

Abstract
Background:
Dental anxiety and fear are major complications for both patient and dental care provider. The purpose of this study was to assess the prevalence of dental anxiety and fear in patients who referred to Isfahan Dental School and their relation to their age, gender, educational level, past traumatic experiences and frequency of dental visits.
Materials and Methods:
In this cross-sectional study, 473 patients were provided with a questionnaire including three sections. First section contained questions concerning their age, gender, educational level, frequency of dental visits, reasons for irregular attendance and existence of past traumatic experiences. Second section comprised a Farsi version of Modified Dental Anxiety Scale (MDAS); and third included a Farsi version of dental fear survey (DFS). Data were analyzed by t-test, ANOVA, Pearson and Spearman correlation tests.
Results:
The prevalence of dental anxiety among the study population was 58.8%. No correlation was found between age and MDAS (r = −0.08, P = 0.07) and DFS (r = −0.03, P = 0.53). Women demonstrated higher anxiety (P < 0.001) and fear (P = 0.003). Education had no significant effect on dental anxiety (r = −0.046, P = 0.32) and dental fear (r = −0.017, P = 0.79). Previous traumatic experiences were found to result in elevated anxiety and fear (P < 0.001). There was an inverse relationship between frequency of dental attendance and anxiety (r = −0.128, P = 0.008).
Conclusions:
Within the limitations of this study, anxiety associated with dental treatment was widespread in the study population. Dental fear and anxiety were not affected by age or education level. Dental fear and anxiety were higher in women. In addition, people who visited the dentist more regularly and individuals without previous traumatic dental experiences were less anxious.
Keywords: Dental anxiety, dental fear, dental treatment, prevalence, sociodemographic data
INTRODUCTION
Fear is usually defined as an individual's response to an actual threatening event or a dangerous situation to protect one's life.[1] An existing specific stimulus like injection or drilling can provoke dental fear.[2] Dental anxiety refers to patient's specific reaction toward stress associated with dental treatment in which the stimulus is unknown, vague or not present at the moment.[2,3] Regardless, in both these situations the patient's emotional reactions could be practically similar.[4]
Dental anxiety is a major complication for both patient and dentist.[5] This apprehension leads patients to postpone or cancel dental visits or avoid treatment entirely.[5,6] It is confirmed that anxious patients have more decayed, missing and less filled teeth in comparison to nonanxious patients.[7] Their poorer oral health status can have negative effect on their social life.[8,9] Furthermore, treating anxious patients might take more time; it is hard to manage them during the procedure and they are often unsatisfied with their treatment.[5] Anxiety can effect patient/dentist relationship and result in misdiagnosis.[10] Dentists claim that such patients are important sources of stress that can compromise their practice.[11]
Dental anxiety is prevalent worldwide and not limited to a population or country.[12] Depending on the population and the measurement technique, 2.5-20% people endure high dental anxiety.[13,14] It is evaluated that 80% Americans have some anxiety regarding dental treatment and 5-14% them feel intense dental anxiety.[15] Many studies ascertain that dental anxiety is more common in women.[1,3,6,15] In addition, it has reported that anxiety subsides with age.[16] Some studies claim that patients with higher education experience less anxiety during dental procedures.[3,16] A study indicated that previous traumatic experience is a significant commencing factor in dental anxiety and fear.[16]
Dentists do not usually screen dental fear. A study in England showed that only 20% of dentists who were interested in treating patients with dental fear, had used a screening method to evaluate their patients’ level of fear.[17]
Prior to treatment, dentists should be able to detect patient's level of anxiety and fear so they can use appropriate management options.[4] Thus, several scales have been developed for this intention. Dental fear survey (DFS) for example, is a questionnaire that contains many questions and is proper for research purposes rather than clinical screening.[18,19] Another scale is Corah's Dental Anxiety Scale (CDAS).[20] This scale does not contain any questions about local anesthetic injection, which is a major anxiety source for some patients.[21] Modified Dental Anxiety Scale (MDAS), is established by Humphris et al.[22] based on the CDAS and comprises a question about local anesthetic injection. MDAS is the most accepted questionnaire for assessing dental anxiety in the UK.[23] It is valid, reliable and has good psychometric properties. Answering is easy, quick, not anxiety provoking and therefore suitable for clinical uses.[24,25,26] In younger children vocabulary, understanding and emotions are not fully developed so using DFS and MDAS are limited to adults.[27]
The purpose of this study was to evaluate the dental anxiety and fear in patients and their relation to age, gender, educational level, past traumatic experiences, and frequency of dental visits.
