

Abstract
Study Objectives:
There is a need for the accurate assessment of circadian phase outside of the clinic/laboratory, particularly with the gold standard dim light melatonin onset (DLMO). We tested a novel kit designed to assist in saliva sampling at home for later determination of the DLMO. The home kit includes objective measures of compliance to the requirements for dim light and half-hourly saliva sampling.
Design:
Participants were randomized to one of two 10-day protocols. Each protocol consisted of two back-to-back home and laboratory phase assessments in counterbalanced order, separated by a 5-day break.
Setting:
Laboratory or participants' homes.
Participants:
Thirty-five healthy adults, age 21–62 y.
Interventions:
N/A.
Measurements and Results:
Most participants received at least one 30-sec epoch of light > 50 lux during the home phase assessments (average light intensity 4.5 lux), but on average for < 9 min of the required 8.5 h. Most participants collected every saliva sample within 5 min of the scheduled time. Ninety-two percent of home DLMOs were not affected by light > 50 lux or sampling errors. There was no significant difference between the home and laboratory DLMOs (P > 0.05); on average the home DLMOs occurred 9.6 min before the laboratory DLMOs. The home DLMOs were highly correlated with the laboratory DLMOs (r = 0.91, P < 0.001).
Conclusions:
Participants were reasonably compliant to the home phase assessment procedures. The good agreement between the home and laboratory dim light melatonin onsets (DLMOs) demonstrates that including objective measures of light exposure and sample timing during home saliva sampling can lead to accurate home DLMOs.
Clinical Trial Registration:
Circadian Phase Assessments at Home, http://clinicaltrials.gov/show/NCT01487252, NCT01487252.
Citation:
Burgess HJ, Wyatt JK, Park M, Fogg LF. Home circadian phase assessments with measures of compliance yield accurate dim light melatonin onsets. SLEEP 2015;38(6):889–897.
Keywords: circadian, compliance, light, melatonin
INTRODUCTION
The most reliable measure of central circadian timing in humans is the onset of melatonin secretion, when measured in dim light conditions (dim light melatonin onset, DLMO).1,2 Melatonin typically begins to rise in the 2–3 h before the usual onset of nocturnal sleep,3 but must be measured in dim light because light can suppress melatonin secretion.4 The measurement of the DLMO is now encouraged in the latest diagnostic criteria for circadian rhythm sleep disorders (International Classification of Sleep Disorders, Third Edition).5 Additionally, measuring the DLMO can help to optimize the treatment of circadian rhythm sleep disorders with melatonin or bright light6–8 and help to prevent patients from receiving treatment at the wrong circadian time, which risks worsening their condition.7,9 Similarly, measuring the DLMO or “phase typing” patients with winter depression can assist in optimizing the timing of bright light treatment.10
The DLMO is most frequently assessed in a research laboratory or clinic. Research participants or clinical patients are required to arrive at the facility approximately 6–8 h before their usual bedtime, and are guided by staff to remain in dim light, and to give samples every half hour or hour until their usual bedtime or even later.1,3 Melatonin can be measured in plasma, but melatonin is most easily assessed noninvasively from saliva samples.11 Additionally, saliva is often sampled more frequently than the urinary melatonin metabolite 6-sulphatoxymelatonin, allowing for greater precision in measurement.11 The need for staff and space considerably increases the expense and inconvenience associated with measuring the DLMO.12 Furthermore, some participants and/or patients are reluctant to stay late or overnight in an unfamiliar laboratory or clinic. Thus, the possibility of having research participants or patients collect saliva samples in their own homes instead of having to stay in the laboratory or clinic at night is very appealing.
However, other concerns arise when saliva sampling occurs at home and is not supervised by staff. The first is the need to ensure people are in sufficiently dim light to avoid melatonin suppression, and subsequent circadian phase shifting. To date, only one study has compared DLMOs generated from home saliva samples to DLMOs generated from saliva samples collected in the laboratory.12 In this study, light exposure at home was not measured, but the authors estimated that approximately 20% of the home DLMOs were suppressed by light, as these home DLMOs occurred more than 1 h later in time than the corresponding laboratory DLMOs. A second concern surrounding home saliva sampling is sample timing. For example, in one study of home saliva sampling for later determination of cortisol levels, compliance to scheduled sample times was poor, especially when participants were not informed that they were being electronically monitored.13 On average, participants who were unaware they were being monitored gave saliva samples more than 2 h from the scheduled sample times, but nevertheless reported significantly better compliance to the study investigators.13 The authors concluded that “researchers cannot rely on participants' self-reports of sampling times”13.
In response to the increasing need for accurate home DLMOs, we have developed a kit designed to facilitate home saliva sampling while including objective measures of compliance to the requirement for dim light levels and scheduled times for saliva samples. After collection, examination of the light levels and sample times can assist in determining whether the home procedures were correctly followed. Light exposure is measured in 30-sec epochs by a photosensor worn around the neck on a cord and pinned to the outermost clothing. This placement of the photosensor reduces the risk of sleeves covering a wrist-worn photosensor. Sample times are recorded by use of a medication monitoring device that tracks the opening of a vial that contains cotton swabs used for generating a saliva sample. The kit also includes a dispenser with prepared labels in chronological order, so the subject only has to attach a label and is not required either to select a specific tube, or to write the correct time on the tube, both of which can lead to errors in sample coding.12,14 To our knowledge this is the first kit for home saliva sampling that includes objective markers of light exposure and saliva sample timing, and a system to reduce sample labeling errors. Here, as a first test of this kit, we report on the subject compliance to the home procedures and on the accuracy of the home DLMOs collected with this kit, in a back-to-back comparison with DLMOs collected in the laboratory.
