs.0.729 ± 0.145, respectively, p = 0.758) was similar in the HAH+ and HAH- subjects (Table 2).
The Spearman’s correlation analyses demonstrated that age (r = 0.178, p = 0.001), HR (r = 0.143, p = 0.006) and CO (r = 0.175, p = 0.001) exhibited significantly positive relationships with the HAH severity, whereas the SpO2 (r = −0.148, p = 0.005) exhibited an inverse relationship. The other parameters in systemic hemodynamics were not closely associated with HAH (all p > 0.05). The anterior circulation parameters, including the velocities, PIs and RIs in the bilateral MCA, had no associations with HAH severity. With the exception of the Vs, the other parameters (Vm, Vd, PI and RI) of the BA exhibited significant associations with HAH (p was 0.023, 0.021, 0.045 and 0.042, respectively). On the left side VA, the Vd (r = 0.157, p = 0.003) and Vm (r = 0.120, p = 0.022) exhibited positive relationships with HAH, whereas the PI (r = −0.152, p = 0.004) and RI (r = −0.166, p = 0.001) were negatively correlated with HAH. The parameters on the right side of the VA were not as closely correlated with HAH. Furthermore, associations between VA asymmetries and HAH were also identified in the bilateral VAs: ΔV of Vd (r = 0.137, p = 0.009), ΔV of Vm (r = 0.105, p = 0.046) and AI (r = 0.106, p = 0.043). The relationships between HAH and the hemodynamic parameters are shown in Table 3.
Table 3.
Relationships between HAH and demographic, systemic and cerebral hemodynamic parameters (N = 363)
| Headache score | |||||
|---|---|---|---|---|---|
| r | p | r | p | ||
| Demographic factors | PI | −0.152 | 0.004** | ||
| Age | 0.178 | 0.001** | RI | −0.166 | 0.001** |
| BMI | 0.075 | 0.155 | |||
| Right side MCA | |||||
| Systemic hemodynamics | Vm | 0.078 | 0.136 | ||
| SBP | 0.031 | 0.561 | Vs | 0.055 | 0.297 |
| DBP | 0.031 | 0.560 | Vd | 0.086 | 0.103 |
| ΔBP | 0.009 | 0.865 | PI | −0.099 | 0.059 |
| MAP | 0.033 | 0.535 | RI | −0.087 | 0.097 |
| HR | 0.143 | 0.006** | |||
| SpO2 | −0.148 | 0.005** | Right side VA | ||
| LA | −0.035 | 0.507 | Vm | 0.039 | 0.455 |
| LV | 0.027 | 0.610 | Vs | <0.001 | 0.997 |
| RA | 0.010 | 0.851 | Vd | 0.036 | 0.499 |
| RV | 0.001 | 0.992 | PI | −0.083 | 0.115 |
| PA | 0.058 | 0.275 | RI | −0.065 | 0.215 |
| EF | 0.045 | 0.390 | |||
| SV | 0.035 | 0.506 | BA | ||
| CO | 0.175 | 0.001** | Vm | 0.119 | 0.023* |
| Tricuspid regurgitation | 0.044 | 0.400 | Vs | 0.077 | 0.141 |
| Vd | 0.121 | 0.021* | |||
| Cerebral hemodynamics | PI | −0.105 | 0.045* | ||
| Left side MCA | RI | −0.107 | 0.042* | ||
| Vm | 0.033 | 0.536 | |||
| Vs | 0.018 | 0.733 | Asymmetry of VAs | ||
| Vd | 0.039 | 0.454 | ΔVs | 0.080 | 0.130 |
| PI | −0.039 | 0.458 | ΔVd | 0.137 | 0.009** |
| RI | −0.050 | 0.345 | ΔVm | 0.105 | 0.046* |
| AI% | 0.106 | 0.043* | |||
| Left side VA | |||||
| Vm | 0.120 | 0.022* | Conduction | ||
| Vs | 0.067 | 0.203 | CVCi | 0.019 | 0.716 |
| Vd | 0.157 | 0.003** | |||
*p is 0.05 or less, **p is 0.01 or less
HAH was positively associated with HR, CO and cerebral velocities while it negatively correlated with SpO2, PIs and RIs in BA and left side VA
Risk factors for HAH at 3700 m
Univariate logistic regression was performed for variable with a p < 0.05 in correlation analyses or significant difference between HAH+ and HAH- groups. HR, SpO2, CO, Vd, PI and RI of left side VA, velocities in BA (Vm, Vd) and ΔVd were risk factors for HAH. After adjusted regression analyses, only HR (or CO) and ΔVd were independent risk factors for HAH (Table 4).
Table 4.
