

Abstract
Background
HIV/AIDS epidemic is concentrated among injecting drug users in Iran. Like many other countries with HIV/AIDS concentrated epidemic, prisons are high risk areas for spreading HIV/AIDS. The aim of this paper was to study the trend of HIV/AIDS prevalence and related interventions administered in prisons of Iran during a 13 years period
Methods
This cross sectional study was conducted using the data collected from the sentinel sites in all prisons in the country and it also used the data about Harm Reduction interventions which has been implemented by Iran Prisons Organization. To evaluate the correlation between the prevalence and each of administered interventions in prisons the Correlation Coefficient Test was used for the second half of the mentioned time period
Results
The prevalence of HIV/AIDS in prisons had increased rapidly in the early stages of epidemic, so that in 2002 the prevalence raised to 3.83%. Followed by the expansion of Methadone Maintenance Therapy and development of Triangular Clinics, HIV/AIDS prevalence in prisons declined. There was a relationship between interventions and the prevalence of HIV/AIDS.
Conclusion
In regions and countries where the epidemic is highly prevalent among injecting drug users and prisoners, Methadone Maintenance Therapy and development of Triangular Clinics can be utilized to control HIV/AIDS epidemic quickly.
Keywords: Prison, HIV/AIDS, Harm reduction, Iran
Introduction
The HIV epidemic, directly and indirectly, puts a high burden on human societies which cannot be easily estimated due to its several complicated factors. With increasing the prevalence of HIV infection Gross domestic product (GDP) is reduced (1). HIV/AIDS is a serious health threat for prisoners in many countries and it causes major challenges for prison and public health authorities and national governments. Worldwide, the levels of HIV among prisoners tend to be much higher than in the population outside. Prisons are considered as an important source of transmission and spread of HIV and other blood-borne diseases (2). Over the past two decades several studies have demon strated the role of prisons in the spread of blood-borne infections such as HIV and viral hepatitis (3–8).
Globally, around 16 million people inject drugs form whom three million are living with HIV and based on available evidences the most important reason for the rapid spread of HIV in such places is the use of shared needles and syringes among injecting drug users (IDUs) (9).
The high risk behaviors in prisons which pave the way of HIV transmission are not just limited to shared needle injection; the prisons provide a ground for other high risk behaviors that may lead to blood-borne diseases. In numerous studies, some high risk behaviors during imprisonment have been reported to be very common. Some behaviors like homosexuality and tattooing are more common in prisons than normal societies yet, compared with using shared needles; they have received less attention (10).
The common response of policy makers in countries with HIV epidemic among IDUs is to concentrate on public training and raising awareness to prevent using illicit drugs and high risk sexual relationships. In addition to training, Harm Reductions is considered as a pragmatic approach to prevent HIV. Using these two approaches, i.e. training and raising awareness concurrent with Harm Reduction interventions, Iran has been able to make a good response against HIV in general population and especially in prisons (11). The current status of HIV/AIDS in Iran (based on the registered records of Islamic Republic of Iran from the beginning) can be demonstrated as follows: by the end of 2011, a total of 24,290 people infected with HIV/AIDS had been identified from which 93.5% were male and 6.5% were female. Among the total registered cases in the country since 1984, the share of common causes of HIV infection has been as follows: shared drug injection 69.6%, Sexual Transmission 10.5%, Mother-To-Child Transmission (MTCT) 1 percent, and Unknown 17.9% (12).
As it was noted, in the second half of 1990s some HIV infection epidemics in Iran’s prisons were reported and based on the reports by Ministry Of Health (MOH) and UNAIDS the HIV epidemic was expended in prisons in these years (13). Based on the available evidences, HIV/AIDS has become prevalent in prisons mostly through the use of shared needles in IDUs (14). It is estimated half of prisoners in Iran are imprisoned due to drug-related crimes (15). According to a study, about 11.6% of the prisoners in Iran are IDUs (16).
Harm Reduction is a health-centered approach which is the main key for controlling HIV among IDUs; it is aimed to reduce the harms of high risk behaviors like intravenous drug injection and to change these behaviors to less harmful methods and behaviors (17).