METHODS
Participants
Thirty-five healthy participants participated in the study year round (12 in spring, 4 in summer, 7 in fall, 12 in winter). All participants were medication free, consumed only moderate caffeine (< 300 mg/day) and alcohol doses (< 2 drinks/day), and had a body mass index between 18.5–29.8 kg/m2. Based on their responses to screening questionnaires, all participants had no medical (Tasto Health Questionnaire15), psychiatric (Minnesota Multiphasic Personality Inventory-2,16 Beck Depression Inventory,17 Personal Inventory for Depression and Seasonal Affective Disorder18), or sleep disorders (Pittsburgh Sleep Quality Index,19 Insomnia Severity Index,20 Berlin Sleep Apnea Questionnaire,21 International Restless Legs Syndrome Study Group consensus criteria for restless leg syndrome22) and were not extreme chronotypes (Owl and Lark Questionnaire23). All participants were required to pass a urine drug screen for common drugs of abuse and nicotine; two participants failed the urine test and were dropped from the study. A third subject was dropped from the study after an urgent work assignment conflicted with study participation. The remaining sample of 32 participants consisted of 16 men, 16 women; 21–62 y, mean age ± standard deviation 39.9 ± 13.9 y. There were 11 moderate morning, 16 neither types, and five moderate evening types in the final sample. Almost all participants had some college education (94% of sample), with the remainder having only completed high school. Most participants were employed on a part-time (44% of sample) or full-time (31% of sample) basis, with the remainder reporting that they were not working. The majority of participants were not students (88% of sample), with only a minority reporting student status (12% of sample). No subject was color blind, as determined by the Ishihara test for color blindness. All participants had not worked any night shifts in the 2 y prior to the study and had not traveled across more than one time zone in the 2 mo preceding the study. All participants reported no previous experience with saliva sampling, and had not previously participated in any research study in our laboratory. Non-steroidal anti-inflammatory drugs were not permitted throughout the study because they can suppress melatonin.24 All participants gave written informed consent prior to their participation. The study was approved by the Rush University Medical Center Institutional Review Board.
Protocols
Participants were randomized in groups of one to three people to one of two 10-day protocols (Figure 1). In Protocol A, participants completed a home circadian phase assessment first, followed by a laboratory circadian phase assessment the next day. Participants then had a 5-day break where they returned to their usual sleep schedule at home, before completing a laboratory phase assessment, followed the next day by a second home phase assessment. In Protocol B, participants completed a laboratory phase assessment first, followed by a home phase assessment the next day. Participants then had a 5-day break where they returned to their usual sleep schedule at home, before completing a home phase assessment, followed the next day by a laboratory phase assessment. Sixteen participants completed Protocol A and 16 participants completed Protocol B.
Figure 1.

Sample protocols for a subject who typically slept from 23:00 to 07:00. Participants were randomized to Protocol A or Protocol B. Protocol A consisted of a home phase assessment, a laboratory phase assessment, a 5-day break, a laboratory phase assessment, and a home phase assessment. Protocol B consisted of a laboratory phase assessment, a home phase assessment, a 5-day break, a home phase assessment and a laboratory phase assessment. The gray rectangles represent the time required for dim light. The dot represents the time of the first saliva sample, with saliva sampling continuing every 30 min up until 2 h after average bedtime. The black rectangles represent scheduled sleep times. Square brackets indicate approximate arrival and departure times from the laboratory.
The protocol for each subject was tailored to each individual's habitual sleep times collected in the week before the study start with daily sleep diaries. Subjects were not required to follow a fixed sleep-wake schedule during this week. On average across the sample, each participant's bedtime varied by a maximum of 89.8 min and each participant's wake time varied by a maximum of 114.5 min during this week. Saliva sampling started 6 h before and ended 2 h after each subject's average bedtime (Figure 1). After the last saliva sample, participants slept at home or in the laboratory before waking at their average wake time, to minimize any shifts in circadian timing. The average bedtime and wake time for the sample was 23:43 ± 0.9 h and 07:41 ± 0.7 h respectively, with average bedtime in the sample ranging from 21:30 to 01:00 and average wake time ranging from 06:30 to 09:00. Participants were required to take a 2-h nap prior to the second and fourth phase assessment (whether at home or in the laboratory) to reduce the sleep deprivation from the night before. Driving was not permitted on any study day where the protocol had led participants to be sleep deprived. All participants wore a wrist actigraphy monitor (30-sec epochs, Actiwatch Spectrum, Respironics, Bend, OR) on their nondominant wrist throughout the 10-day study to ensure compliance to the study protocol.25
Laboratory Circadian Phase Assessments
When in the laboratory participants were continuously supervised by research staff, and guided through the laboratory procedures. Participants were required to remained awake and seated in dim light (< 5 lux, at level of the eyes, in direction of gaze, measured every 2 h, Extech 403125 light meter, Nashua, NH) starting 6.5 h before their average bedtime (Figure 1). After 30 min in the dim light, participants were prompted by staff to give a saliva sample every 30 min using Salivettes (Sarstedt, Newton, NC). The participants tipped the cotton swab from the Salivette into their mouths, and rolled the cotton swab in their mouths for up to 5 min until saturated, before spitting it back into the Salivette. This procedure continued every 30 min until the last saliva sample, which occurred 2 h after their average bedtime. Toothpaste or mouthwash was not allowed during the phase assessments. Small snacks and fluids were permitted, except in the 10 min before each sample, and participants were required to rinse and brush their teeth with water while remaining seated 10 min before each sample if they had consumed food or drink. Participants remained seated throughout the laboratory phase assessment except for bathroom trips, but these were not permitted in the 10 min before each sample. Participants were not permitted to consume any alcohol or caffeine at least 24 h before each phase assessment and were breathalyzed on arrival at the laboratory.
