

Abstract
We report the successful conservative management of a non-Peutz–Jegher syndrome-associated ovarian sex cord tumour with annular tubules in a 32-year-old patient. The patient underwent a unilateral salpingo-oophorectomy by laparoscopy, and conceived spontaneously approximately 6 months after the diagnosis. After a normal term pregnancy, she underwent a contralateral laparoscopic salpingo-oophorectomy with hysterectomy. The patient is now on hormone replacement therapy and, after 30 months of follow-up, continues to present no sign of disease recurrence.
Background
Since the majority of ovarian sex cord tumour with annular tubules (SCTAT) cases are diagnosed in patients of reproductive age, we suggest that ovarian conservation should be considered to preserve fertility. To the best our knowledge, this is the first case of a successful term pregnancy after conservative surgical treatment of non-Peutz–Jegher syndrome-associated ovarian SCTAT.
Case presentation
A 32-year-old multiparous woman was admitted for chronic pelvic pain. She had regular menstruation with no abnormal uterine bleeding. During pelvic examination, a palpable mobile mass was felt in the right vaginal fornix.
Investigations
Vaginal ultrasonography revealed a well-defined, heterogeneous, solid and well vascularised right ovarian mass measuring 40×40×35 mm. The diagnosis was completed by way of a pelvic MRI, which showed a solid hypointense lesion in T1-weighted and T2-weighted sequences, indicative of an ovarian fibroma or fibrothecoma. Markedly restricted diffusion was also observed, which does not rule out the possibility of a malignant or borderline lesion, but has also been reported in fibromas and fibrothecomas (figure 1). Tumoural marker levels were normal.
Figure 1.

MRI findings. The lesion appears as a solid hypointense mass in the axial T1-weighted image (white arrow in A); as hypointense with rare hyperintense spots in the axial T2-weighted image (white arrow in B); with restricted diffusion as seen on b1000 images (white arrow in C); and with a low apparent diffusion coefficient (black arrow in D). Picture 1e corresponds to the fusion of T2 (B) and b1000 (C), thus combining anatomic and functional information.
Treatment
Given the patient's young age and her desire to become pregnant after a recent neonatal death, the conservation of the ovary was prioritised. The right ovarian tumour was completely removed during the operation, through an endoscopic bag by minilaparotomy (figure 2), avoiding morcellation and spillage (figure 3). Pathological diagnosis of an ovarian SCTAT was performed and no lymphovascular invasion or mitosis was found (figure 4). The patient had no clinical signs or family history of Peutz–Jegher syndrome. A cervical biopsy was deemed to be unnecessary given recent clinical and cervical cytology tests, which showed no malignancy. A positron emission tomography–CT scan revealed no extended disease in the pelvic or para-aortic nodes.
Figure 2.

Laparoscopic view of the ovarian mass.
Figure 3.
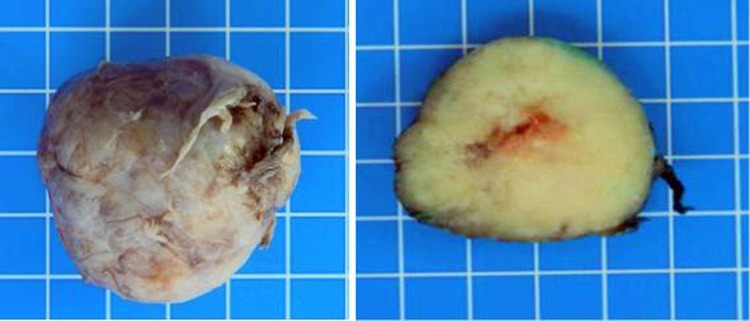
Macroscopic view of the whole ovarian mass (left). Cross-section of the mass (right).
Figure 4.