Harm Reduction programs are selected as the main strategy for controlling HIV in Iran’s prisons. The administration of Methadone Maintenance Therapy (MMT) and the establishment of Triangular Clinics are two main Harm Reduction activities that are convincingly administered in Iran’s prisons. Triangular clinics in prisons provide several services for prisoners including: counseling and training about HIV/AIDS and other STIs, Harm Reduction and MMT services, and treatment of STIs. Accordingly, administration of MMT and prisoner’s access to Triangular Clinic services had extended quickly with a high coverage during the period 1999 to 2011. These services are presented in order to reduce the spread of HIV and other blood-borne diseases in prisons. This study was carried out to examine the prevalence of HIV and its association with Harm Reduction interventions in Iran prisons during a 13- years period (1999–2011).
Materials & Methods
Assessing the milestones through the establishment of sentinel sites is one of the conventional methods for monitoring HIV/AIDS. The data collected from sentinel sites have a special value for observing and monitoring the trends. In Iran, Prison Organization together with MOH design and administer sentinel sites in prisons annually. The sentinel sites are chosen by technical committees whose members are from Prison Organization and MOH. Based on available statistics of Prison Organization the total number of prisons in Iran which changed from 227 in 2006 to 242 Prisons in 2011; the prisons and prisoners in each prison are selected randomly. Based on conditions it is tried to establish sentinel sites in all parts of the country and provinces and in all major prisons. Samples are selected randomly form all groups of prisoners. About 150 to 400 samples were randomly examined in each sentinel site. However, in small prisons and sometimes for other reasons the number of samples might become more or less than this number. Sometimes some small jails were merged together to form a sentinel site. Samples were randomly selected from the list of all prisoners in each ward or prison. The trained people selected the participants and filled up the questionnaires and took samples after counseling prisoners and taking their consent to enroll in the study. If a prisoner was reluctant, he was not enrolled and no samples were taken.
The main variables which were investigated included age, gender and the possible way of transmission. In all these sentinel studies, first the study objectives for described for the participants and after taking their informed consent, the samples were taken. The samples were anonymously sent to a laboratory for ELISA test and positive ELISA cases were then confirmed by Western Blot. After collecting data, the results collected from sentinel sites were sent to the Center for Disease Control of the MOH and Prison Organization. This study includes all the data collected from sentinel sites established in all prisons of Iran from 1999 to 2011.
In addition, the data about the major interventions conducted in this period of time including prisoners MMT and Triangular Clinics in prisons were collected in both absolute and cumulative forms. The collected data included the number of people under the coverage of MMT and the number of triangular clinics. Data and information regarding the expansion of MMT and Triangular Clinics in prisons were received from the Health Statistics and Information Management Department in Prison Organization.
To analyze the data, firstly the trend of HIV prevalence in prisons and also the trend of expanding the interventions were described. Then, the HIV prevalence and confidence interval of prevalence among Iran prisoners were calculated for each year. Variable transformation was used to describe the variables better and to depict a graph showing the logical relationship between the simultaneous decrease in prevalence of HIV and an increase in the trend of interventions. The logarithm of the number of established triangle clinics in prison and the number of prisons accessing MMT services were used to show the changes in variables. To evaluate the correlation between the prevalence and each of the administered interventions in prisons the Pearson Correlation Coefficient Test was used for the second half of the mentioned time period.
Results
Based on the conducted study, a number of 551 sentinel sites were established in Iran’s prisons during the 13 years and in this check points 212,475 prisoners were evaluated and tested. Table 1 presents the number of sentinel sites, the number of inmates who were tested, HIV prevalence, and the Confidence interval for HIV prevalence in prisons of Iran from 1999 to 2011.
Table 1.