Univariate and adjusted logistic regression for variables at 3700 m (N = 363)
| Risk factors | β-coefficient | Odds ratio | (95% CI) | p value | ||
|---|---|---|---|---|---|---|
| Lower | Upper | |||||
| Univariate logistic regression | ||||||
| HR | 0.022 | 1.022 | 1.003 | 1.042 | 0.027* | |
| SpO2 | −0.081 | 0.922 | 0.851 | 1.000 | 0.049* | |
| CO | 0.422 | 1.524 | 1.195 | 1.944 | 0.001** | |
| Left VA | Vd | 0.052 | 1.053 | 1.001 | 1.108 | 0.046* |
| PI | −1.562 | 0.210 | 0.047 | 0.944 | 0.042* | |
| RI | −4.476 | 0.011 | 0.000 | 0.591 | 0.026* | |
| BA | Vm | 0.032 | 1.033 | 1.005 | 1.061 | 0.018* |
| Vd | 0.044 | 1.036 | 1.001 | 1.071 | 0.035* | |
| Asymmetry of VAs | ΔVd | 0.063 | 1.065 | 1.011 | 1.122 | 0.018* |
| Adjusted logistic regression | ||||||
| Model 1 | ||||||
| HR | 0.025 | 1.025 | 1.005 | 1.045 | 0.012* | |
| Model 2 | ||||||
| HR | 0.023 | 1.023 | 1.003 | 1.044 | 0.026* | |
| ΔVd | 0.065 | 1.068 | 1.013 | 1.126 | 0.015* | |
| Model3 | ||||||
| CO | 0.417 | 1.517 | 1.189 | 1.937 | 0.001** | |
| ΔVd | 0.063 | 1.065 | 1.009 | 1.124 | 0.022* | |
*p is 0.05 or less, **p is 0.01 or less
Model 1: Adjusted by primary variables (SpO2, Vd in left side VA and BA);
Model 2: Adjusted by primary variables and an asymmetry data (ΔVd);
Model 3: Avoided the colinearity between HR and CO, indicated that CO and ΔVd were independent risk factors for HAH;
We just listed the variable with a p < 0.05
Associations between hemodynamic parameters and HAH in a subgroup of 129 subjects
In the baseline parameters, CO, Vm, PI and RI in left side VA, velocities [Vm (60.20 ± 10.37 vs. 54.29 ± 7.03 cm/s, p = 0.004), Vs (92.11 ± 14.53 vs. 85.64 ± 10.46 cm/s, p = 0.023) and Vd (41.42 ± 7.60 vs. 37.19 ± 5.50 cm/s, p = 0.005)] in right MCA were significant different between HAH+ and HAH- groups. Furthermore, CO showed a positive relationship with HAH (Table 5).
Table 5.
Associations between baseline parameters and HAH (N = 129)
| Differences between HAH+ | Correlation with HAH intensities | ||||
|---|---|---|---|---|---|
| and HAH- groups | |||||
| Headache Cases(n) | HAH-(31) | HAH+(98) | p value | r | p value |
| Demographic factors | |||||
| Age | 22.71 ± 3.21 | 23.13 ± 4.31 | 0.616 | 0.093 | 0.297 |
| BMI | 21.41 ± 1.67 | 22.07 ± 2.52 | 0.175 | 0.153 | 0.084 |
| Smoking(yes) | 7(22.5%) | 23(23.5%) | 0.919 | / | / |
| Alcohol consumption(yes) | 21(67.7%) | 58(59.2%) | 0.396 | / | / |
| Primary headache(yes) | 4(12.9%) | 23(23.5%) | 0.209 | / | / |
| Systemic hemodynamic | |||||
| SBP | 118.35 ± 10.81 | 117.32 ± 12.37 | 0.676 | 0.018 | 0.843 |
| DBP | 74.00 ± 9.22 | 75.18 ± 11.31 | 0.598 | 0.059 | 0.509 |
| ΔBP | 44.35 ± 6.47 | 42.13 ± 6.37 | 0.094 | −0.137 | 0.122 |
| MAP | 88.78 ± 9.29 | 89.22 ± 11.28 | 0.843 | 0.061 | 0.490 |
| HR | 63.32 ± 11.35 | 64.42 ± 10.10 | 0.607 | 0.008 | 0.930 |
| SpO2 | 98.35 ± 1.02 | 98.30 ± 1.10 | 0.793 | 0.038 | 0.670 |
| LA | 31.06 ± 1.55 | 30.87 ± 1.78 | 0.581 | −0.062 | 0.484 |
| LV | 45.81 ± 2.14 | 46.71 ± 2.50 | 0.071 | 0.183 | 0.037* |