MATERIALS AND METHODS
This cross-sectional study was conducted in Dental School of Isfahan University of Medical Sciences. Samples were made up from 473 patients who were attending dental school clinic during 9 months of study period. After checking in, each patient was provided with a survey form and was asked to answer the questions. All the participants were informed about the confidentiality of their answers. Inclusion criteria were age of 18 and above and agreement to participate in the study. Exclusion criteria were intellectual disability and not having completed the survey form.
The measuring method was a survey form including three sections. First section contained questions concerning sociodemographic information (age, gender, and educational level) and data about frequency of dental visits (every 6 months, every year, sometimes, when there is an emergency), reasons for irregular attendance (high costs, lacking of time, not needing treatment, fear) and existence of past traumatic experiences. Second section was a Farsi version of MDAS. This scale includes 5 brief multiple choice questions and concerns patients’ anxiety in the fallowing situations:
Anticipating a visit to dental clinic,
Waiting in the dentist's office for treatment,
Waiting in the dental chair for drilling of teeth,
Waiting in the dental chair for scaling the teeth, and
Waiting in the dental chair for receiving a local anesthetic injection.
Possible answers could range from “nonanxious” with a value of 1, to “extremely anxious” with a value of 5. Summation of values for all answers assembles a score for level of dental anxiety with a minimum of 5 and maximum of 25. Patients with scores of 11 or more are considered dentally anxious. Scores from 11 to 14 reflect moderate anxiety; and scores from 15 to 19 show high anxiety. In this scale, high levels dental anxiety that may need special attention, is designated with an experimentally established cut-off value of 19 and above.[17]
Third section was a Farsi version of DFS questionnaire. This scale includes 20 questions in three components:
Avoidance of dental treatment,
Physiologic reactions to the dental treatment,
Fear aroused by different dental procedures.
Each question is provided with 5 possible answers ranging from 1 to 5.[18] Scoring 3 or more for each question indicates patient's fear and scoring 1 or 2 for a question expresses that patient isn’t fearful in the particular situation. Summation of answers constructed a score for level of dental fear that ranges from 20 to 100.
The survey form was designed based on literature,[3,5] with the counseling of professors of endodontic department and a psychiatrist. The MDAS and DAS questionnaires were first translated into Persian and then re-translated back to English by a psychiatrist, which established their reversibility.
A group of psychiatrists and professors of endodontic department evaluated content validity of the two questionnaires. Validity and reliability of English versions of MDAS and DFS are proven to be good in many studies.[18,24,28] Moreover, a pilot study was conducted to evaluate validity and test-retest reliability of Farsi versions of MDAS and DFS (Cronbach's α = 0.8). Data were analyzed using SPSS software, version 15 (SPSS Inc, Chicago, IL) by means of statistical analyzes t-test, ANOVA, Pearson and Spearman correlation tests. Statistical significance was defined at P < 0.05.
RESULTS
The sample consisted of 158 males (33.4%) and 315 females (66.6%) with a mean age of 32.5 ± 11 years for both sexes. The majority of the subjects (38.3%) were 26-35 years old. The proportion of regular attendee (16.5%) was less than irregular attendee (83.5%) [Figure 1]. The major reason given by 50.5% of the subjects for not attending the dentist regularly was “cost” while 25.7% thought that “treatment was not needed.” Only minority of the subjects delayed or avoided treatment because of “lack of time” (15%) or “fear” (8%).