HIV prevalence in prisons of Iran (1999–2011)
| Year | No. of sentinel site | No. Of person who were tested | Positive cases | HIV Prevalence (%) | 95 CI% for HIV prevalence |
|---|---|---|---|---|---|
| 1999 | 11 | 3,334 | 52 | 1.56 | 1.14 - 1.98 |
| 2000 | 17 | 5,239 | 95 | 1.81 | 1.45 - 2.17 |
| 2001 | 37 | 15,612 | 487 | 3.12 | 2.84 - 3.4 |
| 2002 | 43 | 18,715 | 717 | 3.83 | 3.56 - 4.1 |
| 2003 | 51 | 19,684 | 547 | 2.78 | 2.55 - 3.01 |
| 2004 | 51 | 20,379 | 622 | 3.05 | 2.81 - 3.29 |
| 2005 | 58 | 21,025 | 682 | 3.24 | 3 - 3.48 |
| 2006 | 57 | 20,896 | 592 | 2.83 | 2.61 - 3.05 |
| 2007 | 52 | 19,403 | 331 | 1.71 | 1.53-1.90 |
| 2008 | 46 | 18,863 | 379 | 2.01 | 1.82-2.22 |
| 2009 | 44 | 16,390 | 252 | 1.54 | 1.36-1.74 |
| 2010 | 41 | 16,466 | 225 | 1.37 | 1.20-156 |
| 2011 | 43 | 16,469 | 210 | 1.28 | 1.13-1.48 |
As shown in Table 1, the maximum prevalence happened in 2002 (3.83%) and the minimum prevalence in 2011 (1.28%). Data in Table 1 shows that the HIV prevalence in Iran had an increasing trend from 1999 to 2002, so that 3.83 percent of prisoners in Iran were HIV infected in 2002. The HIV prevalence remained stable from 2002 to 2005. With implementation of Harm Reduction and interventional programs, the prevalence of HIV in Iran’s prisons gradually decreased from 2005 to 2011, so that it reached the minimum level of 1.28% in 2011. Two most important and effective interventions that have been carried out are: 1- Initiation and expansion of MMT. The program only covered 100 people in 2002 while it covered 38,256 people in 2011; 2- Setting up Triangular Clinics in prisons: the Triangular Clinics were set up in only one prison in 2001 while they were set up in 125 prisons in 2011.
MMT is one of the main Harm Reduction activities in Iran’s prisons that have received a lot of investment and budget allocations. Based on the data collected from MMT Department in Health office of Prison Organization (Table 2), the coverage of MMT program in Iran’s prisons had an increasing trend from 2002 to 2011, so that MMT program has become accessible for all provinces in Iran since 2007. Based on the data presented in Table 2, MMT program was introduced only in one of the prisons in Iran in 2002 while five years later in 2007 the MMT interventional program was expanded to all provinces.
Table 2.
Expanding methadone maintenance therapy (MMT) in prisons of Iran, 1999-2011
| Year | No. of MMT prisons coverage | Cumulative frequency of provinces that provide MMT | Cumulative frequency of prisoners that receive MMT |
|---|---|---|---|
| 1999 | 0 | 0 | 0 |
| 2000 | 0 | 0 | 0 |
| 2001 | 0 | 0 | 0 |
| 2002 | 1 | 1 | 100 |
| 2003 | 3 | 3 | 300 |
| 2004 | 20 | 17 | 1400 |
| 2005 | 40 | 26 | 2800 |
| 2006 | 54 | 27 | 8040 |
| 2007 | 116 | 30 (all provinces) | 19539 |
| 2008 | 142 | 30 (all provinces) | 25407 |
| 2009 | 154 | 30 (all provinces) | 25000 |
| 2010 | 159 | 31 (all provinces) | 28826 |
| 2011 | 164 | 31 (all provinces) | 38256 |
Another important Harm Reduction activity for controlling HIV/AIDS was the introduction and expansion of Triangular Clinics. These clinics were introduced to Iran’s prisons in 1999; Triangular Clinics had been set up in all prisons in Iran by 2001 to provide main services including counseling and training, Harm Reduction, and HIV/STI related services. Table 3 shows the trend of developing and expanding Triangular Clinics in Iran’s prisons.
Table 3.
