

Abstract
Study Objectives:
Coregulation of biological systems is a defining feature of normative attachment in close adult relationships. Sleep is a shared, intimate biological process between couples; however, sleep is usually examined at the individual level. We examined minute-by-minute concordance in couples' actigraphy-defined sleep-wake patterns, and how attachment style and marital satisfaction relate to concordance.
Design:
Couples completed measures of avoidant and anxious attachment styles and relationship functioning and wore wrist actigraphs for 10 days. Minute-by-minute concordance of sleep and wake (i.e., the percentage of epochs in which both partners were asleep, or both were awake) was calculated for each sleep period. Mixed modeling was used to account for measurement occasions across time.
Results:
Percent concordance ranged from 53–88% and was not associated with couples' sleep quality or circadian preference. For wives, neither anxious nor avoidant attachment was associated with sleep-wake concordance. For husbands, anxious attachment style was associated with higher concordance, but was moderated by wives' marital satisfaction. High marital satisfaction in wives was associated with higher concordance, regardless of husbands' attachment style. In couples in which wives reported low satisfaction, concordance was higher when husbands had an anxious attachment style. Avoidant attachment style in husbands was not related to concordance.
Conclusions:
Sleep concordance provides a unique measure of couples' cosleep and varies depending on attachment style and relationship satisfaction.
Citation:
Gunn HE, Buysse DJ, Hasler BP, Begley A, Troxel WM. Sleep concordance in couples is associated with relationship characteristics. SLEEP 2015;38(6):933–939.
Keywords: couples, relationships, concordance, attachment, marital satisfaction
INTRODUCTION
Sleep and sleep behaviors are associated with long-term health outcomes such as cardiovascular disease and diabetes.1–6 Close relationships are also strongly linked to physical and psychological health outcomes through factors such as relationship characteristics, physiological processes, and shared health behaviors.7–11 Although sleep is most often examined at the individual level, it can also be described at the level of the dyad.12–15 Couples' sleep patterns are likely interdependent16 because of similar sleep-timing behaviors and movement patterns associated with the physical presence of another person in the bed.12,13 Therefore, examining sleep at the level of the couple may improve our understanding of the mechanisms by which both sleep and relationships lead to long-term health outcomes.17 Furthermore, relationship characteristics such as relationship security (i.e., attachment style) and marital satisfaction have been shown to influence sleep at the individual level,18–20 and should be considered when examining sleep in a dyadic context.
Couples' sleep behavior is an example of coregulation, i.e., a reciprocally maintained physiological process that serves to maintain psychological and biological homeostasis of individuals in a relationship.8 One way to measure coregulation is to examine the degree of synchrony, or concordance, of physiological processes between individuals across multiple time points. For example couples' cortisol levels are concordant across several time points over several days.21 Concordance in couples' cortisol levels is influenced by couples' ratings of marital satisfaction; less satisfied couples had stronger concordance in cortisol levels.21
Concordance in sleep can be indexed by synchrony in overall sleep behaviors, such as bed and wake times. One study showed that on the one hand, less well-adjusted couples have more conflict in their relationship22 and are less concordant in their self-reported, preferred bed and wake times than better-adjusted couples. On the other hand, well-adjusted couples who were mismatched in their preferred bed and wake times show more flexible and adaptable problem-solving skills compared to well-adjusted couples who are concordant for bed and wake times.23 Hasler and Troxel14 found that discordant bedtimes in couples, assessed by actigraphy, predict negative partner interactions the following day.
Sleep-wake concordance can also be measured by objective assessments of sleep across the night using actigraphy or polysomnography. Pankhurst and Horne14 examined couples' sleep and found concordance in epoch-by-epoch, actigraphy-assessed movement patterns, which suggests that couples have similar sleep-wake patterns throughout the night. However, this study did not examine the degree to which relationship characteristics influence concordance.
Thus, previous research has linked concordance/discordance in overall sleep timing to relationship factors,14 and has suggested that couples have concordant sleep based on movement patterns.12 To our knowledge, previous studies have not examined the association between relationship characteristics and fine-grained, minute-by-minute assessment of couples' sleep-wake concordance throughout the night.
The current study used wrist actigraphy to measure concordance in couples' minute-by-minute sleep throughout the night, and assessed whether attachment style and relationship factors are associated with concordance. We had three main aims. First, we examined sleep-wake concordance within couples, and examined whether concordance was related to self-report measures of sleep quality and circadian function. We compared couples' concordance to statistically randomly-matched individuals to control for the fact that most individuals in the population sleep within the same time frame (i.e., 22:00–08:00). Second, we tested whether attachment style was associated with concordance of objective sleep. Attachment style has been associated with individuals' sleep,19,20,24 and may also be linked to coregulation of physiology in couples.8 We expected that securely attached individuals would have higher sleep-wake concordance than individuals with less attachment security. Third, relationships may adjust to accommodate individual characteristics, such as attachment style and sleep preferences22; therefore, we examined the extent to which global marital satisfaction moderated significant associations between attachment style and sleep-wake concordance.