Home Circadian Phase Assessments with Measures of Compliance
The home phase assessments were designed to be as similar as possible to the laboratory phase assessments, with the addition of objective markers of compliance to the requirement for dim light and correct sampling times. Participants met a staff member at the laboratory earlier in the day of each home phase assessment. During these appointments, participants received a “light medallion” (Actiwatch Spectrum, Respironics, Bend, OR, 30-sec epochs, with wrist band removed, strung onto a cord worn around the neck with an attached safety pin), were instructed on the home procedures, witnessed a demonstration of how to collect a saliva sample, and received a home saliva collection kit. As for the laboratory phase assessments, participants were not permitted to consume any alcohol or caffeine at least 24 h before each home phase assessment and were breathalyzed during their visit to the laboratory. Participants were advised of the need to prepare food ahead of time so they could snack in between the half hourly saliva samples at home. A return appointment was made for the next day, so that participants could return the home kit. Participants were informed that their compliance to the home procedures was being monitored and the data would be examined by staff in their presence during the return appointment. The time taken to explain the home kits and home procedure varied between 20 to 30 min, depending on questions from participants.
The home saliva collection kit consisted of the following: a timer (PalmOne Tungsten E Handheld, programmed with Palm Desktop 4.1.4 software, Hewlett Packard, Palo Alto, CA), a paper checklist, a foam test tube rack, a small insulated bag with removable ice pack, 17 Salivettes with the cotton swabs removed, a vial with a MEMS TrackCap lid (microchip time stamps each lid opening, MWV Healthcare, Richmond VA) with the 17 cotton swabs inside, a dispenser with prepared labels in chronological order, a soft toothbrush, eight Tylenol pills to replace any nonsteroidal anti-inflammatory drugs participants may wish to take in case of headaches and an event log for participants to note any odd events during the home phase assessment. Participants were offered a night light to assist in dimming their home bathrooms and 24 participants (75%) reported using the night light. The kit also contained three spare Salivettes, each with a cotton swab inside in case of an error with a saliva sample. The home kit was packed into a black messenger bag for easy transport home.
Upon arrival at home, participants were instructed to follow the checklist whenever prompted by the preset alarms on the timer, and to check off tasks on the checklist when completed, to assist them in working through the tasks. The first alarm occurred 30 min before the first saliva sample, at which time the checklist prompted participants to close all blinds and curtains in their home environment, to reduce exposure to any outdoor light, and to turn off or dim indoor lights (including bathroom lights) to the lowest level possible while still permitting the reading of the checklist. Participants were also instructed to dim the screens of electronic devices they anticipated using during the home phase assessment, including televisions, computers, cell phones, and music-playing devices. The light from the timer and night light were dim (∼1.5 lux and 3.5 lux respectively, at level of eyes, in direction of gaze, measured ∼42 cm from eye, Extech 403125 light meter). The checklist also prompted participants to place the test tube rack and removable ice pack in their freezer, and to use the attached safety pin to pin the light medallion to their outer most clothing. All other pieces of the home kit were to be placed on a nearby table for easy access. As in the laboratory phase assessments, small snacks and fluids were permitted, except in the 10 min before each sample, when participants were prompted by the alarm/checklist to brush their teeth with the toothbrush if they had eaten any food, to rinse with water if they had consumed anything apart from water, and to remain seated until after the next saliva sample. Compliance to this instruction was not assessed. At each scheduled time for a saliva sample, the alarms/ checklist prompted participants to open the Track Cap lid (which recorded time of opening), remove a cotton swab from the vial, replace the Track Cap lid, roll the cotton swab in their mouths for up to 5 min until saturated, spit the cotton swab into an empty Salivette, attach a label from the label dispenser to the Salivette, and place the Salivette in the test tube rack in their freezer. As in the laboratory phase assessments, showers and exercise, toothpaste or mouthwash was not allowed during the home phase assessments. The checklist also contained the telephone number of a staff member to call if any questions came up during the home phase assessment, although only two participants called the number, with questions about the timer. After the last saliva sample was obtained, the checklist prompted participants to remove the light medallion and place it face up on their bedside table, turn off all lights, and to go to bed to sleep. The following morning, at the participants' average wake time, the checklist prompted participants to put the light medallion back on. When participants were ready to return to the laboratory, the checklist instructed them to place the ice pack and frozen Salivettes in the small insulated bag, and to pack all remaining equipment into the larger messenger bag.
Preliminary Data Analysis
When participants returned to the laboratory to drop off the home kit, the research staff checked that all contents of the kit were returned, and participants were asked how many people were home during the home phase assessment and their respective ages. The number of people home during the home phase assessment ranged from zero to six people, and at least one other person was present for the majority of the home phase assessments (64%). The age of the people present during the home phase assessments ranged from 6 to 84 y. The light medallion was removed from the subject and downloaded, and the activity on the light medallion was checked to confirm participants were wearing the light medallion as instructed. The light levels from the 30 min before the first saliva sample to the last saliva sample were also checked, with light levels < 50 lux coded as compliant and light levels ≥ 50 lux coded as non-compliant. This light threshold was chosen based on an illuminance response curve generated in dark adapted participants, which indicates minimal melatonin suppression at light intensities < 50 lux.26 The Track Cap was also downloaded (Power-View version 3.4.1, MWV Healthcare, Richmond, VA), with any saliva samples ≤ 5 min from the scheduled time coded as compliant, and samples taken > 5 min from the scheduled time coded as noncompliant.
The Salivettes collected in the laboratory were immediately centrifuged to extract the saliva from the cotton swab and then frozen. The Salivettes collected at home were thawed, centrifuged, and then refrozen. The saliva samples were then shipped in dry ice to Solidphase Inc. (Portland, ME) which radioimmunoassayed the samples for melatonin using commercially available kits (ALPCO, Inc, Salem, NH). Each individual's saliva samples were assayed in the same batch. The first non-zero standard of this assay was 0.5 pg/mL. Intra-assay coefficients of variation for low, medium, and high levels of salivary melatonin are 20.1%, 4.1%, and 4.8%, respectively. The interassay coefficients of variation for low, medium, and high levels of salivary melatonin are 16.7%, 6.6%, and 8.4%, respectively. A DLMO was calculated for each phase assessment and defined as the clock time (with linear interpolation) when the melatonin concentration exceeded the mean of three low consecutive daytime values plus twice the standard deviation of these points.27 This low threshold more closely tracks the initial rise of melatonin.28
RESULTS
Compliance to the Scheduled Bed and Wake Times
The wrist activity revealed that all participants except two demonstrated good compliance to the study protocol, going to bed and getting out of bed at home within 15 min of the assigned times. The two noncompliant participants each slept up to 1.5 h after their assigned wake time after their first home phase assessment, but before the first laboratory phase assessment in Protocol A.