Number of prisons and provinces which established triangular clinics (VCT services)
| Year | Cumulative freq. of prisons which have Triangular Clinics | Cumulative freq. of provinces which have Triangular Clinics | Cumulative freq. of provinces which have Triangular Clinics (%) |
|---|---|---|---|
| 1999 | 0 | 0 | 0 |
| 2000 | 0 | 0 | 0 |
| 2001 | 1 | 1 | 3.3 |
| 2002 | 16 | 11 | 36.6 |
| 2003 | 28 | 20 | 66.6 |
| 2004 | 41 | 20 | 66.6 |
| 2005 | 51 | 28 | 93.3 |
| 2006 | 75 | 30 (All Provinces) | 100 |
| 2007 | 105 | 30 (All Provinces) | 100 |
| 2008 | 118 | 30 (All Provinces) | 100 |
| 2009 | 128 | 30 (All Provinces) | 100 |
| 2010 | 133 | 31 (All Provinces) | 100 |
| 2011 | 128 | 31(All Provinces) | 100 |
As shown in Table 3, the coverage of the Triangular Clinics services in all 30 provinces had reached 100 percent by 2006. Following the national territorial divisions, a new province (Alborz Province) was introduced; all large prisons in this new province have triangular clinics.
Based on the results of statistical tests, there is a significant correlation between increasing MMT centers in Iran’s prisons and reducing the HIV prevalence from 2002 [ρ = - 0.62 with P=0.001]. Besides, there is a significant correlation between increasing the number of Triangular Clinics providing VCT services and reducing the incidence of HIV in prison from 2002 [ρ = - 0.51 with P = 0.016].
Graph 1 shows the relationship between the decreasing trend of HIV prevalence and the administered interventions. As shown in the Fig. 1, with increasing the interventions — which reached the maximum in 2004 and 2005 — the trend of HIV prevalence started decreasing.
Fig. 1.
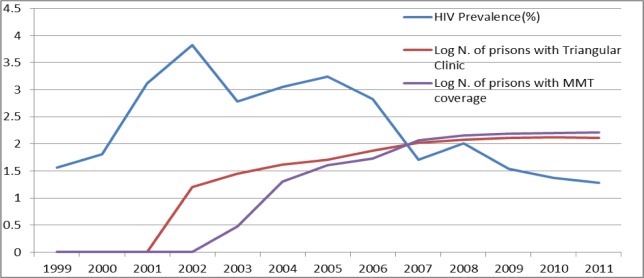
Trend of interventions and HIV prevalence in Iran’s prisons (1999–2011)
Discussion
Based on the results of current study the trend of HIV prevalence in Iran’s prisons from 1999 to 2000 can be described as follows. In the early years, i.e. 1999 to 2000, HIV had an increasing trend; it mostly remained stable from 2002 to 2005 and since 2005 it has started a decreasing trend. The main interventions including MMT and Triangular Clinics had been introduced and expanded since 2002, and since 2006 and 2007 these services have become available in most of prisons in Iran. The coverage of interventions has become stable since 2007 and it has been tried to increase the quality of services since then.
The increasing trend of HIV and the maximum level of HIV prevalence had happened in Iranian prisons during 2002 to 2005 when HIV was spreading in the country. During that time the prevalence of HIV in general populations was about 0.1% to 0.2%. In our study, the maximum prevalence was 3.83% in 2002 which was 19 times more than the prevalence in general population. Overall, the first cases of HIV/AIDS epidemics in Iran were started among IDUs in Iran’s prisons. As a result, the primary spread of the disease in prisons led to the spread of HIV/AIDS in Iran. The first alarms for the spread of HIV rose in prisons among IDUs, however the early responses were not up-to-date and satisfactory. In that time, based on MOH protocols HIV positive prisoners were quarantined. Due to this strategy and, also the lack of Harm Reduction programs in prisons, the increasing trend of HIV prevalence in Iran’s prisons which had started from the second half of 1990s lasted until the early years of 2000s; while HIV was spreading with an alarming speed, the interventional activities were adopted with a delay (18). After understanding the danger, the quarantining strategy was stopped also prisons started interventional activities, the rapid growth of HIV infection was dropped and from 2002 until 2005 the HIV prevalence was remained almost stable or had slight fluctuations. As it is obvious, because of the impacts of the increased coverage and the quality of Harm Reduction services the trend of HIV prevalence has started falling since 2005.
