

A 47-year-old Caucasian man with a 2-year history of type 1 autoimmune pancreatitis (AIP) was referred to the nephrology clinic because of abnormal kidney imaging. He was asymptomatic and his physical examination was normal. Blood tests gave the following results: γ-glutamyltransferase (γ-GT): 662 IU/L (normal 8–16), alanine aminotransferase: 312 IU/L (normal <45), total bilirubin: 2.0 mg/dL (normal <1.2), lipase: 245 IU/L (normal <75), CA19–9: 100 U/mL (normal <37), IgG4: 310 mg/dL (normal 14–126) and serum creatinine (Scr): 0.8 mg/dL (normal 0.7–1.2). Urine analyses (dipstick, microscopy and 24-h urine collection) did not show any abnormality. Kidney ultrasound examination was normal. Besides a relapse of AIP, magnetic resonance imaging (MRI) and diffusion-weighted (DW) MRI sections showed bilateral cortical lesions in both kidneys (Figure 1a–e), corresponding to areas of restricted water diffusion. Biopsy of the left kidney, as classically advised, demonstrated normal parenchyma. The immunofluorescence study and IgG4 staining were negative (Figure 1f). Corticosteroids were started to treat relapsing AIP. During the follow-up, 1 year later, the patient remained asymptomatic. Biological parameters were normalized, except γ-GT and IgG4 serum levels (202 IU/L and 230 mg/dL, respectively). Renal function remained normal (SCr: 0.9 mg/dL). However, a control DW-MRI did not only show signs of AIP, but also enhanced renal lesions (Figure 2a–c). A second kidney biopsy targeting the bright areas well described by DW-MRI (Figure 2b) was performed on the antero-inferior pole of the right kidney. Light microscopy revealed marked tubular destruction and interstitial inflammation (lymphocytes, eosinophils and IgG4+ plasma cells), consistent with acute IgG4-related tubulointerstitial nephritis (TIN) (Figure 2d). Consequently, corticosteroids were increased to better control the involvement of both organs.
Fig. 1.
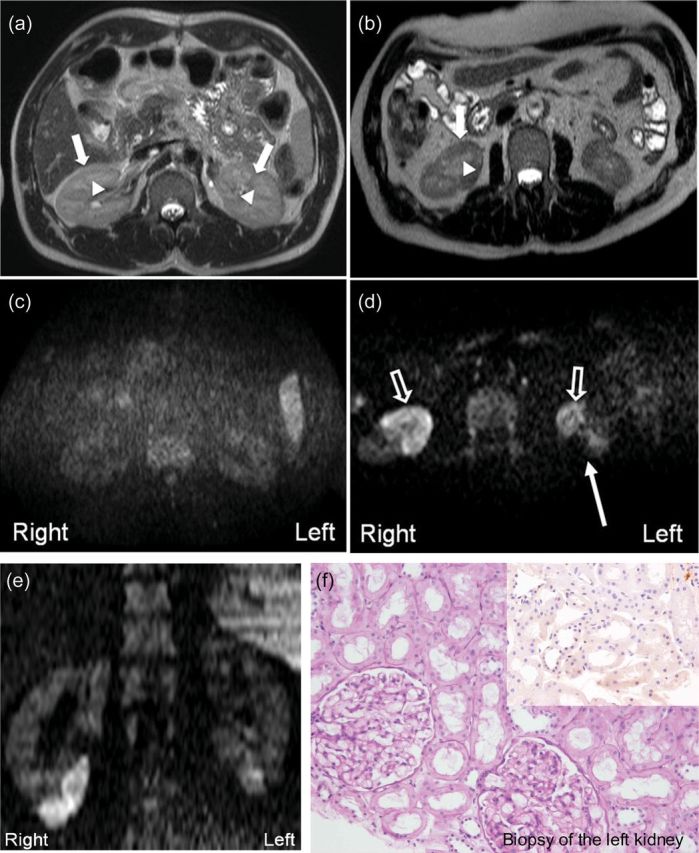
T2-weighted magnetic resonance imaging: (a) Normal kidneys showing the well-delineated renal cortex (closed arrows) from medulla (arrow head). (b) Kidneys during IgG-related TIN characterized by cortical thickening in the anterior and the inferior poles (closed arrows) and unchanged medulla (arrow head). Diffusion-weighted magnetic resonance imaging: (c) No bright areas indicating water movement restriction in normal kidneys. (d) Bright areas of water movement restriction (open arrows) related to increased cellularity in both kidneys in IgG-related TIN. The long arrow indicates ultrasound-guided biopsy of the left kidney. (d and e) Axial and coronal diffusion-weighted imaging sections demonstrated bright areas of water movement restriction related to increased cellularity of renal parenchyma in lower pole of both kidneys. (f) Histologically normal renal parenchyma and negative IgG4 immunohistochemistry (hematoxylin–eosin and IgG4 immunoperoxidase stainings. Original magnifications ×400).