Compliance to the Requirement for Dim Light
Each of the participants completed a home phase assessment twice. Thirteen participants (41% of the sample) received at least one 30-sec epoch of light > 50 lux during both 8.5 h home phase assessments, eleven participants (34%) received such light during only one of the two home phase assessments, whereas eight participants (25%) were able to remain in dim light throughout both home phase assessments. Overall, the median frequency of 30-sec epochs > 50 lux was 2. The average difference in number of epochs > 50 lux between the two home phase assessments was 15.7 ± 34.7. Often the light > 50 lux was received in the first 30 min of the home phase assessment (58% of the time), as participants began to close their blinds and curtains and dimmed their inside lighting. When light > 50 lux did occur during the 8.5 h home phase assessment, the duration lasted between 30 sec to 95 min, and on average lasted for 8.8 ± 16.3 min (or on average 1.7% of the home phase assessment). The average light intensity during home phase assessments was 4.5 lux, with a range of zero to 13,047 lux (the maximum occurring in the first 2 min of the home phase assessment as the subject closed her blinds). The average light intensity of the epochs with light > 50 lux was 158.5 lux. The most common activity during the home phase assessments was watching television (63%), followed by reading (19%), using a computer (9%), and housework (9%). There was no significant relationship between the occurrence of light > 50 lux during the home phase assessments and subject characteristics such as age, sex, race, education, employment status, student status, number of people home, youngest age of people home, oldest age of people home, and whether the first sample was before or after sunset (all P > 0.12). There was a trend for more participants in Protocol A (81%) than in Protocol B (50%) to receive light > 50 lux in the first home phase assessment (chi-square, P = 0.063), but not in the second home phase assessment (chi-square, P = 0.48). This is most likely because in the first home phase assessment participants in Protocol A had not yet experienced the dim light in a laboratory phase assessment.
Compliance to Scheduled Sample Times
Three participants (9% of the sample) collected at least one saliva sample more than 5 min from a scheduled sample time in both home phase assessments, 11 participants (34%) collected at least one saliva sample more than 5 min from a scheduled sample time in only one home phase assessment, and 18 participants (56%) had no problem collecting saliva samples within 5 min of the scheduled times in both home phase assessments. Two subjects missed one sample during their first home phase assessment. The majority of sample errors resulted in samples collected within 11 min of the scheduled time (88% of the errors), and mostly occurred when participants mistakenly collected a saliva sample when the timer/checklist prompted them to brush their teeth and rinse with water in the 10 min before a scheduled sample. There was no significant relationship between compliance to the scheduled sample times during the home phase assessments and subject characteristics such as age, sex, race, education, employment status, student status, number of people home, youngest age of people home, oldest age of people home, or whether the subject participated in Protocol A or B (all P ≥ 0.15).
Dim Light Melatonin Onsets
One subject who ran in Protocol A consistently secreted a low level of melatonin (< 5 pg/mL) and there was no discernible onset in melatonin secretion in all home and laboratory phase assessments. Thus, there were no DLMOs from this subject. After all of the home DLMOs were calculated, they were cross checked against the light levels on the light medallion and sample times from the TrackCap. If a sampling error affected one of the two melatonin data points below and above the threshold, which are used in the calculation of the DLMO, the home DLMO was considered invalid. This occurred on two occasions. Similarly, if light exposure was > 50 lux within 30 min of the two melatonin data points used in the calculation of the DLMO, the home DLMO was considered likely suppressed and invalid. This occurred on three occasions. This rule was derived from data showing melatonin rebounded in ∼30 min after a 12 min exposure to very bright light (∼10,000 lux, Figure 4 in Chang et al.29). Thus, of the 62 home DLMOs calculated, 57 (92%) were considered valid.
Figure 4.
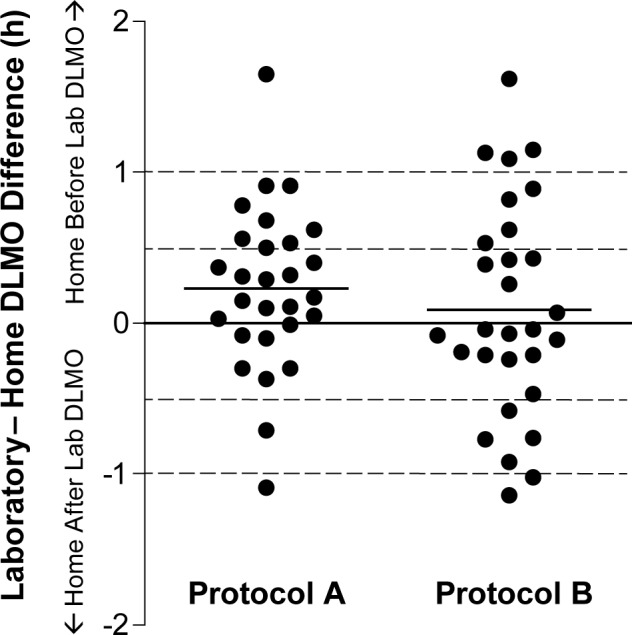
The distribution of the difference between the laboratory dim light melatonin onsets (DLMOs) and home DLMOs, calculated by subtracting each home DLMO from its corresponding laboratory DLMO. The zero line represents no difference between the DLMOs, a positive difference reflects the home DLMO occurring earlier in time than the corresponding laboratory DLMO, while a negative difference reflects the home DLMO occurring after the corresponding laboratory DLMO. The solid lines represent the mean differences in each protocol. The dashed lines represent a 30-min difference and a 1-h difference between the home and laboratory DLMOs.