METHOD
Participants and Procedure
The University of Pittsburgh Biomedical Institutional Review Board approved this study. The current examination is part of a larger study focused on the dynamic association between sleep and relationship quality in married couples, and the influence of these factors on cardiovascular biomarkers (HL093220). Healthy, married couples between the ages of 18–45 y were recruited from the community, primarily using flyers and newspaper advertisements. The age range was selected to minimize the likelihood of clinically manifest cardiovascular disease or use of medications (including hypertensive medication) that could affect cardiovascular function, as well as changes in sleep associated with aging and menopause. Participants in the current analysis were 48 heterosexual, married couples who regularly shared a bed with their spouse (at least 4 nights a week). After written informed consent, participants completed an in-person diagnostic evaluation and an in-home overnight screening night for sleep disordered breathing. Exclusionary criteria included having a current sleep disorder, pregnancy, current psychiatric illness, substance dependence, cardiovascular or renal disease, diabetes, or use of prescription medications known to affect the autonomic nervous system. Each member of the eligible couples completed questionnaires about their relationship and sleep, and each wore a wrist acti-graph for 10 days.
Relationship Measures
Attachment style
Trait-level adult attachment can be characterized within a two-dimensional structure representing anxious and avoidant attachment styles. Attachment anxiety is characterized by fears of abandonment and preoccupation with physical and emotional availability of the other person.25,26 Avoidant attachment is characterized by a tendency to value autonomy and suppress needs for closeness. To measure anxious and avoidant attachment, participants completed the Experiences in Close Relationships (ECR) inventory,26–28 a 36-item measure with 18 items that assess avoidance (“I prefer not to be too close to my romantic partners”) and 18 items that assess anxiety (“I'm afraid I will lose my partner's love”). Each item is rated on a seven-point scale where 1 = strongly disagree and 7 = strongly agree. Items within attachment anxiety and attachment avoidance are each averaged to yield a continuous seven-point rating for attachment anxiety and avoidance. This scale has good temporal stability, reliably distinguishes between anxious and avoidant attachment and has good internal reliability.29 In the current sample, the avoidant and anxious scales were both internally reliable (α = 0.87, α = 0.86, respectively).
Marital Satisfaction
Marital satisfaction was assessed using the Dyadic Satisfaction subscale of the Dyadic Adjustment Scale,30 which is one of the most widely used and well-validated measures in the relationship literature. The scale assesses each member's assessment of the couples' relationship satisfaction. Specific items, such as agreement on important matters in the relationship and degree of affection, are rated on a Likert scale. Scores on Dyadic Satisfaction subscale range from 20 (low satisfaction) to 77 (high satisfaction). The Satisfaction subscale has been shown to be internally consistent.30 The Satisfaction subscale had good internal reliability in our sample (α = 0.83).
Sleep Measures
Actigraphy
Each member of the couple was instructed to wear a wrist actigraph continuously for 10 days. Participants wore the Actiwatch 64 model (Philips Respironics). One couple wore the Actiwatch II model by Philips Respironics; however, the same software and algorithm was used for both types of watches (described later). Actiwatches include accelerometers that record movement. Sleep is determined by the presence or absence of movement at predefined epoch lengths. Epoch lengths in this study were 60 sec. Individuals pushed an event marker on the actigraph when they got into bed and attempted to go to sleep and when they got out of bed and were no longer attempting to sleep. These markers define the rest interval, that is, the total amount of time an individual is intending to sleep. If the participant did not press the event marker for a given night (< 1% of the time), we used his/her diary record to determine their bedtime and wake time to calculate their rest interval.
Sleep was determined for each 60-sec epoch using a scoring algorithm developed by Philips Respironics, Bend, OR. Briefly, depending on the amount of movement, an epoch is scored as wake or sleep. For this article, we used the standard scoring algorithm such that the threshold of movement counts was set at “medium” sensitivity of 40. Actiwatches for the couple were initialized on the same computer within a few minutes of each other. They were also programmed to start and stop collecting data at the same time.
Sleep-wake concordance, the dependent variable in the current analyses and measure of coregulation, refers to whether couples are asleep or awake at the same time. To establish a value for sleep-wake concordance, we first calculated a dyadic rest interval, the total amount of time at least one member of the couple is intending to sleep, for each night the couples wore the Actiwatches. For example, if one member of the couple went to bed, intending to sleep, at 22:30, but the other member did not go to bed until 23:30, the beginning of the rest interval would be 22:30 PM. Similarly, if one member of the couple gets out of bed at 07:00 and the other member does not get out of bed until 08:00, the end of the rest interval would be 08:00. Therefore, the dyadic rest interval refers to the earliest bedtime and the latest wake time for the dyad. This method was chosen to capture the broadest range of couples' sleep and sleep behaviors.
Next, we determined whether the couple was awake or asleep at the same time for each 60-sec epoch throughout each dyadic rest interval. Each epoch for each individual was coded as wake or sleep. We assigned binary values (1 or 0) to represent whether the couple was awake or asleep together within the same epoch (i.e., concordant) or whether one member of the couple was awake and the other member was asleep (i.e., discordant). For example, if the dyadic rest interval was 8.5 h, or 510 epochs, there would be 510 values for that rest interval. On average, the dyadic rest interval was 527 epochs per night, or 8 h, 45 min.
