

Abstract
Accurately recognising a supraclinoid internal carotid artery (ICA) fenestration, despite its rare location, is important as it can mimic an intracranial aneurysm, intraluminal thrombus or focal dissection on non-invasive imaging. The overwhelming majority of reported supraclinoid ICA fenestrations are associated with intracranial aneurysms; however, a concomitant arteriovenous malformation (AVM) remote from the fenestration site should also be considered. We present the case of a 26-year-old woman with a Spetzler-Martin grade I right frontal AVM in whom a left supraclinoid ICA fenestration was incidentally discovered during cerebral angiography. She underwent n-N-Butyl Cyanoacrylate glue embolisation of two dominant middle cerebral artery feeders followed by neurosurgical resection. She tolerated procedures well without complications and has remained neurologically intact.
Background
Intracranial arterial fenestrations are most commonly located in the anterior communicating artery, followed by the vertebrobasilar, anterior cerebral and middle cerebral arteries.1 Rarely is a fenestration of the supraclinoid internal carotid artery (ICA) encountered and of the 18 reported in the literature, 15 are associated with intracranial aneurysms.2 This relationship is well described; however, the coexistence of an intracranial arteriovenous malformation (AVM) is less recognised and has not been reported in association with an ICA fenestration.3 We present this case to highlight the importance of accurately recognising an arterial fenestration in an uncommon location and to emphasise the possibility not only of an associated aneurysm, but also of a coexistent AVM, either of which may be in remote vascular territories.
Case presentation
A 26-year-old woman with a history of migraines and hypertension presented to the emergency room with an atypical headache. A non-contrast CT of the brain showed an area of calcification and focal encephalomalacia in the right frontal lobe. No acute haemorrhage was present. MRI of the brain with gadolinium was performed, which demonstrated a right frontal AVM. Cerebral DSA confirmed the AVM and incidentally discovered a left supraclinoid ICA fenestration.
The patient underwent n-N-Butyl Cyanoacrylate glue embolisation prior to surgical resection and tolerated both procedures well without complications. She had an uneventful postoperative course, was neurologically intact and was discharged to home on postoperative day 7.
Investigations
MRI of the brain with gadolinium demonstrated the right frontal AVM (figure 1); however, the MRA failed to clearly show the left supraclinoid ICA fenestration (figure 2).
Figure 1.
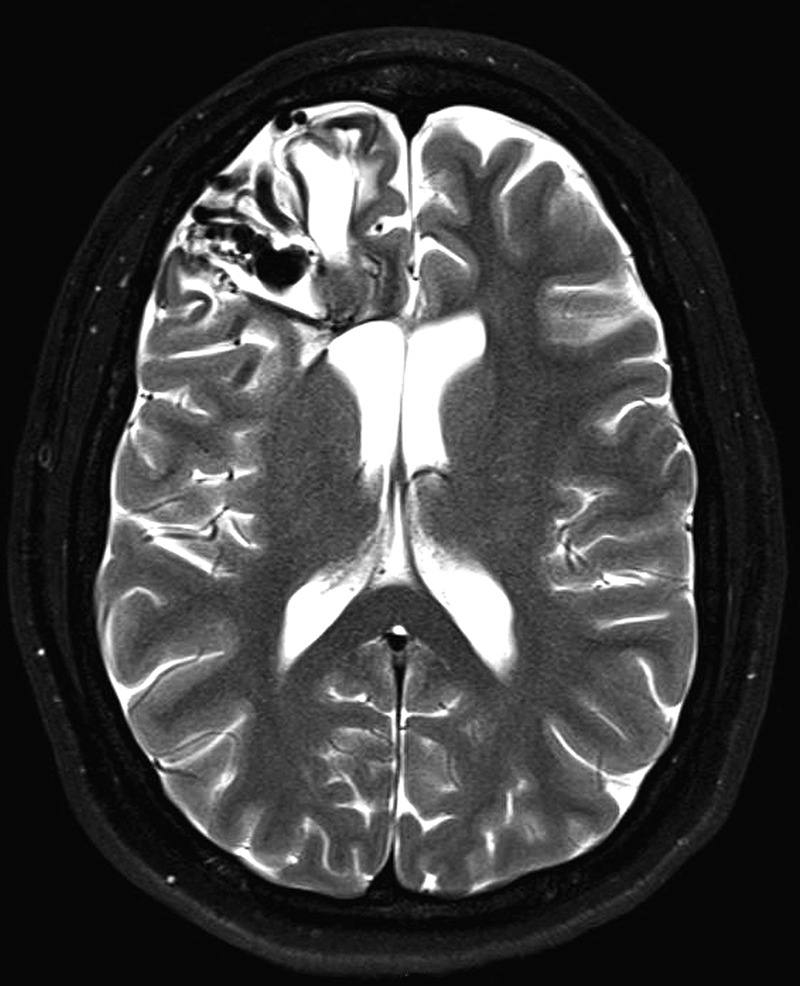
Axial T2-weighted MRI of the brain demonstrates prominent flow voids in the right frontal lobe with surrounding encephalomalacia and a hemosiderin rim, suggestive of prior haemorrhage.