The home and laboratory DLMOs were highly correlated (r = 0.91, P < 0.001) (Figure 2). Individual examples of when the home DLMO occurred more than 30 min before, at approximately the same time, or more than 30 min after the laboratory DLMOs are shown in Figure 3. Each valid home DLMO was subtracted from the laboratory DLMO that occurred immediately before or after that home DLMO. Thus a positive number indicated the home DLMO occurred before the laboratory DLMO, whereas a negative number indicated the home DLMO occurred after the laboratory DLMO. Overall the average difference between the home and laboratory DLMO in each pair of DLMOs was 0.16 ± 0.63 h, reflecting that on average the home DLMO occurred before the laboratory DLMO. However, there was no significant difference between the home and laboratory DLMOs (paired t test, P > 0.05). The distribution of the differences between each pair of home and laboratory DLMOs was normally distributed (skew = 0.07 ± 0.32, kurtosis = −0.01 ± 0.62, Figure 4). In 33 cases (58% of the data) the home DLMO occurred within 30 min of the laboratory DLMO. In 16 cases (28% of the data) the home DLMO occurred more than 30 min earlier than the laboratory DLMO (maximum difference 1.65 h earlier). In eight cases (14% of the data), the home DLMO occurred more than 30 min after the laboratory DLMO (maximum difference 1.14 h later). In both protocols it was less common for the home DLMO to occur after the laboratory DLMO (as might be expected if melatonin suppression was occurring during the home phase assessments). Similarly, the magnitude of the difference between the home and laboratory DLMOs was always less when the home DLMO occurred after the laboratory DLMO. Thus in sum, there was no evidence that the home phase assessments systematically led to later DLMOs than those measured in the laboratory. In 58% of cases the home DLMO occurred within 30 min of the laboratory DLMO and in 88% of cases the home DLMO occurred within 1 h of the laboratory DLMO. The average difference between the two home DLMOs was 0.36 ± 0.68 h and the average difference between the two laboratory DLMOs was 0.48 ± 0.86 h. The average difference between the two home DLMOs and the average difference in number of epochs > 50 lux between the two home phase assessments were not significantly correlated (r = 0.19, P = 0.33).
Figure 2.
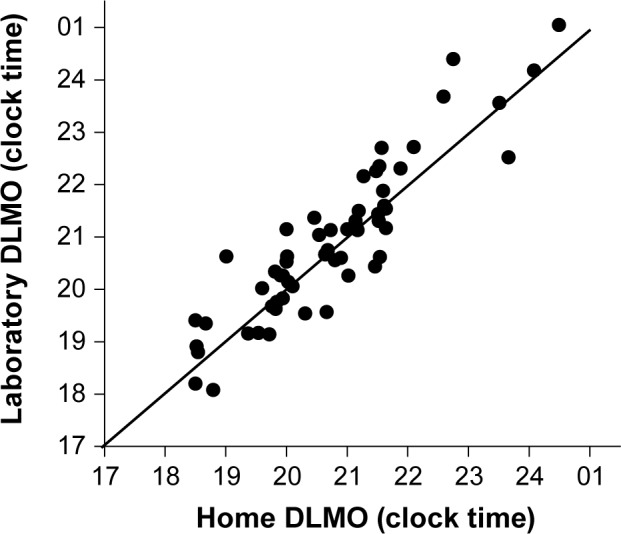
The clock time of dim light melatonin onsets (DLMOs) collected in laboratory phase assessments versus home phase assessments. The two measures were highly correlated (r = 0.91, P < 0.001). The line is the line of unity.
Figure 3.
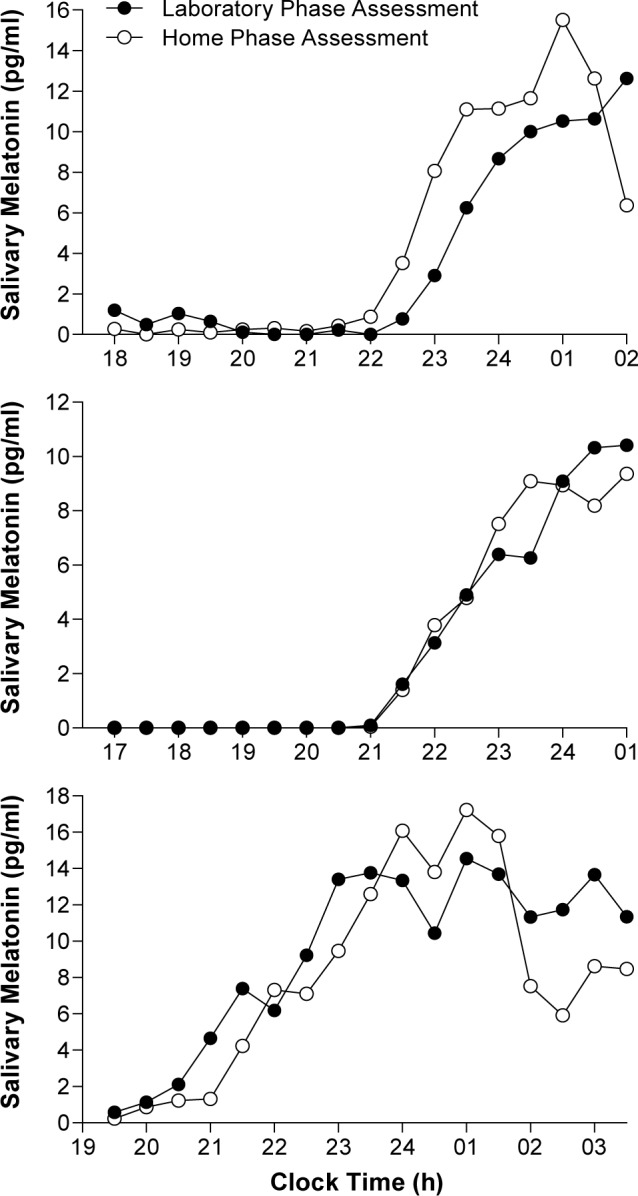
Individual melatonin profiles collected in a home phase assessment either the day before or day after a laboratory phase assessment. Top panel: An example of when the home dim light melatonin onset (DLMO) occurred before the laboratory DLMO. Middle panel: An example of when the home DLMO occurred at the same time as the laboratory DLMO. Bottom panel: An example of when the home DLMO occurred after the laboratory DLMO.