We computed a sleep-wake concordance percentage score by dividing the number of epochs concordant for sleep and wake by the number of total epochs [(#concordant epochs/#total epochs)*100]. Therefore, a value of 85% means that the couple was concordant for sleep and wake in 85% of epochs within the dyadic rest interval.
Sleep Questionnaires
Participants were given questionnaires to measure their circadian preference and self-reported sleep quality. Participants completed these measures before conducting the 10-day portion of the study. Circadian preference was assessed using the Composite Scale of Morningness,31 a 13-item measure that assesses the degree of morningness using a five-point Likert response scale. Participants are asked to rate their timing preference for a range of activities (e.g., wake time, bedtime) and how they feel at certain times during the day. Specific items include “How alert do you feel during the first half hour after awakened in the morning?” and “At what time in the evening do you feel tired and, as a result in need of sleep?” Response scores range from 1 to 5; the measurement scores range from 13 (extreme eveningness) to 55 (extreme morningness). The Morningness Scale has demonstrated good reliability and validity.31 Sleep quality was assessed with the Pittsburgh Sleep Quality Index (PSQI).32 This measure assesses sleep complaints during the previous month. The scale is comprised of 18 items and yields a global PSQI score, ranging from 0 – 21, with higher scores indicating poorer sleep quality. The PSQI is a valid assessment of sleep quality, reliably discriminates between good and poor sleepers, and has good internal and test-retest reliability.32,33
Data Analytic Plan
Descriptives
All data were checked for normality and transformations were performed as necessary. We conducted Pearson correlations to examine mean-level associations among sleep and relationship variables. Correlations were computed separately for men and women due to nesting within couples.
Because most people sleep at night in general, we examined whether “true” couples had higher levels of concordance than unrelated randomly paired males and females. We used individuals within our sample to obtain a bootstrap distribution. That is, individuals in the original sample served as a population reservoir to create a pseudo (bootstrap) sample of 50,000 random pairings of males and females. This was done by randomly sampling observations with replacement using SAS, version 9.3 (PROC SURVEYSELECT, SAS Institute Inc., Cary, NC). True couples were not included in bootstrap distribution. Concordance of the randomly paired individuals was computed matching on day of the week. This analysis yielded estimated confidence intervals of sleep-wake concordance of randomly paired males and females to compare to the true couples sleep-wake concordance.
Sleep-wake concordance is a between-dyad outcome variable. Each couple had one concordance value per night over the 10-day period (i.e., 10 values per couple) Therefore, we conducted mixed modeling to account for measurement occasions across time for percent sleep-wake concordance (SASPROC MIXED) using SAS/STAT® software. To determine whether anxious and avoidant attachment styles were associated with sleep-wake concordance, we conducted four separate statistical tests with scores for anxious and avoidant attachment examined separately for husbands and wives. Thus, each model had one person-level predictor (attachment) and a repeated time-level variable for nightly concordance. If scores on the anxious and avoidant attachment measures were significantly associated with sleep-wake concordance for either husband or wife, we then tested, in separate models, the moderating effect of husband and wife marital satisfaction scores. Moderation was examined using a hierarchical approach whereby the cross-product effects of attachment and marital satisfaction (attachment × marital satisfaction) are examined above and beyond the individual contributions of attachment and marital satisfaction.34 Predictors and interaction terms were centered. Length of marriage (categorical variable) and whether or not the couple had children (dichotomous variable) were selected a priori as covariates in all statistical models. Whether or not the couple had children was chosen as a variable because of prior evidence that parenthood is associated with relationship satisfaction35 and that parent sleep quantity and quality is influenced by children.36 Length of marriage was included to account for potential differences in concordance as a function of changes in couple-level sleep habits over time.
Case-wise diagnostics were conducted and revealed one multivariate outlier (low concordance and low avoidant attachment) in the analysis of wife avoidant attachment and concordance. This case was removed from the analysis.