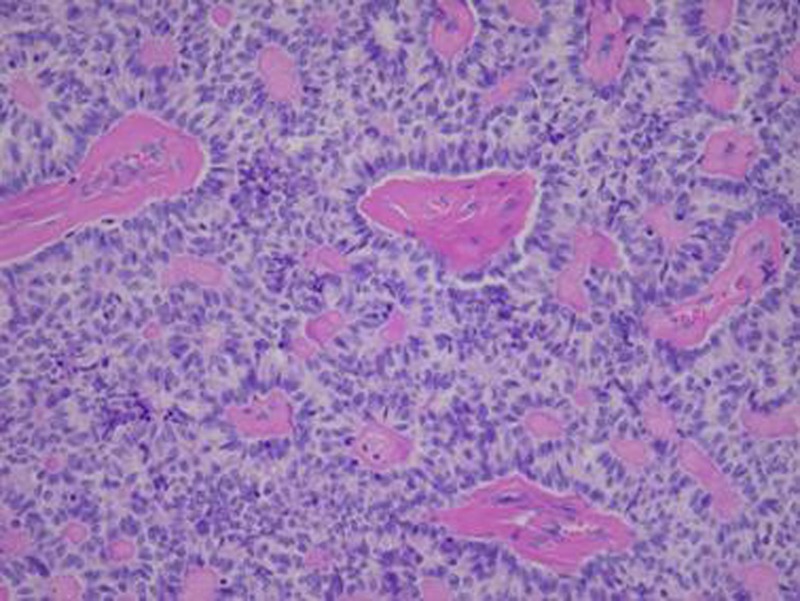
Microscopic view of the ovarian mass.
Following removal of the tumour, the patient underwent a laparoscopic surgical staging including a unilateral right salpingo-oophorectomy with peritoneal washing and peritoneal biopsies. During the operation, the left ovary and fallopian tube were found to be macroscopically normal. Microscopic examination of the right salpingo-oophorectomy, as well as the peritoneal washing and biopsies, showed no malignancy. The patient's fertility was preserved and she was advised to try to become pregnant soon.
Outcome and follow-up
The patient conceived spontaneously 6 months after the diagnosis and experienced a normal term pregnancy. Since she had previously given birth via Caesarean section, the same was scheduled for this pregnancy at 39 weeks of amenorrhoea. During the operation, the left ovary and fallopian tube were found to be macroscopically normal. A contralateral laparoscopic salpingo-oophorectomy with hysterectomy was planned to take place 24 months after the initial diagnosis. Histological samples from the resected specimens showed no evidence of malignancy. The patient is now following a hormone replacement therapy and, after 30 months of follow-up examinations, has had no recurrence of disease.
Discussion
According to the 2014 WHO classification and tumour morphology, ovarian sex cord stromal tumours are relatively rare, comprising of only 8% of all primary ovarian neoplasms.1 In contrast with epithelial ovarian cancer, the majority of patients with malignant sex cord-stromal cancer are diagnosed in the early stage.2
Ovarian SCTATs were first described by Scully in 1970.3 Subsequent case reports have tried to shed light on the histogenesis and prognosis of this rare pathology. The tumour is characterised by its distinctive histological appearance: sharply demarcated and rounded, well-circumscribed epithelial nests composed of ring-shaped tubules encircling hyalinised basement membrane-like material.4 Many cases of ovarian sex cord-stromal tumours have been studied with electron microscopy and, although it is not certain if the primitive cells are of granulosa or Sertoli-type origin, they can potentially be differentiated into either granulosa or Sertoli cells.5 6 Sertoli–Leydig cell tumours present similar morphological features, and have elevated oestradiol, progesterone and testosterone levels. In ovarian sex cord-stromal tumours, both oestradiol and progesterone are elevated, although testosterone levels remain normal. The development of oestrogen-dependent lesions in ovarian sex cord-stromal tumours leads to hormonal symptoms such as irregular menstrual bleeding, postmenopausal bleeding, precocious puberty, premature ovarian failure, fibroadenoma and endometriosis. Additionally, due to excess oestrogen production, patients with an ovarian sex cord-stromal tumour may develop concurrent endometrial pathologies such as endometrial hyperplasia or endometrial carcinoma.7–11
According to a large review of 74 cases, about one-third of patients with ovarian SCTAT also present with Peutz–Jegher syndrome.7 The majority of these patients have tumours that seem to be benign, bilateral, less than 3 cm in diameter and multifocal.12 13 One-third of these patients also have associated minimal-deviation adenocarcinoma of the cervix.8 14–16 Conversely, in the absence of Peutz–Jegher syndrome, tumours tend to be malignant in 15–20% of cases and are mostly large, unilateral and solitary.7 17