DISCUSSION
This study is the first test of a novel kit designed to facilitate home saliva sampling for later determination of the DLMO. The home procedure included objective measures of compliance to the requirement for dim light and scheduled times for saliva samples, and a system to reduce labeling errors. Overall participants were reasonably compliant to the requirement for dim light. Although 75% of the participants received at least one 30-sec epoch of light > 50 lux during their home phase assessments, the average duration of light > 50 lux in these participants was less than 9 min of the required 8.5 h of dim light. Participants were also reasonably compliant to the requirement for saliva samples every half hour, with more than half of the participants collecting all their home saliva samples within 5 min of the scheduled times. Thus overall, compliance to the home procedures was good and the light data from the photo-sensor and sample timing data from the medication monitoring device indicated 92% of the home DLMOs were valid with these relatively strict criteria.
The home DLMOs correlated highly with the laboratory based DLMOs (r = 0.91). This correlation is considerably higher than the correlation between home and laboratory DLMOs previously observed in a study with no measures of light exposure or sample timing (r = 0.68).12 Importantly, the previous study and the current study used the same low threshold to calculate the DLMOs,11,27 and so the DLMOs are directly comparable. In this earlier study, 20% of home DLMOs occurred 1 h or more after the corresponding laboratory DLMOs (suggesting light-induced melatonin suppression at home),12 whereas only 4% of home DLMOs in the current sample occurred 1 h or more after the corresponding laboratory DLMO. Furthermore, the average difference between home and laboratory DLMOs was less than 10 min in the current study versus the previously observed 54 min,12 and less than the 30-min sampling rate. Indeed, the maximum difference between the home and laboratory DLMOs occurred when a home DLMO occurred 1.65 h earlier in time than the corresponding laboratory DLMO. This difference falls within the 95% confidence intervals surrounding the mean difference between two laboratory DLMOs assessed about 3 w apart in healthy participants sleeping on a fixed sleep schedule (± 30 min).30 In that study, the upper limit of the 95% confidence interval was a difference of 2.4 h between the two laboratory DLMOs.30 Similarly, the weekly difference falls within the difference observed between two laboratory DLMOs assessed at least 5 days apart in healthy participants sleeping on an ad lib schedule31 (Figure 2). The observed variability in the difference between the home and laboratory DLMOs in the current study is most likely due to the typical variations in the sleep times of the participants before each back-to-back phase assessment.32,33 By contrast, the 2 h of dim light after habitual bedtime26 and the 2 h afternoon nap before the second phase assessment34 are unlikely to have significantly shifted the DLMO. Overall, the good agreement between the home and laboratory DLMOs in this study suggests that including objective measures of light exposure and sample timing during home saliva sampling, and also informing participants that their compliance is being monitored, can lead to more accurate home DLMOs.
The home saliva sampling procedure tested here is the next step toward developing a standardized approach to measure valid DLMOs at home. Home DLMOs offer several advantages over laboratory or clinic based DLMOs, including reduced cost, and potentially greater accessibility to patient groups that are reluctant to stay overnight in a facility (e.g., postpartum women). The home procedures used in this study required participants to give half-hourly saliva samples, which is significant considering other protocols for home saliva sampling have relied on only hourly sampling.12,14 Half-hourly sampling at home was required as this higher sampling frequency is often used in the laboratory or clinic, and thus provided the optimal comparison to laboratory DLMOs.28 Nonetheless, hourly sampling may be more practical for clinical practice.28 The saliva collection window was tailored to each subject, starting 6 h before each subject's average bedtime and continuing up to 2 h after each subject's average bedtime. A similar 8-h sampling window was used previously, although it was shifted 1 h earlier, with saliva sampling starting 7 h before and ending 1 h after habitual bedtime.12 Other home saliva sampling protocols have used only a 5-h sampling window.14 In the current study the earliest DLMO relative to sampling time occurred 2 h after the first saliva sample and the latest DLMO occurred 1 h before the last sample, suggesting the full 8-h window may be needed to best capture the DLMO, at least in healthy people.
Although the kit and procedures worked quite well, there are several areas for potential improvement in future studies. One possibility is the addition of “blue blocker” glasses, which can minimize any melatonin suppression due to indoor lighting.35,36 Such glasses were not included in the kit tested here, because of the difficulty in measuring subject compliance in wearing them. Nonetheless, participants could be encouraged to wear them during home phase assessments, as in a previous study participants reported wearing them about 70% of the requested time.37 Another change could be to use a small personal electronic device such as a smart phone, as the timer in the kit instead of a personal data assistant (PDA), as the PDA was somewhat burdensome to staff, requiring careful programming of the alarms with specialized desktop software. Additionally, the staff time taken to explain the kit to each and every subject could conceivably be replaced with a short video explaining the procedure, followed by a short question and answer session with staff. Participants were also less likely to receive light > 50 lux during the home phase assessments, after they had experienced the laboratory phase assessment (< 5 lux). Thus, people may be more successful at ensuring dim light at home if they are first shown a room with appropriate dim lighting, as verified by a staff member with a light meter. Finally, participants may experience less sampling errors if they are informed that the foremost sampling error was to generate a saliva sample about 10 min early, when instead they should have been brushing their teeth to remove food particles.