Figure 2.
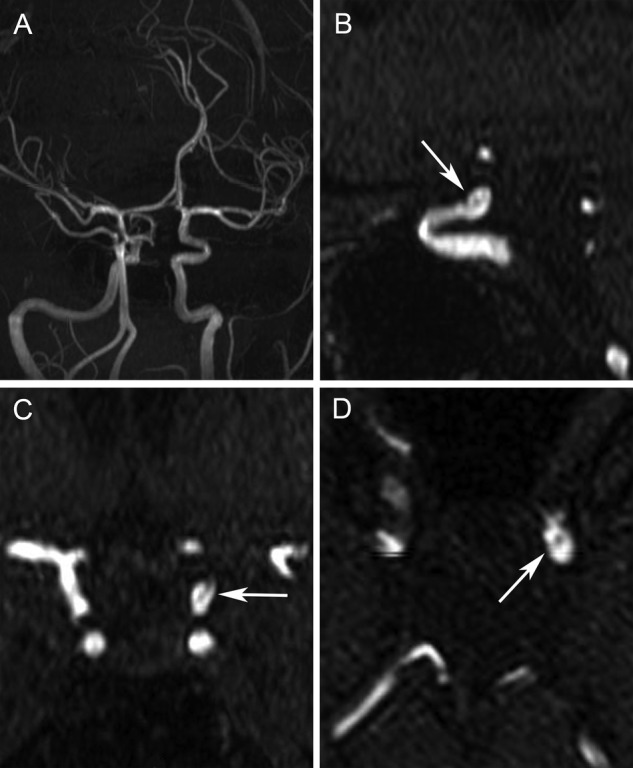
MR angiography (MRA) images of the brain. The left internal carotid artery fenestration is not seen on the oblique maximum intensity projection image (A). A faint intraluminal filling defect is seen on the sagittal (B), coronal (C) and axial (D) MRA images, which can be mistaken for an intraluminal clot or focal dissection.
Cerebral DSA demonstrated a Spetzler-Martin grade I right frontal AVM. Aneurysmally enlarged venous pouches were present, suggestive of direct high-flow arteriovenous shunts within the AVM (figure 3). A left ophthalmic segment fenestration (figure 4) was incidentally discovered.
Figure 3.
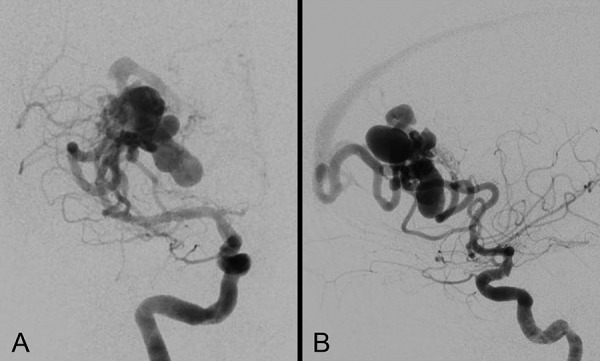
Cerebral DSA images of the right carotid. Posteroanterior and lateral views from a right carotid angiogram demonstrate a high-flow right frontal arteriovenous malformation fed predominantly by two hypertrophied prefrontal branches of the superior division of the right middle cerebral artery. Aneurysmally enlarged venous pouches are seen, suggestive of direct high-flow arteriovenous shunts.