| RA | 35.45 ± 1.98 | 35.78 ± 2.27 | 0.478 | 0.153 | 0.082 |
| RV | 35.29 ± 1.85 | 35.55 ± 2.13 | 0.542 | 0.109 | 0.217 |
| PA | 20.06 ± 1.46 | 20.30 ± 1.63 | 0.481 | 0.094 | 0.288 |
| EF | 62.90 ± 5.98 | 63.10 ± 5.34 | 0.865 | 0.002 | 0.978 |
| SV | 62.53 ± 16.31 | 66.55 ± 10.61 | 0.113 | 0.088 | 0.322 |
| CO | 3.79 ± 1.01 | 4.33 ± 0.93 | 0.007** | 0.177 | 0.045* |
| Tricuspid regurgitation | 0.50(1.00) | 0.45(1.00) | 0.372 | −0.030 | 0.739 |
| Cerebral hemodynamic | |||||
| Left side MCA | |||||
| Vm | 59.61 ± 8.24 | 63.24 ± 10.92 | 0.091 | 0.060 | 0.501 |
| Vs | 93.48 ± 12.13 | 97.00 ± 15.21 | 0.246 | 0.062 | 0.488 |
| Vd | 40.93 ± 6.20 | 43.62 ± 8.37 | 0.102 | 0.058 | 0.513 |
| PI | 0.889 ± 0.154 | 0.852 ± 0.125 | 0.180 | −0.004 | 0.960 |
| RI | 0.562 ± 0.051 | 0.550 ± 0.047 | 0.221 | −0.015 | 0.862 |
| Left side VA | |||||
| Vm | 30.94 ± 5.25 | 33.23 ± 4.97 | 0.029* | 0.171 | 0.053 |
| Vs | 49.64 ± 7.11 | 50.82 ± 7.56 | 0.444 | 0.083 | 0.351 |
| Vd | 20.68 ± 4.17 | 22.26 ± 3.95 | 0.056 | 0.142 | 0.107 |
| PI | 0.957 ± 0.193 | 0.873 ± 0.169 | 0.022* | −0.150 | 0.090 |
| RI | 0.594 ± 0.075 | 0.561 ± 0.056 | 0.010* | −0.159 | 0.072 |
| Right side MCA | |||||
| Vm | 54.29 ± 7.03 | 60.20 ± 10.37 | 0.004** | 0.155 | 0.080 |
| Vs | 85.64 ± 10.46 | 92.11 ± 14.53 | 0.023* | 0.125 | 0.157 |
| Vd | 37.19 ± 5.50 | 41.42 ± 7.60 | 0.005** | 0.114 | 0.200 |
| PI | 0.888 ± 0.150 | 0.855 ± 0.146 | 0.276 | −0.078 | 0.380 |
| RI | 0.574 ± 0.062 | 0.586 ± 0.053 | 0.592 | −0.093 | 0.292 |
| Right side VA | |||||
| Vm | 32.77 ± 5.30 | 34.84 ± 4.40 | 0.032 | 0.126 | 0.155 |
| Vs | 49.38 ± 6.88 | 51.03 ± 6.33 | 0.220 | 0.073 | 0.411 |
| Vd | 22.09 ± 4.29 | 23.64 ± 3.95 | 0.065 | 0.110 | 0.216 |
| PI | 0.849 ± 0.160 | 0.793 ± 0.156 | 0.086 | −0.141 | 0.110 |
| RI | 0.555 ± 0.055 | 0.534 ± 0.061 | 0.081 | −0.134 | 0.130 |
| BA | |||||
| Vm | 37.55 ± 7.36 | 40.50 ± 7.80 | 0.065 | 0.154 | 0.082 |
| Vs | 66.29 ± 13.65 | 68.53 ± 13.87 | 0.433 | 0.054 | 0.546 |
| Vd | 23.48 ± 5.08 | 25.69 ± 5.97 | 0.066 | 0.139 | 0.115 |
| PI | 0.964 ± 0.210 | 0.885 ± 0.197 | 0.092 | −0.104 | 0.239 |
| RI | 0.644 ± 0.055 | 0.621 ± .0714 | 0.108 | −0.074 | 0.404 |
| Asymmetry of bilateral VAs | |||||
| ΔVs | 2.0 (15.0) | 0.0(9.25) | 0.795 | 0.042 | 0.634 |
| ΔVd | 0.0(6.0) | −2.0 (6.0) | 0.703 | 0.017 | 0.851 |
| ΔVm | −2.0 (8.0) | −1.0 (7.0) | 0.934 | 0.064 | 0.468 |
| AI% | −0.061 (0.224) | −0.034(0.200) | 0.815 | 0.075 | 0.398 |
| Conduction | |||||
| CVCi | 0.648 ± 0.103 | 0.704 ± 0.145 | 0.048* | 0.097 | 0.275 |
/:binary variables that were not analyzed by Spearman’s correlation
*p is 0.05 or less, **p is 0.01 or less
Univariate logistic regression revealed that CO, Vm in both VAs and velocities in right side MCA were risk factors for HAH. However, adjusted analyses showed that CO (adjusted by Vs and Vd of right side MCA, OR: 1.613, p = 0.036 or adjusted by Vm of right side MCA OR: 1.811, p = 0.024) and Vm in right MCA (OR: 1.066, p = 0.011) or left VA (OR: 1.099, p = 0.035) were still independent predictors for HAH (Table 6).