Standard treatment of early-stage ovarian sex cord-stromal tumours includes bilateral salpingo-oophorectomy with hysterectomy.18 For patients wishing to preserve their fertility, it is possible to perform a unilateral salpingo-oophorectomy with a diagnostic curettage in order to exclude endometrial hyperplasia or carcinoma. However, no evidence-based surgical treatment protocol exists due to a lack of adequate data in the literature concerning the behaviour and long-term prognosis of these tumours. Staging procedures such as omental biopsy and ipsilateral pelvic and para-aortic lymph node sampling might be effective complementary treatments because lymph node metastasis is the major cause of ovarian sex cord-stromal tumour spread,19 but these are generally recommended for tumours with histological features suggestive of malignant potential such as a high mitotic index or lymphatic invasion. In the case of ovarian sex cord-stromal tumours associated with Peutz–Jegher syndrome, the preservation of fertility by ovarian conservation is possible due to the benign behaviour of the tumour.7 In one case where no Peutz–Jegher syndrome was present, Juhnke et al20 reported a successful term pregnancy, without any surgical treatment before or during the pregnancy.
The decision to treat our patient with a unilateral salpingo-oophorectomy was based on three parameters: (1) the fact that only one ovary was affected, (2) the patient's desire to become pregnant and (3) the absence of histology suggestive of malignant potential. The diagnosis of ovarian SCTAT had no negative impact on fertility, as in the meantime our patient conceived spontaneously. Owing to a lack of adequate literature concerning the long-term prognosis of these tumours, we proceeded to undertake a contralateral salpingo-oophorectomy and hysterectomy after the normal term pregnancy was completed.
Learning points.
Ovarian sex cord tumour with annular tubules (SCTAT) is characterised by low-grade malignancy and possible late recurrence between 3 and 8 years after diagnosis.19
The behaviour and long-term prognosis of ovarian SCTAT is still unknown.
The majority of patients with ovarian SCTAT are of reproductive age,13 20 21 which raises the major issue of ovarian conservation.14
A multidisciplinary approach involving specialists (gynaecologist surgeon, oncologist, reproductive endocrinologist, pathologist, radiologist and oncogeneticist) is encouraged and justified.
Footnotes
Contributors: KC was involved in reporting the case. DB was involved in reporting the radiological images. J-CT was involved in reporting the histological images. JD was involved in reporting and reviewing the case.
Competing interests: None declared.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Kurman JR, Carcangiu ML, Herrington CS et al. . WHO classification of tumor of female reproductive organs. Lyon: IARC Press, 2014. [Google Scholar]
- 2.Quirk JT, Natarajan N. Sex cord-stromal tumors of the ovary: tumors with granulosa and Sertoli–Leydig elements. Gynecol Oncol 2005;97:519–23. 10.1016/j.ygyno.2005.02.007 [DOI] [PubMed] [Google Scholar]
- 3.Scully RE, Sobin LH. Histological typing of ovarian tumors. World Health Organization international histological classification of tumors. 2nd edn Berlin: Springer, 1999. [Google Scholar]
