

Abstract
Objective
Daily events of discrimination are important factors in understanding health disparities. Vigilant coping, or protecting against anticipated discrimination by monitoring and modifying behaviour, is an understudied mechanism that may link discrimination and health outcomes. This study investigates how responding to everyday discrimination with anticipatory vigilance relates to the health of Black men and women.
Methods
Black adults (N = 221) from the Detroit area completed measures of discrimination, adverse life events, vigilance coping, stress, depressive symptoms and self-reported health.
Results
Vigilance coping strategies mediated the relationship between discrimination and stress. Multi-group path analysis revealed that stress in turn was associated with increased depression in men and women. Self-reported health consequences of stress differed between men and women.
Conclusions
Vigilance coping mediates the link between discrimination and stress, and stress has consequences for health outcomes resulting from discrimination. More research is needed to understand other underlying contributors to discrimination, stress and poor health outcomes as well as to create potential interventions to ameliorate health outcomes in the face of discrimination-related stress.
Keywords: health disparities, discrimination, vigilance, stress, coping strategies, self-rated health
Black Americans have significantly worse health outcomes on multiple health indicators than White Americans (Williams, 1999), and chronic experiences of discrimination are a major component in the creation of these health disparities (Mays, Cochran, & Barnes, 2007; Williams, Neighbors, & Jackson, 2008). Self-reports of discrimination have been linked to stress, and both discrimination and stress are associated with a wide range of negative health indicators and outcomes (Pascoe & Richman, 2009; Williams & Mohammed, 2009). The psychosocial mechanisms that operate in these processes are poorly understood. The current work begins to fill the gap by examining the mechanism of anticipatory vigilant behaviours in the context of Pascoe’s discrimination-health model (Pascoe & Richman, 2009). It further extends the vital, but limited, research on gender differences in the relationship between discrimination, psychosocial reactions to discrimination and health outcomes for Black men and women.
Everyday discrimination has an additive, negative, impact on Black Americans’ health (Williams et al., 2008). Meta-analysis indicates discrimination negatively impacts health indirectly through increased physiological stress responses and unhealthy stress-coping behaviours (Pascoe & Richman, 2009). Self-reports of discrimination have been linked to a wide range of health indicators and outcomes including depression (Borrell, Kiefe, Williams, Diez-Roux, & Gordon-Larsen, 2006) and overall self-reported health (Brondolo et al., 2011). Discrimination experiences have been causally linked to an increase in depressive symptoms (Schulz et al., 2006), and longitudinal evidence suggests that discrimination incrementally contributes to depression, rather than depression increasing attention to discriminatory experiences (Brown et al., 2000). Discrimination has been linked to general poor self-reported health among multiple racial and ethnic minority group members (Molina, Alegría, & Mahalingam, 2013).
In a recent meta-analysis, Pascoe and colleagues described a broad discrimination-health model generated from the extant literature to begin to frame how discrimination negatively influences health. The discrimination-health model theorises that, along with direct effects and influencing health behaviours, discrimination impacts physical and mental health by increasing stress (Pascoe & Richman, 2009). This model incorporates the stress-coping framework, as discrimination operates as a constant and uncontrollable stressor that increases the stress response (Pascoe & Richman, 2009; Sawyer, Major, Casad, Townsend, & Mendes, 2012). Stress then has negative downstream consequences for health and health behaviours.
Understanding the mechanisms through which discrimination operates in health disparities is paramount to creating effective interventions and policies to begin to close the gap (Williams et al., 2008), and the discrimination-stress model postulates that coping styles mediate the relationship between discrimination and stress (Pascoe & Richman, 2009). Though research has begun to explore the psychosocial processes that mediate the relationship between discrimination and health (Adler & Conner Snibbe, 2003; Molina et al., 2013), research on the relationship between coping with discrimination and health has been limited. Generally, active coping mechanisms (such as seeking support from social networks or confronting) have positive effects on health (Brondolo, Brady Ver Halen, Pencille, Beatty, & Contrada, 2009; Krieger & Sidney, 1996; Smith, Ruiz, & Uchino, 2000), as well as the potential to ameliorate the negative relationship between discrimination and health (Clark & Adams, 2004; Noh & Kaspar, 2003; Pascoe & Richman, 2009). Passive coping mechanisms (such as disengagement or substance use) are generally linked with negative health effects (Brondolo et al., 2009; Krieger & Sidney, 1996; Smith et al., 2000), and can exacerbate the relationship between discrimination and health (Noh & Kaspar, 2003; Pascoe & Richman, 2009), but this may be context specific (Noh, Beiser, & Kaspar, 1999; Wei, Heppner, Ku, & Liao, 2010). These relationships are further complicated by evidence suggesting that discrimination may decrease the use of active coping (Bianchi, Zea, Poppen, Reisen, & Echeverry, 2004). Even though vigilant coping, a passive coping strategy, has been theorised as an important psychosocial mechanism in the relationship between discrimination, stress and health (Pascoe & Richman, 2009; Williams & Mohammed, 2009), research on this relationship remains limited.
