

Description
We report two cases of rare left circumflex artery (LCX) anomalies: one case of absent LCX with super-dominant right coronary artery (RCA) and another of anomalous origin of LCX from right coronary sinus.
Case 1: A 48-year-old woman presented with exertional dyspnoea. Echocardiography was normal. CT coronary angiography (on 256-slice CT scanner) revealed absent LCX in the left atrioventricular groove. The RCA was prominent and posterolateral branch was supplying the posterior wall of left ventricle. LCX territory was supplied by the small branches from diagonal arteries of left anterior descending artery (figures 1 and 2).
Figure 1.
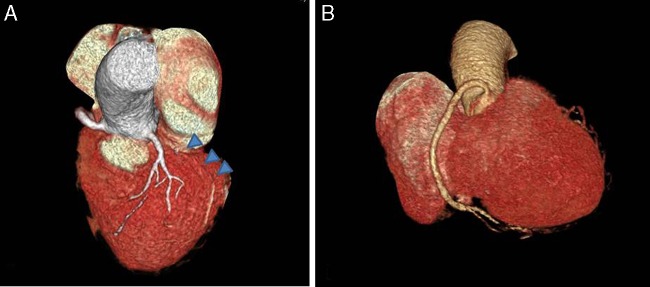
CT angiography volume-rendering technique images showing absent left circumflex artery in the left atrioventricular groove (arrowheads in A) and dilated right coronary artery (B).
Figure 2.
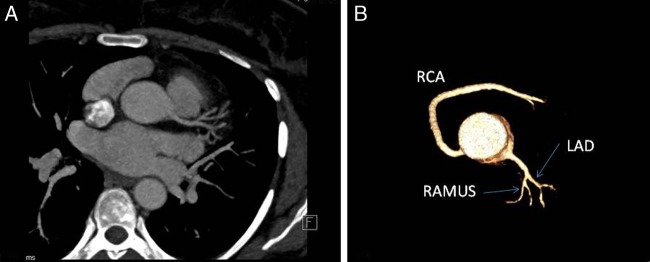
Axial MIP (A) and VRT (B) images showing division of left main coronary artery into LAD and Ramus intermedius with absent LCX (LAD, left anterior descending; LCX, left circumflex artery; MIP, maximum intensity projection; RCA, right coronary artery; VRT, volume-rendering technique).
Case 2: A 58-year-old man presented with atypical chest pain. Echocardiography was normal. CT angiography revealed anomalous origin of LCX from the right coronary sinus, adjacent to the origin of RCA (type II variant). The LCX was retroaortic in course, traversing between the aortic root and left atrium. No compression or luminal narrowing was seen (figures 3 and 4).
Figure 3.
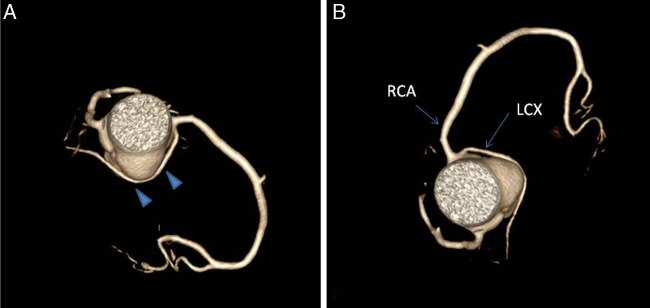
VRT images showing anomalous origin of LCX from right coronary sinus (arrows in B) with retroaortic course (arrowheads in A; LCX, left circumflex artery; RCA, right coronary artery; VRT, volume-rendering technique).
Figure 4.
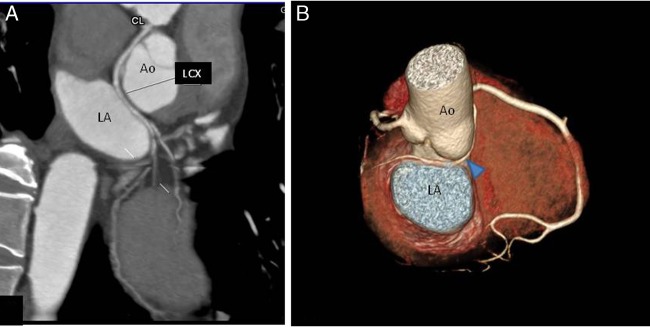
MIIP (A) and VRT(B) images showing LCX coursing between Ao and LA (Ao, aorta; CL, cycle length; LA, left atrium; MIP, maximum intensity projection; VRT, volume-rendering technique).
Congenital absence of LCX is a very rare anomaly with incidence of 0.003% in patients undergoing coronary angiography. CT coronary angiography is advantageous over catheter angiography in differentiating between congenital absence and complete obstruction. It also helps in delineating the course of the vessel in relation to the surrounding cardiac chambers. These patients may be symptomatic due to a steal phenomenon.1
Anomalous origin of LCX from right coronary sinus is the most common congenital variant with prevalence of 0.18–0.67%. These patients may develop coronary symptoms due to kinking/compression in their retroaortic course (malignant course).2
Learning points.
Most patients of congenitally absent left circumflex artery (LCX) are asymptomatic; however, they may develop symptoms due to transient ischaemia of other coronary arterial territories due to stealing of blood in LCX.
- An anomalous origin of LCX from right coronary sinus is the most common congenital variant and is divided into three types3:
- Type I: Separate ostia for right coronary artery (RCA) and LCX.
- Type II: Common ostia in the right sinus.
- Type III: LCX arising as a branch of the proximal RCA.
CT coronary angiography is an excellent non-invasive imaging modality for detection of coronary artery anomalies.
Footnotes
Competing interests: None declared.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Hongsakul K, Suwannanon R. Congenital absence of left circumflex artery detected by computed tomography coronary angiography: a case report. Case Rep Vasc Med 2012;2012:204657 doi:10.1155/2012/204657 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Mohsen GA, Mohsin KG, Forsberg M et al. Anomalous left circumflex artery from the right coronary cusp: a benign variant? J Invasive Cardiol 2013;25:284–7. [PubMed] [Google Scholar]
- 3.Page HL, Engel HJ, Campbell WB et al. Anomalous origin of the left circumflex coronary artery: recognition, angiographic demonstration and clinical significance. Circulation 1974;50(4):768–73 doi:10.1161/01.CIR.50.4.768 [DOI] [PubMed] [Google Scholar]