RESULTS
Couple and Individual Sample Characteristics
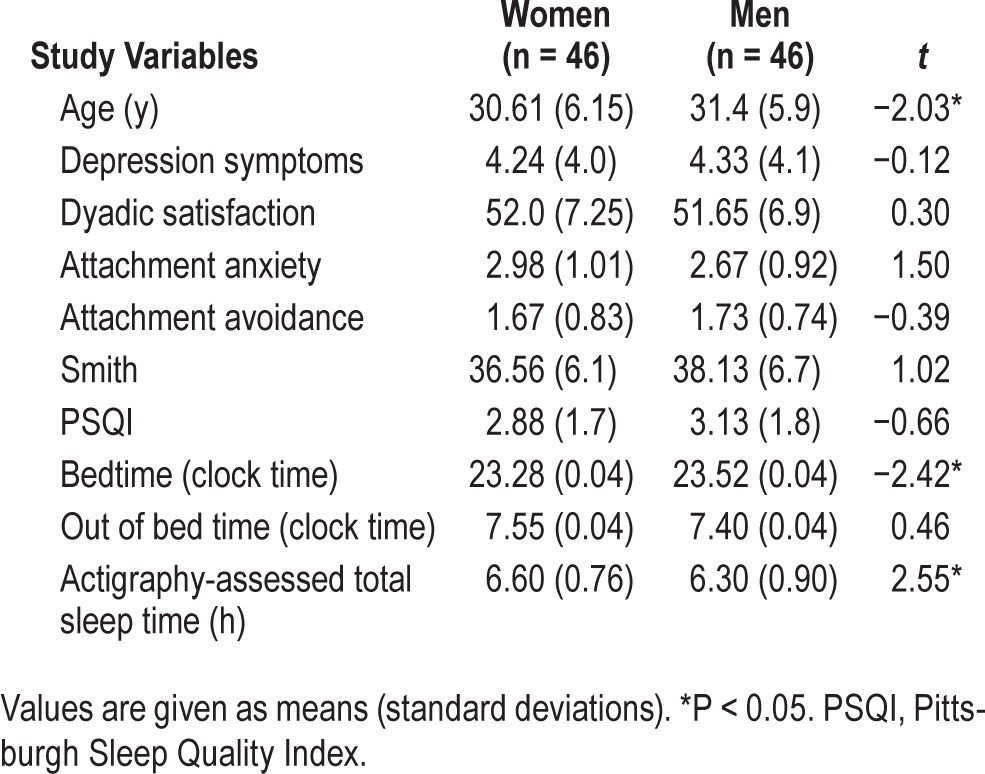
About half (45%) of the couples were married 1–4 y; 21% were married < 1 y; 17% were married 5–10 y, 4% were married 11–14 y, and 10% were married > 15 y. Most couples (64%) did not have children living at home. The remaining couples had between one and four children (mean = 2.13). Length of marriage and having children in the home were not significantly correlated with predictor or outcome variables. These covariates were retained in all statistical models to account for their variance in the association between relationship factors and sleep-wake concordance. However, the associations reported below do not change when excluding covariates. Mean differences between husbands and wives on all other study variables are presented in Table 1. Husbands and wives were significantly different on three study variables: Husbands were about 1 y older than wives; wives went to bed, on average, 15 min before husbands; and wives slept an average of 20 min longer than husbands (6 h, 40 min per night versus 6 h, 20 min, respectively).
Table 1.
Means, standard deviations, and paired t-tests of descriptive and study variables.
Are Couples More Concordant Than Randomly Paired Individuals?
An illustrative example of one true couples' and one randomly paired couples' actigraphy is presented in Figure 1. Concordance for each couple, as it was calculated in the current study (concordant versus not concordant), is depicted in Figures 1C and 1F. Figure 2 demonstrates that couples' concordance was higher than the bootstrapped sample of randomly matched individuals. Mean concordance for the true couples was 75% versus 59% for the bootstrap sample. The 95% confidence intervals of the true couples (60–85%) and randomly paired individuals (45–70%) overlap. However, mean concordance for the “true” couples (75%) falls outside the 95th percentile for the bootstrapped sample.
Figure 1.

Actigrams for each partner of a true (A,B) and randomly paired (D,E) couple for one night using the dyadic rest interval. Binary illustration of concordance presented below actigrams (C,F). Panels C and F represent 89% and 75% sleep-wake concordance, respectively. The gray, upper lines illustrate when the couple is concordant for wake or sleep. The black, lower lines illustrate when the couple is discordant.
Figure 2.
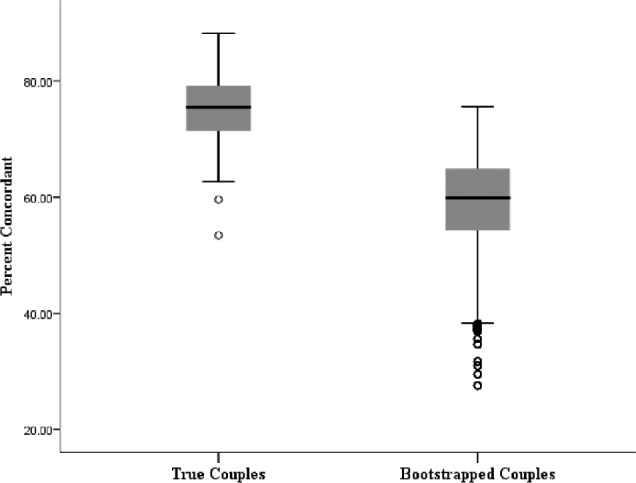
Box and whisker plot of true couples versus bootstrapped couples. T-bars represent 5th and 95th confidence intervals. The center black line in each box represents the mean.