Figure 1.
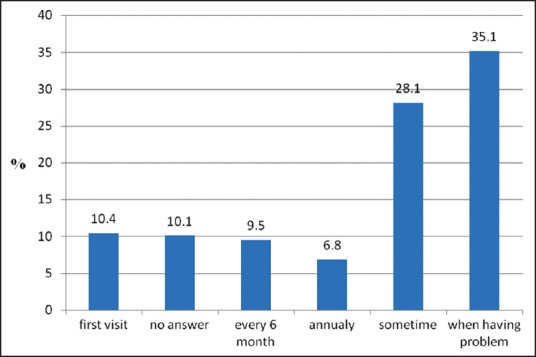
Frequency of dental visit.
The prevalence of dental anxiety among the study population was 58.8%. Based on severity of dental anxiety, 27.2%, 19.1% and 12.5% were found to be moderately, highly and extremely anxious, respectively.
The general question of DFS (how fearful are you of having dental work?) showed that about 39.6% the subjects reported some fear. Of these, 10.8% had a high dental phobia compared to 28.8% being slightly to moderately fearful of dental treatment.
The individual item frequencies of MDAS showed that the majority of men were “slightly anxious” with all items in the questionnaire except for sitting in the waiting room that most of them were “relax” [Table 1]. The majority of women were “slightly anxious” with all items in the questionnaire with exception of visiting the dentist tomorrow that they were “fairly anxious” [Table 1].
Table 1.
Item frequency breakdown of MDAS across men and women (number [%])

The total of MDAS and DFS scores were 12.34 ± 4.74 and 41.16 ± 15.96, respectively. Women demonstrated significantly higher MDAS scores (P < 0.001) and DFS scores (P = 0.003) than men [Table 2]. No correlation was found between age and MDAS (r = −0.08, P = 0.07) and DFS (r = −0.03, P = 0.53) [Table 2]. The results showed that education had no significant effect on dental anxiety (r = −0.046, P = 0.32) and dental fear (r = −0.017, P = 0.79) [Table 2]. Independent t-test demonstrates that MDAS scores in patients with previous traumatic experiences (13.9 ± 4.9) were significantly (P < 0.001) higher than the patients without bad experiences (11.5 ± 4.3). Furthermore, DFS scores in patients with previous traumatic experiences were (47.4 ± 17.03) and in patients without bad experiences were (37.9 ± 13.7). This difference was statistically significant (P < 0.001).
Table 2.
Mean and standard deviation of MDAS and DFS scores breakdown across gender, age and educational levels
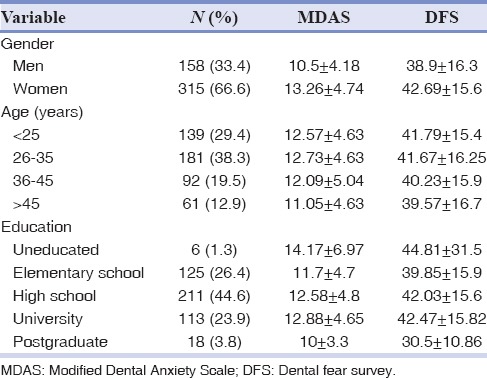
There was an inverse relationship between frequency of dental attendance and anxiety (r = −0.128, P = 0.008).