Analysis of the results of this study shows that the two main interventions (MMT and Triangular Clinics) in line with Harm Reduction services first dropped the increasing trend of HIV prevalence in Iran’s prisons and then have made it reversed. Although based on a comparison in 2008 the prevalence of HIV among Iran’s prisoners was eight times more than that among general population, it has decreased obviously compared with previous years. Concerning the epidemic stages of HIV/AIDS, we can say Iran is in Concentrated Epidemic stage, i.e. it is concentrated in IDUs as one of the high risk groups. Since many addicts often experience prison repeatedly, prisons are very high risk places. It is quite obvious that the high risk group of IDUs in Iran has had the biggest role in spreading HIV in the society and prisons. The estimations about the prevalence of drug abuse in Iran present significant numbers (16). However, the most important fact is that about half of Iran’s prison inmates are drug addicts from which 11.6% are IDUs (16). Additionally, it has been reported that the prevalence of using shared needles and syringes among IDUs prisoners is 47.3% (16).
One of the outcomes of this study is to present a 13-year trend of HIV epidemic in the prisons of Iran. There are few number of studies focusing on the prevalence of HIV in prisons in low and middle-income countries and most of effective and useful studies and researches are conducted in high income countries; the data in low and middle income countries are very limited and inadequate (19). Even in high income countries it is difficult to estimate the accurate number of HIV infected prisoners and the reported HIV prevalence are usually limited to only a prison or a region and cannot accurately reflect the prevalence of HIV in all prisons of a country (19). However, the data in the current study which is collected from annual data gatherings from sentinel sites in most of prisons in the country can demonstrate the real trend of HIV prevalence in Iran’s prisons.
Our result is in line with other finding in other countries which reported higher prevalence in prisons than in general populations. Nevertheless, re-viewing the prevalence of HIV in prisons around the world has shown that HIV infection is a serious issue that needs further actions (20). In terms of HIV prevalence among prisoners, in some cases our results shows higher prevalence of HIV in the country’s prisons than in the general population. In a study among 623 prisoners at one of the Belize Central Prisons, the HIV test positivity rate was 4% (21). HIV prevalence among prisoners in Austria was five times higher than the prevalence in the general population of the country (22). HIV prevalence among prisoners in America has been reported to be five times higher than the prevalence in the general population (23).
Overall, the reported prevalence rates in different prisons from different countries are diverse. In some prisons from different parts of the world, higher levels of HIV prevalence have been reported. Different studies have reported a various range of HIV prevalence in prisons on different countries: the HIV prevalence is reported zero among Scottish male inmates and Lowa prisoners (24), 33.6% among adult prisoners in Catalonia, Spain (25), and more than 50% among women in a correctional facility in New York (26).
World Health Organization has recommended a comprehensive package including nine interventions for IDUs for many countries especially low and middle income countries; in this package four important and effective activities that can effectively reduce HIV prevalence are (27):
Needle and syringe programs (NSP)/Medications-assisted Therapy (MAT)/Antiretroviral Therapy (ART) / HIV Counseling and testing (HCT) From the activities mentioned, NSP and MAT can decline injecting behavior. HCT or VCT reduce the risk of risky sexual behavior and ART can the risk of transmission through intravenous drug injection and also through sexual relationships. Iran has complied with these guidelines and provided a good coverage of these programs, particularly in prisons, and has been able to control HIV infection in prisons. In Spain, the impact of Harm Reduction programs, particularly NSP program, in reducing HIV infection in prisons has been proven (28). Previous studies in Iran indicate that Harm Reduction programs are successful (17).
Based on the results it can be concluded that setting up Triangular Clinics and Methadone Maintenance Therapy as the HIV/AIDS Control Strategies which are implemented in Iran’s prisons following the WHO recommendations are highly efficient and they not only controlled the prevalence of HIV but also has led to its decreasing trend in prisons. It is recommended to continue and enhance these services and try to increase the quality of services in Iran. In other countries that are facing concentrated epidemics among IDUs and have many addicts and especially IDUs in their prisons these experiences and strategies may be implemented to reduce and control HIV in prisons. It is recommended to conduct further studies to measure the quality of interventions. Additionally, since Harm Reduction programs cover a large group of people in Iran’s prisons, it may provide a good ground for studying positive outcomes as well as deficiencies and problems of Harm Reduction activities to be utilized in the prisons all around the world.