Bivariate Correlations
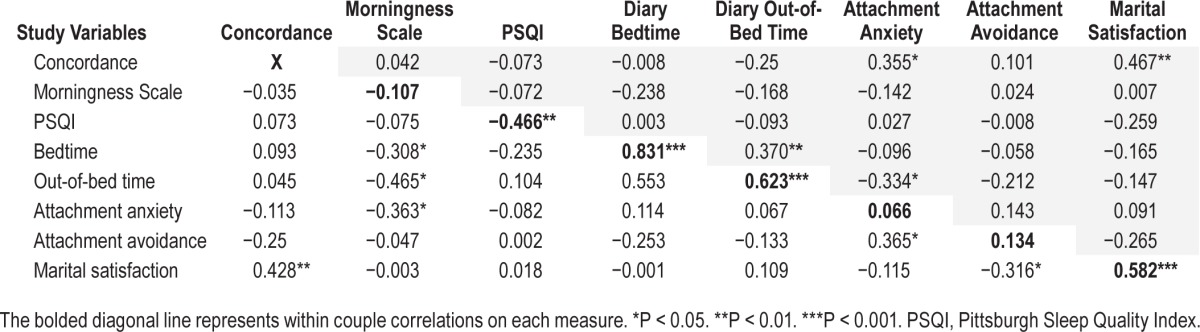
Zero-order bivariate correlations among sleep variables for husbands (shaded and displayed above the diagonal) and for wives (displayed below the diagonal) are presented in Table 2. Within-dyad correlations are displayed along the bolded diagonal line. Within couples, PSQI scores were negatively correlated, whereas into-bed times and out-of-bed times were positively correlated. In other words, husbands and wives tended to get in and out of bed at the same times. Husbands' and wives' attachment styles were not significantly correlated. Marital satisfaction between partners was positively correlated. There were no other significant correlations within couples. Higher marital satisfaction in both partners was associated with higher sleep-wake concordance, but higher attachment anxiety was associated with higher sleep-wake concordance in husbands only. Concordance was the only sleep related variable associated with attachment style and marital satisfaction. For wives, scores on the Morningness Scale and into-bed and out-of-bed times were significantly correlated; morningness was associated with earlier bedtimes and eveningness was associated with later bedtimes. The associations between Morningness scores and into-bed and out-of-bed times were not significant for husbands. Concordance was not significantly associated with other sleep variables for husbands or wives.
Table 2.
Bivariate intercorrelations for sleep measures (concordance, morningness scale, Pittsburgh Sleep Quality Index) and relationship measures (attachment anxiety, attachment avoidance, and marital satisfaction). Values for husbands are shaded and displayed above the diagonal and values for wives are displayed below the diagonal.
Attachment Style and Sleep-Wake Concordance
Wives
Avoidant attachment in wives was not significantly associated with concordance, B = −10.74, standard error [SE] = 5.98, t(39) = −1.80, P = 0.080. Anxious attachment style for wives was also not associated with sleep-wake concordance, B = −1.00, SE = 1.16 t(40) −0.86, P = 0.40.
Husbands
For husbands, avoidant attachment was not related to sleep-wake concordance, B = 1.06, SE = 1.55, t(40) = 0.69, P = 0.49. However, anxious attachment style was associated with higher concordance, B = 2.96, SE = 1.21 t(40) = 2.37, P = 0.019.
Marital Satisfaction as a Moderator of Attachment Style and Sleep-Wake Concordance
Given the significant association between husbands' anxious attachment style and concordance, we tested whether marital satisfaction moderated this association. The association between anxious attachment style in husbands was moderated by wives' marital satisfaction scores, B = −0.335, SE = 0.139 t(38) = −2.42, P = 0.021 (Figure 3). When wives reported higher marital high satisfaction, there was no effect of husband's anxious attachment on sleep-wake concordance. However, when wives reported lower marital satisfaction, anxious attachment style in husbands was associated with higher sleep-wake concordance. In contrast, although husbands and wives' marital satisfaction scores were correlated, husbands' report of marital satisfaction did not moderate the association between his anxious attachment score and sleep-wake concordance, B = −0.126, SE = 0.127 t(38) = −1.00, P = 0.32.
Figure 3.
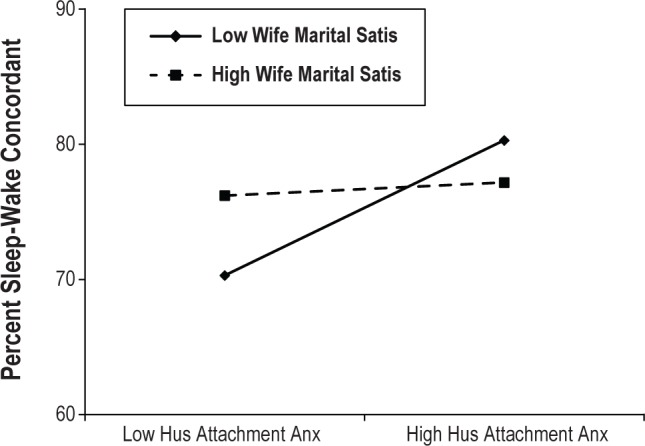
Interaction between husband attachment anxiety by wife marital satisfaction on sleep-wake concordance based on mixed model controlling for covariates. Values are plotted at one standard deviation above and below the mean. Values for low and high husband attachment anxiety are 1.73 and 3.60, respectively. Values for low and high wife marital satisfaction are 44.75 and 59.25, respectively. Percent sleep-wake concordance values account for night-to-night variation in concordance.