DISCUSSION
The prevalence of dental anxiety in the present study was found to be 58.8%, which suggests that despite the technological advances made in modern dentistry, anxiety associated with dental treatment was widespread in the study population. Prevalence was higher than that reported in studies done by Do Nascimento et al. (23%),[16] Malvania and Ajithkrishnan (46%).[29] However, it was less than the study conducted by Madfa et al. (63%).[30] This difference can be attributed partly to the methodological differences or geographical variation. Furthermore, overall level of fear of dental work among our population was similar to the Saudian population.[13]
About 16.5% of the subjects claimed to visit the dentist on regularity. This figure is low compared with the figures reported in the developed countries (50-72%).[31] The level of dental anxiety has been reported to effect dental attendance rate.[31] An inverse relationship between frequency of dental attendance and anxiety was evident in this study because regular attendee had less anxiety than irregular attendee. This finding was in agreement with two previous studies.[3,5]
The levels of anxiety shown during sitting in the waiting area and chair before having dental treatment demonstrate the need for well-trained supporting staff to be aware of the anxious patients. However, memory of dental experiences is extremely powerful and painless dental experiences following bad experience may not overcome perceived dental anxiety in the short term.[5] In a study conducted by Do Nascimento et al.,[16] it was found that people with previous traumatic dental experiences showed higher levels of dental fear and anxiety. This finding is consistent with the results of the present study.
In previous studies, dental anxiety has been frequently reported to vary with sex, age, education and social class.[3] In this study, the relation between patients’ sociodemographic factors (including age, gender and education) and MDAS and DFS scores was surveyed. The results of the study showed no statistically significant difference in anxiety levels between the age groups. In previous reports which are in compatible with our results, Humphris et al.,[3] Do Nascimento et al.,[16] Stabholz and Peretz[32] reported that age was strongly associated with dental anxiety and younger subjects were more anxious than older ones. However, Kanegane et al.,[33] Erten et al.,[6] Malvania and Ajithkrishnan[29] and Arslan et al.[1] found similar results with our study. In their report, Kanegane et al.[33] explained their finding with the small number of patients over 50 years of age. Furthermore, the majority of subjects in the studies conducted by Arslan et al.[1] and Erten et al.[6] were young. For the present survey, the youngest age of patients was 18 with the average age being 32.5 ± 11. This, therefore, may be a reasonable explanation why anxiety levels for the age groups showed no difference.
In the literature, although Kanegane et al.[33] reported no relation between gender and dental anxiety, many authors have shown that dental anxiety is more common in women.[1,3,5,6,16,27,32] The result of our study is similar to the most recent reports that females demonstrate higher levels of dental anxiety than males. This difference may be explained by women being more able to express their feelings of fear. In addition, physiological conditions such as social phobia, panic, depression, stress, and fear are more common in females and dental anxiety may be associated with such emotions.[1]
Patients with higher educational levels may have better oral health or visit the dentist more regularly.[1] In studies conducted by Humphris et al.,[3] Erten et al.[6] and Do Nascimento et al.[16] it's found that higher education leads to a reduction in dental anxiety. However, in our study, differences in educational level did not influence the dental anxiety level as was the case in the studies of Arslan et al.[1] and Kanegane et al.[33]
The present cross-sectional study has been conducted on a limited population who referred to Isfahan dental school during the study period. These patients had lower economical and educational levels; therefor studies on larger populations are needed to reveal prevalence and enormity of dental fear and anxiety in the society. Also further studies with different designs should be accomplished to investigate different commencing factors of dental anxiety and fear.
CONCLUSIONS
In this study, it was observed that anxiety associated with dental treatment was widespread in the study population. Dental fear and anxiety were not affected by age or education level. Dental anxiety levels of females were higher than males. In addition, people who visit the dentist more regularly were less anxious and having previous traumatic dental experiences can cause more anxiety.
ACKNOWLEDGMENTS
This study was supported by Isfahan University of Medical Sciences Research Grant Number 293324.
Footnotes
Source of Support: Isfahan University of Medical Sciences (Grant # 293324).
Conflict of Interest: The authors of this manuscript declare that they have no conflicts of interest, real or perceived, financial or non-financial in this article.