As one of the study limitations, the data used in this study was extracted from the data collected by HIV/AIDS Surveillance System over a period of 13 years. The data may not have the same quality over the mentioned period; since the data had not been intended for a research, it might have some biases. Another limitation is that its response rate is not clear and it is likely the people who rejected doing the test were those who were infected with HIV.
Conclusion
Intravenous drug injection can lead to the spread of HIV/AIDS in prisons and societies all over the world. In regions and countries where the epidemic is highly prevalent among IDUs and prisoners, MMT and development of Triangular Clinics can be utilized to control HIV/AIDS epidemic quickly.
Ethical considerations
Ethical issues (Including plagiarism, Informed Consent, misconduct, data fabrication and/or falsification, double publication and/or submission, re dundancy, etc) have been completely observed by the authors.
Acknowledgments
The researchers of this study would like to thank the following people for their help in collecting the data and conducting the sentinel site studies all over the years:
The managers and technician staffs in Prison Organization, The head of Communicable Center of Disease Control, the personnel of HIV/AIDS office in MOH, and Health deputies of universities of medical sciences in all over Iran. The authors declare that there is no conflict of interests.
References
- UNAIDS, (2010). UNAIDS report on the global AIDS epidemic. Available from:http://ww-w.unaids.org/globalrepor/documents/20101123_GlobalReport_full_en.pdf.
- UNODC, WHO, UNAIDS, (2006). HIV/AIDS Prevention, Care, Treatment and Support in Prison Settings, A Framework for an Effective National Response, UNODC Report, 2006.
- Diendéré EA, Tiéno H, Bognounou R, Ouédraogo DD, Simporé J, Ouédraogo-Traoré R, Drabo J (2011). Prevalence and risk factors associated with infection by human immune-deficiency virus, hepatitis B virus, syphilis and bacillary pulmonary tuberculosis in prisons in Burkina Faso. Med Trop, 71(5) pp.: 464–467. [PubMed] [Google Scholar]
- Peate I (2011). Prisoner health: HIV infection and other blood-borne viral infections. Br J Nurs, 20(10) pp.: 605–606, 608–610. [DOI] [PubMed] [Google Scholar]
- Nelles J, Fuhrer A, Hirsbrunner H P, Harding T W (1998). Provision of syringes: the cutting edge of Harm Reduction in prison? BMJ, 317 pp.: 270–273. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thaisri H, Lerwitworapong J, Vongsheree S, Sawanpanyalert P, Chadbanchachai C, Rojana-wiwat A, Kongpromsook W, Paungtubtim W, Sri-ngam P, Jaisue R (2003). HIV infection and risk factors among Bangkok prisoners, Thailand: a prospective cohort study. BMC Infect Dis, 3: 25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stark K, Herrmann U, Ehrhardt S, Bienzle U (2006). A syringe exchange programme in prison as prevention strategy against HIV infection and hepatitis B and C in Berlin, Germany. Epidemiol Infect, 134, pp.: 814–819. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Razani N, Mohraz M, Kheirandish P, Malekinejad M, Malekafzali H, Mokri A, McFarland W, Rutherford G (2007). HIV risk behavior among injection drug users in Tehran, Iran. Addiction, 102(9) pp.: 1472–1482 Epub 2007July23. [DOI] [PubMed] [Google Scholar]
- Pont J, Strutz H, Kahl W, Salzner G (1994). HIV epidemiology and risk behavior promoting HIV transmission in Austrian prisons. Eur J Epidemiol, 10(3) pp.: 285–289. [DOI] [PubMed] [Google Scholar]
- Rotily M, Weilandt C, Bird SM, Käll K, Van Haastrecht HJ, Iandolo E, Rousseau S (2001). Surveillance of HIV infection and related risk behaviour in European prisons. A multicentre pilot study. Eur J Public Health, 11(3) pp.: 243–250. [DOI] [PubMed] [Google Scholar]
- Moradi GH, Malekafzali H, Holakoeii Naieni K, Rashidian A, Vazirian P, Mirzazadeh A, Barati H (2011). HIV/AIDS Situation in Economic Cooperation Countries; Achievement and Gaps toward Millennium Development Goals. Journal of Family and Reproductive Health, 5(1): 1–9. [Google Scholar]
- Iran Ministry of health (2011). Center for disease control. Annual report of HIV in Iran. December of 2011.