Follow-up Analyses
The aforementioned findings suggest that sleep-wake concordance using the dyadic rest interval is associated with husband's attachment anxiety, and the association between husband's attachment anxiety and sleep-wake concordance is moderated by the wife's marital satisfaction scores. It is possible that differing in- and out-of-bed times could explain some of the variation in sleep-wake concordance and its association with relationship variables.14 Therefore, we repeated the aforementioned analyses to determine whether attachment style and marital satisfaction were associated with sleep-wake concordance, restricted to the time interval when both members of the couple are in bed and trying to sleep.
The number of epochs per night in which to calculate concordance was reduced (440 epochs versus 527 epochs in the dyadic rest interval), and led to higher average sleep-wake concordance (82% versus 74.9% for the dyadic rest interval). The main effects and interaction described above were in the same direction and still significant at the 0.05 level. No new associations emerged.
DISCUSSION
Compared to randomly matched dyads, couples had higher concordance in sleep-wake patterns throughout the night. Attachment style was related to sleep-wake concordance; specifically, couples had higher concordance when husbands endorsed an anxious attachment style, but only for couples in which the wife endorsed low marital satisfaction.
The findings on couples' concordance are a novel contribution to the couples and sleep literature and are consistent with previous findings on concordance in movement by Pankhurst and Horne.12 The higher degree of concordance among couples compared to randomly paired individuals would suggest that sleep may be one type of biological coregulation that occurs within close, roman tic relationships.8 Sleep-wake concordance was not associated with husbands' or wives' morningness or eveningness preference or self-reported sleep quality. This suggests that concordance in objectively measured sleep is a unique assessment of couples' co-sleep that does not appear to be explained by sleep quality or circadian preference.
Consistent with the e merging literature,14 our findings on attachment, satisfaction, and concordance support the general notion that sleep is associated with couples' relationship factors. Similar to previous studies, we found that an anxious attachment style was associated with sleep-wake patterns.19,20,24
Whereas previous studies have found that attachment anxiety was associated with poor sleep quality and reduced quantity of restorative sleep, we found that attachment anxiety in husbands was associated with higher concordance in couples' sleep-wake patterns. This finding was somewhat unexpected because women had higher mean attachment anxiety scores than men (though not significantly different), which is consistent wi th previous research.37 It is possible that husbands who are anxious about the relationship influence bedtime behaviors, including time in bed, especially given that attachment anxiety is characterized by heightened need for closeness. However, this finding was moderated by the wives' level of relationship satisfaction, such that when wives reported higher marital satisfaction there was no effect of husbands' anxious attachment style. Therefore, in addition to considering how an individual's attachment style is associated with sleep, it may also be important to consider contextual factors, such as the level of satisfaction of each member of the couple.
Both husbands' and wives' marital satisfaction were positively correlated with concordance. However, wives', but not husbands', marital satisfaction moderated the association between husbands' anxious attachment and concordance. This is somewhat consistent with previous findi ngs. Hasler and Troxel14 found that concordance in sleep timing (bedtimes and wake times) was associated with positive or negative marital interactions, but only for women. Our finding suggests that wives' ratings of marital satisfaction may be more closely connected to concordance than husbands' ratings. Of note is that previous studies of marital satisfaction and other physiological outcomes, such as blood pressure reactivity, have found that wives' physiological responses are more closely linked to marital satisfaction, possibly because women are more attuned to the emotional q uality of the marriage.7
This study has a number of strengths, including an objective measure of sleep and multiple data points (i.e., 10 days of actigraphy). In addition, to our knowledge, it is the first examination of relationship factors and minute-by-minute concordance in couples' sleep. This approach allowed for an objective assessment of sleep that may approximate coregulation in sleep throughout the night. However, it is important to note that actigraphy has been shown to overestimate sleep by categorizing quiet, non-moving wakefulness as sleep.38 In future studies, it will be useful to explore coregulation using polysomnography (PSG) for an even more detailed physiological assessment of couples' sleep. Home PSG assessments will be particularly useful for assessing coregulation of sleep in the couples' environment. The couples in this study were healthy, tended to sleep well, and were generally satisfied in their relationship. Therefore, there was a limited range in the assessment of marital satisfaction and attachment. The current sample was also limited to heterosexual, married couples given the aims of the overall study, and that there are known biological sex differences in sleep and cardiovascular biomarkers. Future studies would benefit from also including culturally diverse couples with varying attachment styles and sleep problems to increase precision and understanding of these associations.
CONCLUSIONS
Limitations notwithstanding, the minute-by-minute approach to couples sleep used in this study provided a finer grained analysis of couples' nighttime sleep behaviors than comparisons between individually-assessed global sleep-wake characteristics. Findings from the current study and from a handful of previous studies on couples' sleep12,14 provide growing evidence for concordance in sleep-wake and movement patterns and in sleep behaviors, such as bedtimes and wake times. Our findings also suggest that couples' sleep may be a coregulated process and that dynamic relationship factors influence the degree of coregulation. Specifically, attachment style is associated with coregulation but varies depending on relationship satisfaction. Coregulation of physiological processes, including sleep, may be one pathway linking romantic relationships to health outcomes.8 To that end, an important next step in this line of research will be to test the influence of sleep-wake concordance on health outcomes. Moreover, as evidence that sleep is a shared process becomes more prominent, it will be important to expand how we assess an individual's sleep to include children or other family members who may influence an individual's sleep, and influence mechanisms by which relationships influence the sleep-health connection.