Fig. 2.
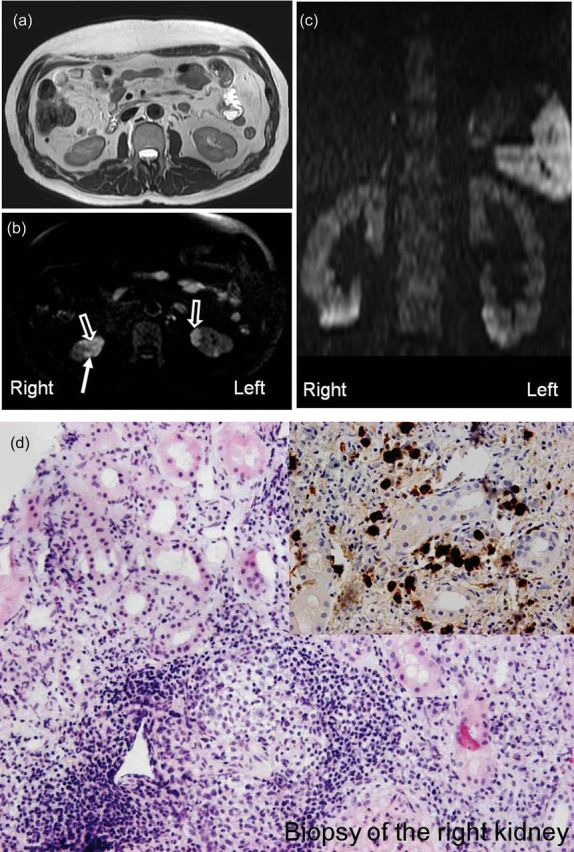
Magnetic resonance imaging performed 1 year later. (a) T2-weighted and (b) diffusion-weighted sections demonstrating slight increased renal lesions (open arrows). (c) Coronal reformat of diffusion-weighted magnetic resonance imaging displays the localization of affected (bright) and spared (dark) areas of both kidneys. These bright, multiple, bilateral areas of water movement restriction were related to hypercellular content of the renal tissue associated with marked thickening of the anterior cortex. The long arrow indicates ultrasound-guided biopsy of the right kidney. (d). Massive interstitial infiltration by plasma cells, lymphocytes and eosinophils with extensive tubular destruction and normal glomeruli. Marked (>30 IgG4+ cells/400× field) increase in IgG4+ plasma cells interstitial infiltration. (hematoxylin–eosin and IgG4 immunoperoxidase stainings. Original magnifications ×400).
IgG4-related TIN is a part of IgG4-related disease [1]. Recognition of this specific type of autoimmune TIN is mandatory to start appropriate therapy early and to prevent any further degradation of renal function [2]. Our observation demonstrates that DW-MRI can be useful in detecting subclinical (inflammatory) stage of IgG4-related TIN.
References
- 1.Cornell LD. IgG4-related kidney disease. Curr Opin Nephrol Hypertens. 2012;3:279–288. doi: 10.1097/MNH.0b013e32835265ac. [DOI] [PubMed] [Google Scholar]
- 2.Stone JH, Zen Y, Deshpande V. IgG4-related disease. N Engl J Med. 2012;366:539–551. doi: 10.1056/NEJMra1104650. [DOI] [PubMed] [Google Scholar]