Table 6.
Univariate and adjusted logistic regression for variables at baseline to predict HAH. (N = 129)
| Predictors | β-coefficient | Odds ratio | (95% CI) | P value | ||
|---|---|---|---|---|---|---|
| Lower | Upper | |||||
| Univariate logistic regression | ||||||
| CO | 0.650 | 1.915 | 1.158 | 3.168 | 0.011* | |
| Left side VA | Vm | 0.095 | 1.099 | 1.008 | 1.198 | 0.031* |
| Right side MCA | Vm | 0.071 | 1.073 | 1.021 | 1.127 | 0.005** |
| Vs | 0.039 | 1.040 | 1.005 | 1.076 | 0.026* | |
| Vd | 0.087 | 1.091 | 1.024 | 1.161 | 0.007** | |
| Right side VA | Vm | 0.099 | 1.104 | 1.007 | 1.211 | 0.035* |
| Adjusted logistic regression | ||||||
| Model 1 | ||||||
| Left VA | Vm | 0.094 | 1.099 | 1.007 | 1.199 | 0.035* |
| CO | 0.478 | 1.613 | 1.031 | 2.522 | 0.036* | |
| Model 2 | ||||||
| Right side MCA | Vm | 0.064 | 1.066 | 1.015 | 1.121 | 0.011* |
| CO | 0.594 | 1.811 | 1.080 | 3.036 | 0.024* | |
Model 1: Adjusted by primary variables (Vs and Vd of right side MCA)
Model 2: Adjusted by calculated variable (Vm of right side MCA)
Baseline CO was an independent predictor for HAH at 3700 m, whereas, Vm in left VA or right MCA was also independent predictors for HAH in different models
Only the variable with a significant statistically has been listed above
* p is 0.05 or less, ** p is 0.01 or less
Furthermore, in the subgroup analysis, the change in tricuspid regurgitation from sea level to 3700 m was significantly different between the HAH+ and HAH- groups. The alterations of ΔV in Vd and Vs of the VAs and the Vm and Vd of the BA were also significantly different between the HAH+ and HAH- groups (see Additional file 1: Table S1A).
Discussion
Alterations in both systemic and cerebral hemodynamics
In the current study, we identified alterations in both systemic and cerebral hemodynamics. The HR dramatically increased between sea level and high altitudes, which is consistent with a previous study that reported a significant increase in HR after exposure to high altitude because of the activation of the parasympathetic nervous system by hypobaric hypoxic stress [15, 4, 16]. However, the SV was similar at both altitudes, which indicates the increased CO was primarily caused by the increased HR [16]. Conversely, the hypoxia also induced a reduction in the SpO2, which may result in a decrease in the delivery of oxygen and energy to organs and tissues. Furthermore, the diastolic function of the heart has been reported to decrease in high altitude environments, which may be because of the shortened cardiac diastolic phase caused by the increased HR [17, 16].
Following acute hypoxic stress, parasympathetic nervous system activation, combined with a disequilibrium in the synthesis and expression of certain vasoconstrictors and vasodilators, results in endothelial cell dysfunction (e.g., increased endothelin-1 expression vs. decreased nitric oxide level) [18, 19]. Therefore, the vasoconstriction of systemic and cerebral arteries exhibits a significant impact on the measured velocities of blood flow [20]. We demonstrated that most velocities in both the anterior and posterior cerebral circulations significantly increased. These results are similar to previous studies in which cerebral blood flow increased dramatically after high altitude exposure [21–23].
Associations between HAH occurrence and demographical data
As previously reported by our team and other researchers, HAH patients are typically older in age, which is consistent with the risk factors of primary headache at sea level and high altitude [8, 9]. Although a history of smoking and alcohol consumption did not exhibit associations with HAH, they were not precisely measured, which could be improved in future studies.