Figure 4.
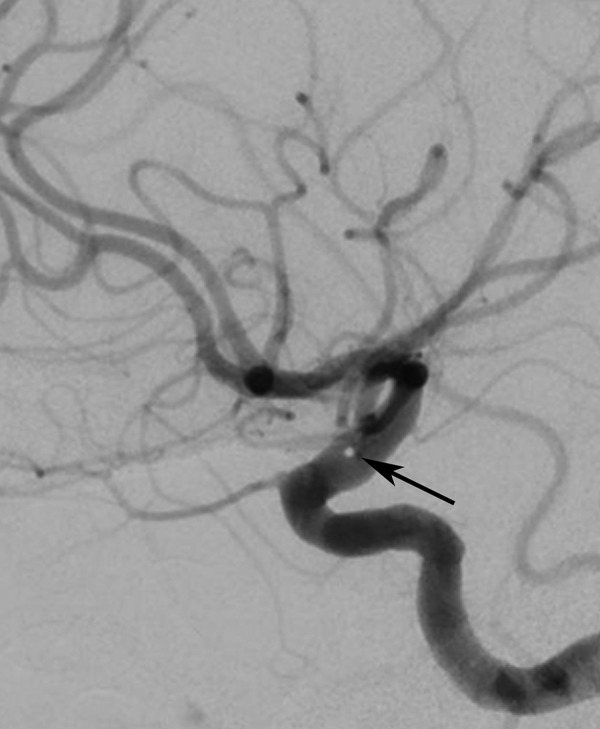
Lateral view from a left carotid angiogram shows the left ophthalmic segment fenestration (arrow) between the origins of the ophthalmic and posterior communicating arteries.
Discussion
Fenestration of an intracranial artery refers to division of an arterial lumen resulting in two distinct endothelium-lined channels, which may or may not share an adventitial layer. The appearance may vary from a small island of tissue separating the two channels to duplication of a long arterial segment.4
Intracranial fenestrations are most commonly located in the anterior communicating artery, followed by the vertebrobasilar, anterior cerebral and middle cerebral arteries.1 The supraclinoid ICA is a rare site with only 18 cases reported.2 5 Of these, 15 are associated with intracranial aneurysms, most commonly involving the fenestration itself (n=12); however, aneurysms may also exist remote to the fenestration.
The association of fenestrations with intracranial aneurysms has been well documented; however, few studies have considered the coexistence of fenestrations and AVMs. Teal et al6 was the first to describe this association and to date there are 22 reported cases, the largest single series by Yang et al.3 The most common fenestration site associated with an intracranial AVM is the vertebrobasilar system, followed by the anterior communicating region. No associated AVMs have been reported in conjunction with a supraclinoid ICA fenestration. All described fenestrations are remote to the AVMs, as in our case, which emphasises the need to interrogate all intracranial vascular territories when a vascular anomaly is encountered.