DISCLOSURE STATEMENT
This study was funded by National Heart Lung and Blood Institute K23HL093220 (PI: Wendy M. Troxel). Support for Dr. Gunn was provided by National Institute of Health T32 HL082610 (PI: Daniel J. Buysse). Dr Buysse has served as a paid consultant on scientific advisory boards for Merck, Otsuka, Eisai, CME Outfitters, and Medscape. The other authors have indicated no financial conflicts of interest.
ACKNOWLEDGMENTS
The authors wish to thank Mary Fletcher and Jean Miewald for their assistance with data management.
REFERENCES
- 1.Cappuccio FP, Stranges S, Kandala NB, et al. Gender-specific associations of short sleep duration with prevalent and incident hypertension: the Whitehall II Study. Hypertension. 2007;50:693–700. doi: 10.1161/HYPERTENSIONAHA.107.095471. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Gottlieb DJ, Redline S, Nieto FJ, et al. Association of usual sleep duration with hypertension: the Sleep Heart Health Study. Sleep. 2006;29:1009–14. doi: 10.1093/sleep/29.8.1009. [DOI] [PubMed] [Google Scholar]
- 3.Gangwisch JE, Heymsfield SB, Boden-Albala B, et al. Short sleep duration as a risk factor for hypertension: analyses of the first National Health and Nutrition Examination Survey. Hypertension. 2006;47:833–9. doi: 10.1161/01.HYP.0000217362.34748.e0. [DOI] [PubMed] [Google Scholar]
- 4.Quan SF. Sleep disturbances and their relationship to cardiovascular disease. Am J Lifestyle Med. 2009;3:55s–9s. doi: 10.1177/1559827609331709. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Ayas NT, White DP, Manson JE, et al. A prospective study of sleep duration and coronary heart disease in women. Arch Intern Med. 2003;163:205–9. doi: 10.1001/archinte.163.2.205. [DOI] [PubMed] [Google Scholar]
- 6.Ayas NT, White DP, Al-Delaimy WK, et al. A prospective study of self-reported sleep duration and incident diabetes in women. Diabetes Care. 2003;26:380–4. doi: 10.2337/diacare.26.2.380. [DOI] [PubMed] [Google Scholar]
- 7.Kiecolt-Glaser JK, Newton TL. Marriage and health: his and hers. Psychol Bull. 2001;127:472–503. doi: 10.1037/0033-2909.127.4.472. [DOI] [PubMed] [Google Scholar]
- 8.Sbarra DA, Hazan C. Coregulation, dysregulation, self-regulation: an integrative analysis and empirical agenda for understanding adult attachment, separation, loss, and recovery. Pers Soc Psychol Rev. 2008;12:141–67. doi: 10.1177/1088868308315702. [DOI] [PubMed] [Google Scholar]
- 9.Butler EA, Randall AK. Emotional coregulation in close relationships. Emotion Review. 2013;5:202–10. [Google Scholar]
- 10.Pietromonaco PR, Uchino BNDSC. Close relationship processes and health: implications for attachment theory for health and disease. Health Psychol. 2014;32:499–513. doi: 10.1037/a0029349. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Meyler D, Stimpson JP, Peek MK. Health concordance within couples: a systematic review. Soc Sci Med. 2007;64:2297–310. doi: 10.1016/j.socscimed.2007.02.007. [DOI] [PubMed] [Google Scholar]
- 12.Pankhurst FP, Horne JA. The influence of bed partners on movement during sleep. Sleep. 1994;17:308–15. doi: 10.1093/sleep/17.4.308. [DOI] [PubMed] [Google Scholar]
- 13.Meadows R, Venn S, Hislop J, Stanley N, Arber S. Investigating couples' sleep: an evaluation of actigraphic analysis techniques. J Sleep Res. 2005;14:377–86. doi: 10.1111/j.1365-2869.2005.00485.x. [DOI] [PubMed] [Google Scholar]
- 14.Hasler BP, Troxel WM. Couples' nighttime sleep efficiency and concordance: evidence for bidirectional associations with daytime relationship functioning. Psychosom Med. 2010;72:794–801. doi: 10.1097/PSY.0b013e3181ecd08a. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Troxel WM, Robles TF, Hall M, Buysse DJ. Marital quality and the marital bed: examining the covariation between relationship quality and sleep. Sleep Med Rev. 2007;11:389–404. doi: 10.1016/j.smrv.2007.05.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Meadows R, Arber S, Venn S, Hislop J, Stanley N. Exploring the interdependence of couples' rest-wake cycles: an actigraphic study. Chronobiol Int. 2009;26:80–92. doi: 10.1080/07420520802678452. [DOI] [PubMed] [Google Scholar]