HAH is partially associated with systemic hemodynamics
HAH is a regional symptom that comprises the primary diagnostic criteria of acute mountain sickness, which is typically induced by a local and systematic factor [5, 24]. Therefore, systemic hemodynamics may be a cause of HAH because it functions to deliver blood to all organs, including the brain, which is an organ with considerably high metabolism and energy consumption. First, an increased HR exhibited a strongly positive correlation with HAH, which is consistent with the relationship between CO and HAH. The HAH patients were also characterized by increased HR and CO. Further analyses indicated that baseline CO and LV were correlated with HAH significantly. These results may be because of the nervous system changes that lead to alterations in systemic hemodynamics [19, 25, 16]. In addition, the SpO2 was inversely correlated with HAH; however, the SBP and DBP were not related to HAH, which was similar to previous studies [8, 15, 25]. A reduced SpO2 and increased HR are independent risk factors for HAH [8, 9]. These changes could result from sympathetic nervous system activation and a decreased partial pressure of oxygen, which results in a decrease in oxygen delivery to the brain, where oxygen consumption is increased during hypoxic stress [5, 9, 6]. The change in tricuspid regurgitation in HAH patients differed from the non-HAH subjects, which indicates alterations in cardiac function induced by hypoxia may be risk factors for HAH (see Additional file 1).
Cerebral hemodynamic characteristics of HAH
In the present study, we demonstrated that the velocities in both the BA and left VA in the posterior cerebral circulation were strongly associated with HAH, which is partly consistent with previous reports [26, 22, 27]. The HAH patients were characterized by an increased Vd but decreased RI and PI in the left VA. These findings imply that HAH is associated with higher blood flow but lower resistance and compliance. At the baseline, HAH+ patients were also featured with a higher Vm in VAs on both sides indicating that posterior circulation plays critical roles in HAH or it is a pathophysiological process of HAH. Furthermore, the HAH+ group also exhibited increased Vs and Vd in the BA, which supplies blood and oxygen to the cerebellum. These results are consistent with the clinical characteristics that HAH often presents (i.e., a pulsing headache), which may be caused by diastolic dysfunction in the arteries [5, 6]. The relationship between HAH and posterior, rather than anterior, cerebral circulation contributed to HAH occurrence.
Of note, velocities in right MCA at baseline in HAH+ group were differed significantly from those in HAH- group. In partial agreement with the results reported for acute mountain sickness, including HAH, we did not identify an association between HAH and anterior circulation as assessed by the velocities, PI and RI of the bilateral MCAs [28]. However, these results were inconsistent with the previously reported that acute mountain sickness related headache usually presents as frontal headache [5]. The inconsistence may be caused by the sample size in the subgroup of 129 participants.
Though the baseline conduction from systemic to cerebral blood flow, which was evaluated using the cerebrovascular conductance index, showed a significant difference between HAH+ and HAH- groups, it is not predictor for HAH. Furthermore, it was not associated with HAH at 3700 m, which indicates cerebral blood flow plays a primary role in HAH and has more critical importance than systemic hemodynamics.
Predictors and risk factors for HAH
After adjusted regression analyses at baseline, we identified that CO and Vm in left VA (or right MCA in different regressions) were independent predictors for HAH. However, the posterior and anterior circulations were not valuable in a same model.
Other adjusted analyses at 3700 m revealed that only HR (or CO) and ΔVd were independent risk factors for HAH, which is partly consistent with our and others’ previous studies. However, ΔVd was found to be a novel risk factor for HAH which may be caused by the hypoxia induced local expressions of vasoactive substances. Furthermore, the variation in VAs of Chinese Han in anatomy may also be a reason for our findings.
Relationship between HAH and VA asymmetry
We report a novel finding in that VA asymmetry was closely related to HAH. An asymmetry in the bilateral isonym VA exists under normal physiological conditions [21, 28, 29]. However, this physiological asymmetry could become a considerable or pathological irregularity because of its amplification by hypoxia-induced vasodilatation and an impaired auto-regulation of cerebral blood flow following acute high-altitude exposure [21].
Furthermore, HAH severity was closely associated with the VA asymmetry, which represents a characteristic that has not been previously reported. This finding may be associated with the region of blood flow and perfusion in the cortex and cerebellum. It may also be related to the clinical characteristics of the migraine pattern present in many HAH patients [5]. The variance between the isonym VAs may contribute to the development of HAH and requires further examination to identify its precise pathophysiological mechanisms.
HAH comprises multifactorial components [30, 12, 31, 14]. Therefore, the cerebral and systemic hemodynamic characteristics of HAH may be relevant to the disease development, as well as its pathophysiological processes and clinical manifestations.