REFERENCES
- 1.Arslan S, Erta E, Ülker M. The relationship between dental fear and sociodemographic variables. Erciyes Med J. 2011;33:295–300. [Google Scholar]
- 2.Jaakkola S, Rautava P, Alanen P, Aromaa M, Pienihäkkinen K, Räihä H, et al. Dental fear: One single clinical question for measurement. Open Dent J. 2009;3:161–6. doi: 10.2174/1874210600903010161. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Humphris GM, Dyer TA, Robinson PG. The modified dental anxiety scale: UK general public population norms in 2008 with further psychometrics and effects of age. BMC Oral Health. 2009;9:20. doi: 10.1186/1472-6831-9-20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Milgrom P, Weinstein P, Kleinknecht R, Getz T. Reston, VA: Reston Publishing Co; 1985. Treating Fearful Dental Patients: A Patient Management Handbook. [Google Scholar]
- 5.Quteish Taani DS. Dental anxiety and regularity of dental attendance in younger adults. J Oral Rehabil. 2002;29:604–8. doi: 10.1046/j.1365-2842.2002.00905.x. [DOI] [PubMed] [Google Scholar]
- 6.Erten H, Akarslan ZZ, Bodrumlu E. Dental fear and anxiety levels of patients attending a dental clinic. Quintessence Int. 2006;37:304–10. [PubMed] [Google Scholar]
- 7.Esa R, Savithri V, Humphris G, Freeman R. The relationship between dental anxiety and dental decay experience in antenatal mothers. Eur J Oral Sci. 2010;118:59–65. doi: 10.1111/j.1600-0722.2009.00701.x. [DOI] [PubMed] [Google Scholar]
- 8.Crofts-Barnes NP, Brough E, Wilson KE, Beddis AJ, Girdler NM. Anxiety and quality of life in phobic dental patients. J Dent Res. 2010;89:302–6. doi: 10.1177/0022034509360189. [DOI] [PubMed] [Google Scholar]
- 9.Walsh LJ. Anxiety prevention: Implementing the 4 S principle in conservative dentistry. Auxilliary. 2007;17:24–6. [Google Scholar]
- 10.Cohen LA, Snyder TL, LaBelle AD. Correlates of dental anxiety in a university population. J Public Health Dent. 1982;42:228–35. doi: 10.1111/j.1752-7325.1982.tb02639.x. [DOI] [PubMed] [Google Scholar]
- 11.Toet A, Smeets MA, van Dijk E, Dijkstra D, van den Reijen L. Effects of pleasant ambient fragrances on dental fear: Comparing apples and oranges. Chemosens Percept. 2010;3:182–9. doi: 10.1007/s12078-010-9078-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Chellappah NK, Vignehsa H, Milgrom P, Lam LG. Prevalence of dental anxiety and fear in children in Singapore. Community Dent Oral Epidemiol. 1990;18:269–71. doi: 10.1111/j.1600-0528.1990.tb00075.x. [DOI] [PubMed] [Google Scholar]
- 13.Quteish Taani DS. Dental fear among a young adult Saudian population. Int Dent J. 2001;51:62–6. doi: 10.1002/j.1875-595x.2001.tb00823.x. [DOI] [PubMed] [Google Scholar]
- 14.Vassend O. Anxiety, pain and discomfort associated with dental treatment. Behav Res Ther. 1993;31:659–66. doi: 10.1016/0005-7967(93)90119-f. [DOI] [PubMed] [Google Scholar]
- 15.Scott DS, Hirschman R. Psychological aspects of dental anxiety in adults. J Am Dent Assoc. 1982;104:27–31. doi: 10.14219/jada.archive.1982.0123. [DOI] [PubMed] [Google Scholar]
- 16.Do Nascimento DL, da Silva Araújo AC, Gusmão ES, Cimões R. Anxiety and fear of dental treatment among users of public health services. Oral Health Prev Dent. 2011;9:329–37. [PubMed] [Google Scholar]
- 17.Armfield JM. Australian population norms for the Index of Dental Anxiety and Fear (IDAF-4C) Aust Dent J. 2011;56:16–22. doi: 10.1111/j.1834-7819.2010.01279.x. [DOI] [PubMed] [Google Scholar]