- UNAIDS Website (2012). available at: www. UNAIDS.org\2012.
- Amin-Esmaeili M, Rahimi-Movaghar A, Haghdoost AA, Mohraz M (2012). Evidence of HIV epidemics among non-injecting drug users in Iran: a systematic review. Addiction, 107(11) pp.: 1929–1938. [DOI] [PubMed] [Google Scholar]
- Iran Prison Organization (2009). Report by Health and Treatment Headquarter of Iran Prison Organization, in August2009. [Google Scholar]
- Narenjiha H, Rafiei H, Baghestani AR, Noori R, Shirin Baian P, Vejdani A & et al. (2005). Report of rapid assessment drug abuse and drug dependency in Iran. Center for Education and Research of Olom Behzisti University. June2005.
- Eshrati B, Asl RT, Dell CA, Afshar P, Millson PM, Kamali M, Weekes J (2008). Preventing HIV transmission among Iranian prisoners: initial support for providing education on the benefits of Harm Reduction practices. Harm Reduct J, 9; 5 p.: 21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Health and Treatment Headquarter of Iran Prison Organization. (2006). an overview on HIV/AI-DS in prisons of Islamic Republic of Iran. Tehran: Iran Prison Organization. [Google Scholar]
- Dolan K, Kite B, Black E, Aceijas C, Stimson GV (2007). HIV in prison in low-income and middle-income countries. Lancet Infect Dis, 7(1) pp.: 32–41. [DOI] [PubMed] [Google Scholar]
- WHO/UNODC/UNAIDS(2007). Interventions to address HIV in prisons: Comprehensive review (Evidence for Action Technical Paper), Geneva: World Health Organization. [Google Scholar]
- Gough E, Edwards P (2009). HIV sero-prevalence and associated risk factors among male inmates at the Belize central prison. Rev Panama Salud Publica, 25(4) pp.: 292–299. [DOI] [PubMed] [Google Scholar]
- Hellard ME, Aitken CK (2004). HIV in prison: what are the risks and what can be done? Sex Health, 1(2) pp.: 107–113. [DOI] [PubMed] [Google Scholar]
- Jürgens R, Ball A, Verster A (2009). Interventions to reduce HIV transmission related to injecting drug use in prison. Lancet Infect Dis, 9: 57–66. [DOI] [PubMed] [Google Scholar]
- Jafa K, McElroy P, Fitzpatrick L, Borkowf CB, Macgowan R, Margolis A, Robbins K, Youngpairoj AS, Stratford D, Greenberg A, Taussig J, Shouse RL, Lamarre M, McLellan-Lemal E, Heneine W, Sullivan PS (2009). HIV transmission in a state prison system, 1988–2005 PLoS One, 4(5): e5416. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Martin V, Bayas IM, Laliga A (1990). Seroepidemiology of HIV-1 infection in a Catalonian penitentiary. AIDS, 4 pp.: 1023–1026. [DOI] [PubMed] [Google Scholar]
- Vlahov D, Brewer TF, Castro KG (1991): Prevalence of antibody to HIV-1 among entrants to US correctional facilities. J Am Med Ass, 265 pp.: 1129–1132. [PubMed] [Google Scholar]
- Dutta A, Wirtz AL, Baral S, Beyrer C, Cleghorn FR (2012). Key Harm Reduction interventions and their impact on the reduction of risky behavior and HIV incidence among people who inject drugs in low-income and middle-income countries. Curr Opin HIV AIDS, 7(4) pp.: 362–368. [DOI] [PubMed] [Google Scholar]
- Arroyo-Cobo JM (2010). Public health gains from health in prisons in Spain. Public Health, 124(11) pp.: 629–631. [DOI] [PubMed] [Google Scholar]