Limitations
Our study was restricted to young Chinese men, which could potentially generate a bias regarding age or gender; thus, this issue should be addressed in future studies. Another limitation is that a key modulator of cerebral perfusion, partial pressure of carbon dioxide (PaCO2), was not measured in the present study. This modulator could be included in future mechanistic studies. Another limitation is that headache satisfied the diagnostic criteria of the International Classification of Headache Disorders basically. Although the descent was not performed immediately after the onset of the headache, cephalalgia almost resolved as time went on. Furthermore, the subjects were all newcomers from sea level, thus none of them with a history of HAH or acute mountain sickness history, which should be improved in future study.
Conclusions
HAH is characterized, in part, by increased systemic hemodynamics and posterior cerebral circulation as reflected by the velocities in the BA and left VA, as well as lower arterial resistance and compliance. Furthermore, baseline CO and Vm in left VA or right MCA at sea level are independent predictors for HAH, whilst bilateral VA asymmetry may contribute to the development of HAH at high-altitude.
Acknowledgements
This work was supported by the Ministry of Health of the P.R. China [Grant No. 201002012]. We would like to thank all individuals who participated in this study for their support. We are grateful to professor Xia Zhang, Mr. Can Chen, Mr. Bai-Da Xu and Miss Shuang-Fei Li for their helps. We also thank Mr. Ru-Fu Xu for his suggestions regarding the statistical analyses.
Abbreviations
- BA
Basilar artery
- CO
Cardiac output
- DBP
Diastolic blood pressure
- EF
Ejection fraction
- HAH
High-altitude headache
- HAH+
HAH positive or with HAH
- HAH-
HAH negative or without HAH
- HR
Heart rate
- LA
End-diastolic internal diameters of left atrium
- LV
End-diastolic internal diameters of left ventricle
- MCA
Middle cerebral artery
- PA
End-diastolic internal diameters of pulmonary artery
- PI
Pulsatility index
- RA
End-diastolic internal diameters of right atrium
- RI
Resistance index
- RV
End-diastolic internal diameters of right ventricle
- SBP
Systolic blood pressure
- SpO2
Saturation pulse oxygen
- SV
Stroke volume
- VA
Vertebral artery
- Vd
Diastolic velocity
- Vm
Mean velocity
- Vs
Systolic velocity
- ΔVd
Difference in diastolic velocity between bilateral isonym cerebral arteries
- ΔVm
Difference in mean velocity between bilateral isonym cerebral arteries
- ΔVs
Difference in systolic velocity between bilateral isonym cerebral arteries
Additional file
Associations between changes of hemodymics and HAH in the subgroup.
Footnotes
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
SZB and LH participated the design of this research. SZB also has drafted the manuscript and performed the statistical analysis. JJ, XHZ and JQ have reviewed and revised this manuscript critically for important intellectual content. JY, XHZ, JQ and SZB carried out the filling of case report form and the measurements of blood pressure, HR and SpO2. RSR and SYY carried out the echocardiography examinations. The transcranial Doppler examinations were performed by CFT and QNL. All authors read and approved the final manuscript.
Authors’ information
SZB, MD, Physician and instructor from Institute of Cardiovascular Diseases of PLA; Department of Cardiology, Xinqiao Hospital, Third Military Medical University. His research areas include cardiovascular diseases, acute mountain sickness and high altitude headache and he has published two articles in Journal of headache and pain and European journal of Applied Physiology [8, 28].
LH, PhD, MD, FACC; Professor and Director of Institute of Cardiovascular Diseases of PLA; Department of Cardiology, Xinqiao Hospital, Third Military Medical University. His interests focus on basic and clinical researches in cardiovascular diseases, acute mountain sickness and high altitude headache.
Contributor Information
Shi-Zhu Bian, Phone: +86-23-68755601, Email: bianshizhu@163.com.
Jun Jin, Email: jjxqyy@163.com.
Qian-Ning Li, Email: LLQQNN@hotmail.com.
Jie Yu, Email: simpls@163.com.
Cai-Fa Tang, Email: tangcaifaxinqiao@163.com.
Rong-Sheng Rao, Email: rrs5103@163.com.
Shi-Yong Yu, Email: doctoryushiyong@126.com.
Xiao-Hui Zhao, Email: zxhwn@tmmu.edu.cn.
Jun Qin, Email: qinjunxq@126.com.
Lan Huang, Email: huanglan260@126.com.