- 18.Kleinknecht RA, Klepac RK, Alexander LD. Origins and characteristics of fear of dentistry. J Am Dent Assoc. 1973;86:842–8. doi: 10.14219/jada.archive.1973.0165. [DOI] [PubMed] [Google Scholar]
- 19.Newton JT, Buck DJ. Anxiety and pain measures in dentistry: A guide to their quality and application. J Am Dent Assoc. 2000;131:1449–57. doi: 10.14219/jada.archive.2000.0056. [DOI] [PubMed] [Google Scholar]
- 20.Kelly M, Steele JG, Nuttal N, Bradnock G, Morris J, Nunn J, et al. London: The Stationary Office; 2000. Adult dental health survey, Oral health in the United Kingdom 1998. [Google Scholar]
- 21.Lindsay SJ, Humphris G, Barnby GJ. Expectations and preferences for routine dentistry in anxious adult patients. Br Dent J. 1987;163:120–4. doi: 10.1038/sj.bdj.4806218. [DOI] [PubMed] [Google Scholar]
- 22.Humphris GM, Morrison T, Lindsay SJ. The modified dental anxiety scale: Validation and United Kingdom norms. Community Dent Health. 1995;12:143–50. [PubMed] [Google Scholar]
- 23.Dailey YM, Humphris GM, Lennon MA. The use of dental anxiety questionnaires: A survey of a group of UK dental practitioners. Br Dent J. 2001;190:450–3. doi: 10.1038/sj.bdj.4801000. [DOI] [PubMed] [Google Scholar]
- 24.Humphris GM, Freeman R, Campbell J, Tuutti H, D’Souza V. Further evidence for the reliability and validity of the Modified Dental Anxiety Scale. Int Dent J. 2000;50:367–70. doi: 10.1111/j.1875-595x.2000.tb00570.x. [DOI] [PubMed] [Google Scholar]
- 25.Humphris GM, Hull P. Do dental anxiety questionnaires raise anxiety in dentally anxious adult patients. A two-wave panel study? Prim Dent Care. 2007;14:7–11. doi: 10.1308/135576107779398165. [DOI] [PubMed] [Google Scholar]
- 26.Newton JT, Edwards JC. Psychometric properties of the modified dental anxiety scale: An independent replication. Community Dent Health. 2005;22:40–2. [PubMed] [Google Scholar]
- 27.Peretz B, Efrat J. Dental anxiety among young adolescent patients in Israel. Int J Paediatr Dent. 2000;10:126–32. doi: 10.1046/j.1365-263x.2000.00181.x. [DOI] [PubMed] [Google Scholar]
- 28.Ronis DL. Updating a measure of dental anxiety: Reliability, validity, and norms. J Dent Hyg. 1994;68:228–33. [PubMed] [Google Scholar]
- 29.Malvania EA, Ajithkrishnan CG. Prevalence and socio-demographic correlates of dental anxiety among a group of adult patients attending a dental institution in Vadodara city, Gujarat, India. Indian J Dent Res. 2011;22:179–80. doi: 10.4103/0970-9290.79989. [DOI] [PubMed] [Google Scholar]
- 30.Madfa AA, Amran AG, Al-Sanabani FA, Alhajj MN, Al-Qudaimi NH, AL-Malahy NA, et al. Prevalence of dental anxiety and fear among medical students at University of Thamar. Am J Health Res. 2015;3:5–9. [Google Scholar]
- 31.Woolgrove J, Cumberbatch G. Dental anxiety and regularity of dental attendance. J Dent. 1986;14:209–13. doi: 10.1016/0300-5712(86)90003-5. [DOI] [PubMed] [Google Scholar]
- 32.Stabholz A, Peretz B. Dental anxiety among patients prior to different dental treatments. Int Dent J. 1999;49:90–4. doi: 10.1111/j.1875-595x.1999.tb00514.x. [DOI] [PubMed] [Google Scholar]
- 33.Kanegane K, Penha SS, Munhoz CD, Rocha RG. Dental anxiety and salivary cortisol levels before urgent dental care. J Oral Sci. 2009;51:515–20. doi: 10.2334/josnusd.51.515. [DOI] [PubMed] [Google Scholar]