The home saliva sampling procedure in this study was tested in healthy participants whose age ranged between 21–62 y. Interestingly, subject compliance to the requirement for dim light and sample times were not significantly associated with any characteristics of the participants such as their age, race, education, employment status or student status. Similarly, there were no significant relationships between characteristics of the participants' home environment and their compliance, such as the number of people home during the home phase assessment and their respective ages. One subject successfully completed both home phase assessments with six other family members present and the difference between his home and laboratory DLMOs was less than 5 min on both occasions. Nonetheless, the sample was highly educated, with 94% of subjects having started some college education, indicating further validation of the procedure may be required in a more representative sample of the general population. Nonetheless, all the participants were healthy, and the home saliva sampling kit and procedure remains to be tested in patient populations, including those with extremes of chronotype. Given the greater variability in the sleep-wake schedules of patients with various circadian rhythm sleep disorders, including delayed sleep-wake phase disorder, there is likely to be larger variability between home-and laboratory-based phase assessments. The home kit and procedures will also need validation for use in children and older adults with neurodegenerative conditions, as both will require assistance with the home procedures. As a next step we are testing the home saliva sampling procedure in patients with delayed sleep-wake phase disorder because the DLMO can be quite useful in the differential diagnosis of this disorder.38
DISCLOSURE STATEMENT
This was not an industry supported study. This research was supported by an R01 grant (AT007104) from the National Center for Complementary and Integrative Health of the National Institutes of Health to Dr. Burgess. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Complementary and Alternative Medicine or the National Institutes of Health. The authors have indicated no financial conflicts of interest.
ACKNOWLEDGMENTS
The authors thank Marissa Dziepak, Andrew Eiden, James Farrell, Amy Feehan, Jazmin Garcia, Anna Ishikawa, Toni Iurcotta, Julia Kleinhenz, Devon Langston, Thomas Molina, Brock Peiffer, Muneer Rizvydeen, Michael Steinert, Christina Suh, Haein Sung, Asantewaa Ture, and Gabriela Velazquez for their assistance with data collection and analysis.
Footnotes
A commentary on this article appears in this issue on page 849.
REFERENCES
- 1.Lewy AJ, Cutler NL, Sack RL. The endogenous melatonin profile as a marker of circadian phase position. J Biol Rhythms. 1999;14:227–36. doi: 10.1177/074873099129000641. [DOI] [PubMed] [Google Scholar]
- 2.Klerman EB, Gershengorn HB, Duffy JF, Kronauer RE. Comparisons of the variability of three markers of the human circadian pacemaker. J Biol Rhythms. 2002;17:181–93. doi: 10.1177/074873002129002474. [DOI] [PubMed] [Google Scholar]
- 3.Burgess HJ, Fogg LF. Individual differences in the amount and timing of salivary melatonin secretion. PLoS One. 2008;3:e3055. doi: 10.1371/journal.pone.0003055. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Lewy AJ, Wehr TA, Goodwin FK, Newsome DA, Markey SP. Light suppresses melatonin secretion in humans. Science. 1980;210:1267–9. doi: 10.1126/science.7434030. [DOI] [PubMed] [Google Scholar]
- 5.American Academy of Sleep Medicine. The International Classification of Sleep Disorders. 3rd Edition. Darien, IL: American Academy of Sleep Medicine; 2014. [Google Scholar]
- 6.Lockley SW. Timed melatonin treatment for delayed sleep phase syndrome: the importance of knowing circadian phase. Sleep. 2005;28:1214–6. doi: 10.1093/sleep/28.10.1214. [DOI] [PubMed] [Google Scholar]
- 7.Keijzer H, Smits MG, Duffy JF, Curfs LM. Why the dim light melatonin onset (DLMO) should be measured before treatment of patients with circadian rhythm sleep disorders. Sleep Med Rev. 2014;18:333–9. doi: 10.1016/j.smrv.2013.12.001. [DOI] [PubMed] [Google Scholar]
- 8.Strollo PJ, Jr., Badr MS, Coppola MP, Fleishman SA, Jacobowitz O, Kushida CA. The future of sleep medicine. Sleep. 2011;34:1613–9. doi: 10.5665/sleep.1410. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Bjorvatn B, Pallesen S. A practical approach to circadian rhythm sleep disorders. Sleep Med Rev. 2009;13:47–60. doi: 10.1016/j.smrv.2008.04.009. [DOI] [PubMed] [Google Scholar]
- 10.Lewy AJ, Lefler BJ, Emens JS, Bauer VK. The circadian basis of winter depression. Proc Natl Acad Sci U S A. 2006;103:7414–9. doi: 10.1073/pnas.0602425103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Benloucif S, Burgess HJ, Klerman EB, et al. Measuring melatonin in humans. J Clin Sleep Med. 2008;4:66–9. [PMC free article] [PubMed] [Google Scholar]
- 12.Pullman RE, Roepke SE, Duffy JF. Laboratory validation of an in-home method for assessing circadian phase using dim light melatonin onset (DLMO) Sleep Med. 2012;13:703–6. doi: 10.1016/j.sleep.2011.11.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Kudielka BM, Broderick JE, Kirschbaum C. Compliance with saliva sampling protocols: electronic monitoring reveals invalid cortisol daytime profiles in noncompliant subjects. Psychosom Med. 2003;65:313–9. doi: 10.1097/01.psy.0000058374.50240.bf. [DOI] [PubMed] [Google Scholar]
- 14.Keijzer H, Smits MG, Peeters T, Looman CW, Endenburg SC, Gunnewiek JM. Evaluation of salivary melatonin measurements for Dim Light Melatonin Onset calculations in patients with possible sleep-wake rhythm disorders. Clin Chim Acta. 2011;412:1616–20. doi: 10.1016/j.cca.2011.05.014. [DOI] [PubMed] [Google Scholar]