Intracranial fenestrations presumably result from the anomalous fusion or division of primitive vessels and mechanisms underlying their formation have been proposed for the basilar artery (incomplete fusion of parallel arterial segments), and distal vertebral artery (passage of a solid structure such as the hypoglossal nerve). The aetiology is less clear for a supraclinoid ICA fenestration. A proposed theory suggests this anomaly develops at the 4–5 mm embryonic stage, during which the primitive carotid artery divides to form the cranial and caudal divisions of the ICA.7 At this stage, the two intracranial carotid arteries temporarily connect through small plexiform channels and persistence of one of these channels may give rise to a fenestration at this site.8 This theory would explain the location (just distal to the ophthalmic artery) of all reported supraclinoid ICA fenestration cases.2
While the association of intracranial aneurysms at fenestration sites can be explained due to haemodynamic stresses akin to bifurcation sites, the aetiology of concomitant AVMs and fenestrations remains unclear. Some propose this association may exist because both entities are developmental anomalies of the persistent embryonic state.9
A supraclinoid ICA fenestration is important to recognise as it has diagnostic implications. Owing to of its rare location, a fenestration in this location may mimic an intraluminal thrombus,5 dissection or aneurysm10 on non-invasive imaging. They are also difficult to diagnose in the absence of a conventional angiogram, as evidenced by our case.
Learning points.
The supraclinoid internal carotid artery (ICA) is a rare location for an arterial fenestration and accurate recognition is important to distinguish it from an intracranial aneurysm, intraluminal thrombus, or focal dissection.
The majority of reported supraclinoid ICA fenestrations are associated with intracranial aneurysms; however, a concomitant arteriovenous malformation remote from the fenestration site should also be considered.
Footnotes
Competing interests: None declared.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Dey M, Awad IA. Fenestration of supraclinoid internal carotid artery and associated aneurysm: embryogenesis, recognition, and management. World Neurosurg 2011;76:592 e1–5. 10.1016/j.wneu.2011.04.019 [DOI] [PubMed] [Google Scholar]
- 2.Park SH, Lee CY. Supraclinoid internal carotid artery fenestration harboring an unruptured aneurysm and another remote ruptured aneurysm: case report and review of the literature. J Cerebrovasc Endovasc Neurosur 2012;14:295–9. 10.7461/jcen.2012.14.4.295 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Yang YJ, Gao LY, Guo X et al. Intracranial arterial fenestrations associated with arteriovenous malformations diagnosed by CT angiography. J Neuroimaging 2014;24:366–70. 10.1111/jon.12092 [DOI] [PubMed] [Google Scholar]
- 4.Sanders WP, Sorek PA, Mehta BA. Fenestration of intracranial arteries with special attention to associated aneurysms and other anomalies. AJNR Am J Neuroradiol 1993;14:675–80. [PMC free article] [PubMed] [Google Scholar]
- 5.Tourdias T, Berge J, Menegon P et al. Fenestration of the internal carotid artery mimicking floating thrombus on CT and MR angiography. Neurology 2011;76:1846 10.1212/WNL.0b013e31821ccd28 [DOI] [PubMed] [Google Scholar]
- 6.Teal JS, Rumbaugh CL, Bergeron RT et al. Angiographic demonstration of fenestrations of the intradural intracranial arteries. Radiology 1973;106:123–6. 10.1148/106.1.123 [DOI] [PubMed] [Google Scholar]
- 7.Lasjaunias P, Santoyo-Vazquez A. Segmental agenesis of the internal carotid artery: angiographic aspects with embryological discussion. Anatomia clinica 1984;6:133–41. 10.1007/BF01773165 [DOI] [PubMed] [Google Scholar]
- 8.Banach MJ, Flamm ES. Supraclinoid internal carotid artery fenestration with an associated aneurysm. Case report J Neurosurg 1993;79:438–41. 10.3171/jns.1993.79.3.0438 [DOI] [PubMed] [Google Scholar]
- 9.Plumb AA, Herwadkar A, Pickett G. Incidental finding of fenestration of the supraclinoid internal carotid artery with appearances on magnetic resonance angiography. Surg Radiol Anat 2010;32:165–9. 10.1007/s00276-009-0555-2 [DOI] [PubMed] [Google Scholar]
- 10.Bharatha A, Fox AJ, Aviv RI et al. CT angiographic depiction of a supraclinoid ICA fenestration mimicking aneurysm, confirmed with catheter angiography. Surg Radiol Anat 2007;29:317–21. 10.1007/s00276-007-0205-5 [DOI] [PubMed] [Google Scholar]