- 4.Song SH, Lee JK, Saw HS et al. . Peutz-Jeghers syndrome with multiple genital tract tumors and breast cancer: a case report with a review of literatures. J Korean Med Sci 2006;21:752–7. 10.3346/jkms.2006.21.4.752 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Hart WR, Kumure N, Crissman JD. Ovarian neoplasms resembling sex cord tumors with annular tubules. Cancer 1980;45:2352–63. [DOI] [PubMed] [Google Scholar]
- 6.Ahn GH, Chi JG, Lee SK. Ovarian sex cord tumor with annular tubules. Cancer 1986;57:1066–73. [DOI] [PubMed] [Google Scholar]
- 7.Young RH, Welch WR, Dickersin R. Ovarian sex cord tumor with annular tubules: review of 74 cases including 27 with Peutz-Jeghers syndrome and four with adenoma malignum of the cervix. Cancer 1982;50:1384–402. [DOI] [PubMed] [Google Scholar]
- 8.Srivatsa PJ, Keeney GL, Podratz KC. Disseminated cervical adenoma malignum and bilateral ovarian sex cord tumors with annular tubules associated with Peutz-Jeghers syndrome. Gynecol Oncol 1994;53:256–64. 10.1006/gyno.1994.1127 [DOI] [PubMed] [Google Scholar]
- 9.Magu SK, Malaviya AK, Behl AK et al. . Ovarian sex cord-tumor with Peutz-Jeghers polyp and giant keratoacanthoma. MJAFI 2007;63:289–91. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Griffith LM, Carcangiu ML. Sex cord-tumor with annular tubules associated with endometriosis of the fallopian tube. Am J Clin Pathol 1991;96:259–62. [DOI] [PubMed] [Google Scholar]
- 11.Garcia-Galiana S, Tortajada M, Monteagudo C et al. . Ovarian sex cord tumor in a woman with premature ovarian failure. Fertil Steril 2001;76:1264–6. 10.1016/S0015-0282(01)02907-7 [DOI] [PubMed] [Google Scholar]
- 12.Rodu B, Martinez MG. Peutz-Jeghers syndrome and cancer. Oral Surg 1984;58:584–8. 10.1016/0030-4220(84)90084-7 [DOI] [PubMed] [Google Scholar]
- 13.Lele SM, Sawh RN, Zaharopoulos P et al. . Malignant ovarian sex cord tumor with annular tubules in a patient with Peutz-Jeghers syndrome: a case report. Mod Pathol 2000;13:466–70. 10.1038/modpathol.3880079 [DOI] [PubMed] [Google Scholar]
- 14.Gibbon DG. Conservative management of sex cord tumors with annular tubules of the ovary in women with Peutz-Jeghers syndrome. J Pediatr Hematol Oncol 2005;27:630–2. 10.1097/01.mph.0000188302.97324.6d [DOI] [PubMed] [Google Scholar]
- 15.Outwater EK, Huang AB, Dunton CJ et al. . Papillary projections in ovarian neoplasms: appearance on MRI. J Magn Reson Imaging 1997;7:689–95. 10.1002/jmri.1880070414 [DOI] [PubMed] [Google Scholar]
- 16.Papageorgiou T, Stratakis CA. Ovarian tumors associated with multiple endocrine neoplasias and related syndromes. Int J Gynecol Cancer 2002;12:337–47. 10.1046/j.1525-1438.2002.01147.x [DOI] [PubMed] [Google Scholar]
- 17.Scully RE. Sex cord stromal tumor with annular tubules a distinctive ovarian tumor of the Peutz-Jegher syndrome. Cancer 1970;25:1107–21. [DOI] [PubMed] [Google Scholar]
- 18.Nosov V, Park S, Rao J et al. . Non-Peutz-Jeghers syndrome associated ovarian sex cord tumor with annular tubules: a case report. Fertil Steril 2009;92:1497.e5–8. 10.1016/j.fertnstert.2009.07.1002 [DOI] [PubMed] [Google Scholar]
- 19.Shen K, Wu PC, Lang JH et al. . Ovarian sex cord tumor with annular tubules: a report of six cases. Gynecol Oncol 1993;48:180–4. 10.1006/gyno.1993.1030 [DOI] [PubMed] [Google Scholar]
- 20.Juhnke I, Deichert U, Ruschoff J. Sex cord stromal tumor with annular tubules in a sterility patient. Geburtshilfe Frauenheilkd 1991;51:150–3. [German]. 10.1055/s-2007-1023694 [DOI] [PubMed] [Google Scholar]
- 21.Scully RE. Hormonally active ovarian tumors. Verch Deutsch Ges Pathol 1997;81:245–52. [PubMed] [Google Scholar]