- 17.Troxel WM. It's more than sex: exploring the dyadic nature of sleep and implications for health. Psychosom Med. 2010;72:578–86. doi: 10.1097/PSY.0b013e3181de7ff8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Troxel WM, Buysse DJ, Hall M, Matthews KA. Marital happiness and sleep disturbances in a multi-ethnic sample of middle-aged women. Behav Sleep Med. 2009;7:2–19. doi: 10.1080/15402000802577736. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Carmichael CL, Reis HT. Attachment, sleep quality, and depressed affect. Health Psychol. 2005;24:526–31. doi: 10.1037/0278-6133.24.5.526. [DOI] [PubMed] [Google Scholar]
- 20.Scharfe E, Eldredge D. Associations between attachment representations and health behaviors in late adolescence. J Health Psychol. 2001;6:295–307. doi: 10.1177/135910530100600303. [DOI] [PubMed] [Google Scholar]
- 21.Saxbe D, Repetti RL. For better or worse? Coregulation of couples' cortisol levels and mood states. J Pers Soc Psychol. 2010;98:92–103. doi: 10.1037/a0016959. [DOI] [PubMed] [Google Scholar]
- 22.De Waterman AL, Kerkhof G. Sleep-wake patterns of partners. Percept Mot Skills. 1998;86:1141–2. doi: 10.2466/pms.1998.86.3c.1141. [DOI] [PubMed] [Google Scholar]
- 23.Larson JH, Crane D, Smith CW. Morning and night couples: the effect of wake and sleep patterns on marital adjustment. J Marital Fam Ther. 1991;17:53–65. [Google Scholar]
- 24.Troxel WM, Cyranowski JM, Hall M, Frank E, Buysse DJ. Attachment anxiety, relationship context, and sleep in women with recurrent major depression. Psychosom Med. 2007;69:692–9. doi: 10.1097/PSY.0b013e3180cc2ec7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Hazan C, Shaver PR. Attachment as an organizational framework for research on close relationships. Psychological Inquiry: An International Journal for the Advancement of Psychological Theory. 1994;5:1–22. [Google Scholar]
- 26.Fraley RC, Shaver PR. Adult romantic attachment: theoretical developments, emerging controversies, and unanswered questions. Review of General Psychology. 2000;4:132–54. [Google Scholar]
- 27.Fraley RC, Waller NG, Brennan KA. An item response theory analysis of self-report measures of adult attachment. J Pers Soc Psychol. 2000;78:350–65. doi: 10.1037//0022-3514.78.2.350. [DOI] [PubMed] [Google Scholar]
- 28.Brennan KA, Clark CL, Shaver PR. Self-report measurement of adult attachment. In: Simpson JA, Rholes WS, editors. Attachment Theory and Close Relationships. New York: Guilford; 1998. pp. 46–76. [Google Scholar]
- 29.Sibley CG, Fischer R, Liu JH. Reliability and validity of the revised experiences in close relationships (ECR-R) self-report measure of adult romantic attachment. Pers Soc Psychol Bull. 2005;31:1524–36. doi: 10.1177/0146167205276865. [DOI] [PubMed] [Google Scholar]
- 30.Spanier G. Measuring dyadic adjustment: new scales for assessing the quality of marriage and similar dyads. Journal of Marriage and the Family. 1976;38:15–28. [Google Scholar]
- 31.Smith CS, Reilly C, Midkiff K. Evaluation of three circadian rhythm questionnaires with suggestions for an improved measure of morningness. J Appl Physiol. 1989;74:728–38. doi: 10.1037/0021-9010.74.5.728. [DOI] [PubMed] [Google Scholar]
- 32.Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28:193–213. doi: 10.1016/0165-1781(89)90047-4. [DOI] [PubMed] [Google Scholar]
- 33.Morin CM, Espie CA. New York: Kluwer Academic/Plenum Publishers; 2003. Insomnia: a clinical guide to assessment and treatment. [Google Scholar]
- 34.Cohen J, Cohen P, West SG, Aiken LS. 3rd ed. Mahwah: Lawrence Erlbaum Associates; 2003. Applied multiple regression/ correlation analysis for the behavioral sciences. [Google Scholar]
- 35.Don BP, Mickelson KD. Relationship satisfaction trajectories across the transition to parenthood among low-risk parents. Journal of Marriage and Family. 2014;76:677–92. [Google Scholar]
- 36.Meltzer LJ, Mindell JA. Relationship between child sleep disturbances and maternal sleep, mood, and parenting stress: a pilot study. J Fam Psychol. 2007;21:67–73. doi: 10.1037/0893-3200.21.1.67. [DOI] [PubMed] [Google Scholar]
- 37.Fraley RC, Heffernan ME, Vicary AM, Brumbaugh CC. The Experiences in Close Relationships-Relationship Structures Questionnaire: a method for assessing attachment orientations across relationships. Psychol Assess. 2011;23:615–25. doi: 10.1037/a0022898. [DOI] [PubMed] [Google Scholar]
- 38.Marino M, Li Y, Rueschman MN, et al. Measuring sleep: accuracy, sensitivity, and specificity of wrist actigraphy compared to polysomnography. Sleep. 2013;36:1747–55. doi: 10.5665/sleep.3142. [DOI] [PMC free article] [PubMed] [Google Scholar]