References
- 1.Serrano-Duenas M. High-altitude headache. Expert Rev Neurother. 2007;7:245–248. doi: 10.1586/14737175.7.3.245. [DOI] [PubMed] [Google Scholar]
- 2.Burtscher M. High altitude headache: epidemiology, pathophysiology, therapy and prophylaxis. Wien Klin Wochenschr. 1999;111:830–836. [PubMed] [Google Scholar]
- 3.Carod-Artal FJ, High-altitude headache and acute mountain sickness High-altitude headache and acute mountain sickness. Neurologia (Barcelona, Spain) 2014;29(9):533–540. doi: 10.1016/j.nrl.2012.04.015. [DOI] [PubMed] [Google Scholar]
- 4.Imray C, Wright A, Subudhi A, Roach R. Acute mountain sickness: pathophysiology, prevention, and treatment. Prog Cardiovasc Dis. 2010;52:467–484. doi: 10.1016/j.pcad.2010.02.003. [DOI] [PubMed] [Google Scholar]
- 5.Alizadeh R, Ziaee V, Aghsaeifard Z, Mehrabi F, Ahmadinejad T. Characteristics of headache at altitude among trekkers; a comparison between acute mountain sickness and Non-acute mountain sickness headache. Asian J Sports Med. 2012;3:126–130. doi: 10.5812/asjsm.34714. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Silber E, Sonnenberg P, Collier DJ, Pollard AJ, Murdoch DR, Goadsby PJ. Clinical features of headache at altitude a prospective study. NEUROLOGY. 2003;60:1167–1171. doi: 10.1212/01.WNL.0000055876.26737.B9. [DOI] [PubMed] [Google Scholar]
- 7.Lawley JS. Identifying the possible risk factors for high-altitude headache in mountaineers. Cephalalgia. 2011;31:1677–1678. doi: 10.1177/0333102411422385. [DOI] [PubMed] [Google Scholar]
- 8.Bian SZ, Zhang JH, Gao XB, Li M, Yu J, Liu X, et al. Risk factors for high-altitude headache upon acute high-altitude exposure at 3700 m in young Chinese men: a cohort study. J Headache Pain. 2013;14:35. doi: 10.1186/1129-2377-14-35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Burtscher M, Mairer K, Wille M, Broessner G. Risk factors for high-altitude headache in mountaineers. Cephalalgia. 2011;31:706–711. doi: 10.1177/0333102410394678. [DOI] [PubMed] [Google Scholar]
- 10.Harris NS, Wenzel RP, Thomas SH. High altitude headache: efficacy of acetaminophen vs. ibuprofen in a randomized, controlled trial. J Emerg Med. 2003;24:383–387. doi: 10.1016/S0736-4679(03)00034-9. [DOI] [PubMed] [Google Scholar]
- 11.Mampreso E, Maggioni F, Viaro F, Disco C, Zanchin G. Efficacy of oxygen inhalation in sumatriptan refractory "high altitude" cluster headache attacks. J Headache Pain. 2009;10:465–467. doi: 10.1007/s10194-009-0160-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Carod-Artal FJ. High-altitude headache and acute mountain sickness. Neurologia. 2012;29(9):533–540. doi: 10.1016/j.nrl.2012.04.015. [DOI] [PubMed] [Google Scholar]
- 13.Sanchez del Rio M, Moskowitz MA. High altitude headache. Lessons from headaches at sea level. Adv Exp Med Biol. 1999;474:145–153. doi: 10.1007/978-1-4615-4711-2_13. [DOI] [PubMed] [Google Scholar]
- 14.Serrano-Duenas M. High altitude headache. A prospective study of its clinical characteristics. Cephalalgia. 2005;25:1110–1116. doi: 10.1111/j.1468-2982.2005.00968.x. [DOI] [PubMed] [Google Scholar]
- 15.Huang H-H, Tseng C-Y, Fan J-S, Yen DH-T, Kao W-F, Chang S-C, et al. Alternations of heart rate variability at lower altitude in the predication of trekkers with acute mountain sickness at high altitude. Clin J Sport Med. 2010;20:58–63. doi: 10.1097/JSM.0b013e3181cae6ba. [DOI] [PubMed] [Google Scholar]
- 16.Naeije R. Physiological adaptation of the cardiovascular system to high altitude. Prog Cardiovasc Dis. 2010;52:456–466. doi: 10.1016/j.pcad.2010.03.004. [DOI] [PubMed] [Google Scholar]
- 17.Bartsch P, Swenson ER. Acute high-altitude illnesses. N Engl J Med. 2013;369:1666–1667. doi: 10.1056/NEJMc1309747. [DOI] [PubMed] [Google Scholar]