- 15.Tasto DL, Colligan MJ, Skjei EW, Polly SJ. Health consequences of shift work. Cincinnati, OH: NIOSH Publication #78-154; 1978. [Google Scholar]
- 16.Butcher JN, Dahlstrom WG, Graham JR, Tellegen A, Kaemmer B. Minneapolis, MN: University of Minnesota Press; 1989. MMPI-2 (Minnesota Multiphasic Personality Inventory-2): manual for administration and scoring. [Google Scholar]
- 17.Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An inventory for measuring depression. Arch General Psychiatry. 1961;4:53–63. doi: 10.1001/archpsyc.1961.01710120031004. [DOI] [PubMed] [Google Scholar]
- 18.Terman M, Williams J. Personal inventory for depression and SAD (PIDS) J Prac Psychiatry Behav Health. 1998;5:301–3. [Google Scholar]
- 19.Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh sleep quality index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28:193–213. doi: 10.1016/0165-1781(89)90047-4. [DOI] [PubMed] [Google Scholar]
- 20.Bastien CH, Vallieres A, Morin CM. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med. 2001;2:297–307. doi: 10.1016/s1389-9457(00)00065-4. [DOI] [PubMed] [Google Scholar]
- 21.Netzer NC, Stoohs RA, Netzer CM, Clark K, Strohl KP. Using the Berlin Questionnaire to identify patients at risk for the sleep apnea syndrome. Ann Intern Med. 1999;131:485–91. doi: 10.7326/0003-4819-131-7-199910050-00002. [DOI] [PubMed] [Google Scholar]
- 22.Allen RP, Picchietti DL, Garcia-Borreguero D, et al. Restless legs syndrome/Willis-Ekbom disease diagnostic criteria: updated International Restless Legs Syndrome Study Group (IRLSSG) consensus criteria - history, rationale, description, and significance. Sleep Med. 2014;15:860–73. doi: 10.1016/j.sleep.2014.03.025. [DOI] [PubMed] [Google Scholar]
- 23.Horne JA, Ostberg O. A self-assessment questionnaire to determine morningness-eveningness in human circadian rhythms. Int J Chronobiol. 1976;4:97–110. [PubMed] [Google Scholar]
- 24.Murphy PJ, Myers BL, Badia P. Nonsteroidal anti-inflammatory drugs alter body temperature and suppress melatonin in humans. Physiol Behav. 1996;59:133–9. doi: 10.1016/0031-9384(95)02036-5. [DOI] [PubMed] [Google Scholar]
- 25.Burgess HJ. Evening ambient light exposure can reduce circadian phase advances to morning light independent of sleep deprivation. J Sleep Res. 2013;22:83–8. doi: 10.1111/j.1365-2869.2012.01042.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Zeitzer JM, Dijk DJ, Kronauer RE, Brown EN, Czeisler CA. Sensitivity of the human circadian pacemaker to nocturnal light: melatonin phase resetting and suppression. J Physiol. 2000;526.3:695–702. doi: 10.1111/j.1469-7793.2000.00695.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Voultsios A, Kennaway DJ, Dawson D. Salivary melatonin as a circadian phase marker: validation and comparison to plasma melatonin. J Biol Rhythms. 1997;12:457–66. doi: 10.1177/074873049701200507. [DOI] [PubMed] [Google Scholar]
- 28.Molina TA, Burgess HJ. Calculating the dim light melatonin onset: the impact of threshold and sampling rate. Chronobiol Int. 2011;28:714–8. doi: 10.3109/07420528.2011.597531. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Chang AM, Santhi N, St Hilaire MA, et al. Human responses to bright light of different durations. J Physiol. 2012;590:3103–12. doi: 10.1113/jphysiol.2011.226555. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Benloucif S, Guico MJ, Reid KJ, Wolfe LF, L'Hermite-Baleriaux M, Zee PC. Stability of melatonin and temperature as circadian phase markers and their relation to sleep times in humans. J Biol Rhythms. 2005;20:178–88. doi: 10.1177/0748730404273983. [DOI] [PubMed] [Google Scholar]
- 31.Wyatt JK, Stepanski EJ, Kirkby J. Circadian phase in delayed sleep phase syndrome: predictors and temporal stability across multiple assessments. Sleep. 2006;29:1075–80. doi: 10.1093/sleep/29.8.1075. [DOI] [PubMed] [Google Scholar]
- 32.Burgess HJ, Eastman CI. Early versus late bedtimes phase shift the human dim light melatonin rhythm despite a fixed morning lights on time. Neurosci Lett. 2004;356:115–8. doi: 10.1016/j.neulet.2003.11.032. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Burgess HJ, Eastman CI. A late wake time phase delays the human dim light melatonin rhythm. Neurosci Lett. 2006;395:191–5. doi: 10.1016/j.neulet.2005.10.082. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Buxton OM, L'Hermite-Baleriaux M, Turek FW, Van Cauter E. Daytime naps in darkness phase shift the human circadian rhythms of melatonin and thyrotropin secretion. Am J Physiol. 2000;278:R373–82. doi: 10.1152/ajpregu.2000.278.2.R373. [DOI] [PubMed] [Google Scholar]
- 35.Sasseville A, Paquet N, Sevigny J, Hebert M. Blue blocker glasses impede the capacity of bright light to suppress melatonin production. J Pineal Res. 2006;41:73–8. doi: 10.1111/j.1600-079X.2006.00332.x. [DOI] [PubMed] [Google Scholar]
- 36.Kayumov L, Casper RF, Hawa RJ, et al. Blocking low-wavelength light prevents nocturnal melatonin suppression with no adverse effect on performance during simulated shift work. J Clin Endocrinol Metab. 2005;90:2755–61. doi: 10.1210/jc.2004-2062. [DOI] [PubMed] [Google Scholar]
- 37.Burgess HJ, Molina TA. Home lighting before usual bedtime impacts circadian timing: a field study. Photochem Photobiol. 2014;90:723–6. doi: 10.1111/php.12241. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Rahman SA, Kayumov L, Tchmoutina EA, Shapiro CM. Clinical efficacy of dim light melatonin onset testing in diagnosing delayed sleep phase syndrome. Sleep Med. 2009;10:549–55. doi: 10.1016/j.sleep.2008.03.020. [DOI] [PubMed] [Google Scholar]