- 18.Bailey DM, Roukens R, Knauth M, Kallenberg K, Christ S, Mohr A, et al. Free radical-mediated damage to barrier function is not associated with altered brain morphology in high-altitude headache. J Cereb Blood Flow Metab. 2006;26:99–111. doi: 10.1038/sj.jcbfm.9600169. [DOI] [PubMed] [Google Scholar]
- 19.Boushel R, Calbet JA, Radegran G, Sondergaard H, Wagner PD, Saltin B. Parasympathetic neural activity accounts for the lowering of exercise heart rate at high altitude. Circulation. 2001;104:1785–1791. doi: 10.1161/hc4001.097040. [DOI] [PubMed] [Google Scholar]
- 20.Jansen GF, Krins A, Basnyat B. Cerebral vasomotor reactivity at high altitude in humans. J Appl Physiol (Bethesda, Md : 1985) . 1999;86:681–686. doi: 10.1152/jappl.1999.86.2.681. [DOI] [PubMed] [Google Scholar]
- 21.Ainslie PN, Subudhi AW. Cerebral blood flow at high altitude. High Alt Med Biol. 2014;15:133–140. doi: 10.1089/ham.2013.1138. [DOI] [PubMed] [Google Scholar]
- 22.Lucas SJE, Burgess KR, Thomas KN, Donnelly J, Peebles KC, Lucas RAI, et al. Alterations in cerebral blood flow and cerebrovascular reactivity during 14 days at 5050 m. J Physiol. 2011;589:741–753. doi: 10.1113/jphysiol.2010.192534. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Norcliffe LJ, Rivera-Ch M, Claydon VE, Moore JP, Leon-Velarde F, Appenzeller O, et al. Cerebrovascular responses to hypoxia and hypocapnia in high-altitude dwellers. J Physiol. 2005;566:287–294. doi: 10.1113/jphysiol.2005.086629. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Willie CK, Smith KJ, Day TA, Ray LA, Lewis NCS, Bakker A, et al. Regional cerebral blood flow in humans at high altitude: gradual ascent and 2 wk at 5,050 m. J Appl Physiol (Bethesda, Md : 1985) 2014;116:905–910. doi: 10.1152/japplphysiol.00594.2013. [DOI] [PubMed] [Google Scholar]
- 25.Koehle MS, Guenette JA, Warburton DER. Oximetry, heart rate variability, and the diagnosis of mild-to-moderate acute mountain sickness. Eur J Emerg Med: official journal of the European Society for Emergency Medicine. 2010;17:119–122. doi: 10.1097/MEJ.0b013e32832fa099. [DOI] [PubMed] [Google Scholar]
- 26.Baumgartner RW, Spyridopoulos I, Bartsch P, Maggiorini M, Oelz O. Acute mountain sickness is not related to cerebral blood flow: a decompression chamber study. J Appl Physiol (1985) 1999;86:1578–1582. doi: 10.1152/jappl.1999.86.5.1578. [DOI] [PubMed] [Google Scholar]
- 27.Birmingham Medical Research Expeditionary S, Caudwell Xtreme Everest Research G. Wilson MH, Davagnanam I, Holland G, Dattani RS, Tamm A, Hirani SP, Kolfschoten N, Strycharczuk L, Green C, Thornton JS, Wright A, Edsell M, Kitchen ND, Sharp DJ, Ham TE, Murray A, Holloway CJ, Clarke K, Grocott MPW, Montgomery H, Imray C, Ahuja V, Aref-Adib G, Burnham R, Chisholm A, Clarke K, Coates D, Coates M, et al. Cerebral venous system and anatomical predisposition to high-altitude headache. Ann Neurol. 2013;73:381–389. doi: 10.1002/ana.23796. [DOI] [PubMed] [Google Scholar]
- 28.Bian SZ, Jin J, Li QN, Qin J, Zhang JH, Yu SY, Chen JF, Tang CF, Huang L. Cerebral hemodynamic characteristics of acute mountain sickness upon acute high-altitude exposure at 3,700 m in young Chinese men. European journal of applied physiology. 2014;114(10):2193–2200. doi: 10.1007/s00421-014-2934-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Wolff CB. Cerebral blood flow and oxygen delivery at high altitude. High Alt Med Biol. 2000;1:33–38. doi: 10.1089/152702900320667. [DOI] [PubMed] [Google Scholar]
- 30.Batsis JA, Phy MP. Intracranial hypotension: aggravation of headache at high altitude. Headache. 2005;45:380–384. doi: 10.1111/j.1526-4610.2005.05077_2.x. [DOI] [PubMed] [Google Scholar]
- 31.Miller JA, Gray J. Migraines and high-altitude headaches. Wilderness Environ Med. 2003;14:286–287. doi: 10.1580/1080-6032(2003)14[286:LTTE]2.0.CO;2. [DOI] [PubMed] [Google Scholar]