Discrimination-related vigilance, a coping mechanism characterised by attempting to protect oneself from anticipated discrimination by continuously monitoring and modifying one’s behaviour and surroundings (Hicken, Lee, Ailshire, Burgard, & Williams, 2013), is a potentially important mechanism in the complex relationship between discrimination and health. Simply anticipating discrimination can increase stress and cardiovascular reactivity associated with stress (Sawyer et al., 2012). Perseverative cognitions related to vigilance, such as worry and rumination, can lead to increased somatic complaints, changes in immunology reaction, loss of sleep, and negative cardiac effects (Brosschot, Gerin, & Thayer, 2006; Clark, Benkert, & Flack, 2006; Williams & Mohammed, 2009). Moreover, attending to cues in the social environment (i.e. vigilance) has been shown to increase blood pressure (Smith et al., 2000). Thus, prolonged vigilance, especially in response to discrimination (see Hicken et al., 2013), may have serious long-term consequences for stress-related health outcomes.
Recent research has examined the potential health-related outcomes of discrimination-related vigilance focusing specifically on events that could involve racism (Clark et al., 2006; Hicken et al., 2013). Specifically, racism-related vigilance is related to racial health disparities in sleep functioning (Hicken et al., 2013) and arterial elasticity in Black Americans (Clark et al., 2006). Though these previous studies do not explicitly measure stress, they do indicate that discrimination-related vigilance is, in and of itself, a stressor leading to sleep disruption and an increase in precursors to hypertension (Clark et al., 2006; Hicken et al., 2013). Despite this initial work on vigilance, studies investigating the role of vigilance in the discrimination-health disparity link are still limited (Sawyer et al., 2012). To our knowledge, no study has investigated the direct and indirect relationship between everyday discrimination, vigilance and health outcomes; the current work will explicitly investigate vigilance in the discrimination-health link.
The intersectional impact of race and gender can further illuminate the relationship between discrimination and health (Greer, 2011; Molina et al., 2013; Pascoe & Richman, 2009). There is a large body of literature exploring gender differences in perceived discrimination (Paradies, 2006) and health outcomes (Bertakis, Azari, Helms, Callahan, & Robbins, 2000; McGee, Liao, Cao, & Cooper, 1999) for racial and ethnic minority men and women. Though Black men and women may experience similar levels of discrimination (Landrine & Klonoff, 1996), they may have different experiences of, and reactions to, racism (Clark, 2004; Paradies, 2006). Black men may be more likely to experience institutional discrimination (e.g. from the legal system), and furthermore may be perceived as more prototypically Black which may influence the types of discrimination they experience (Johnson, Freeman, & Pauker, 2012; Utsey, Payne, Jackson, & Jones, 2002). On the other hand, Black women may experience additional stressors in the form of sexism (Perry, Harp, & Oser, 2013; Szymanski & Stewart, 2010), as well as intersectional discrimination stemming from the relationship between their gender and race (Johnson et al., 2012). Black men and women also may rely on different strategies to deal with discrimination (Clark, 2004), and these coping strategies may influence health outcomes related to discrimination (Brondolo et al., 2009; Paradies, 2006; Pascoe & Richman, 2009)
Few studies have directly examined gender differences in the relationship between discrimination and health outcomes (Pascoe & Richman, 2009), however, the extant research does provide evidence that the relationships between discrimination and health may differ for men and women. For example, Black young men may have increased cardiovascular activity in response to discrimination compared to Black young women (Clark et al., 2006), and coping by attempting to disprove stereotypes may have positive health benefits for women, but not for men (Clark & Adams, 2004). Similarly, compared to Latino men, Latina women may have a stronger relationship between discrimination and distress (Molina et al., 2013). Though research in this area is growing, the paucity of current evidence necessitates continued investigations into gender differences.
In this study, we focus on gender differences in self-reported health and depression. Previous research suggests that these negative health outcomes can vary by gender (Bertakis et al., 2000; McGee et al., 1999; Nolen-Hoeksema, 2001). Women have a higher incidence of depression compared to men (Nolen-Hoeksema, 2001), and discrimination (Molina et al., 2013) and stress (Hyde, Mezulis, & Abramson, 2008) may play roles in developing these differences. Thus, we expect to find a larger association between stress and depression in women. Likewise, given literature indicating more self-reported poor health in women compared to men (Bertakis et al., 2000; McGee et al., 1999), we could expect a stronger association between stress and health for women compared to men. This research aims to add to the current literature addressing gender differences and to lay a foundation for future work in the area.
This research has several aims. First, we situate vigilance into current understandings of the relationship between discrimination, stress and health using path analysis. This tests the hypothesis that vigilance mediates the relationship between discrimination and stress, and further models how vigilance to discrimination is indirectly related to health disparity outcomes associated with discrimination and stress: symptoms of depression and overall self-reported health (Brondolo et al., 2011; Pascoe & Richman, 2009; Williams & Mohammed, 2009). Second, this study explores how this piece of the discrimination-health model differs among Black men and women using multiple-groups analysis. Though the relationships between vigilance, stress and health have been hypothezized to be different for men and women (Pascoe & Richman, 2009), few studies have directly addressed this. Specifically, we hypothesise depression and self-reported poor health will be more strongly related to stress in women compared to men.
Methods
Participants
This analysis focuses on a sub-sample of Black-identified (N = 221) respondents from the 1995 Detroit Area Study (DAS; Jackson & Williams, 1995) who indicated frequent experiences of discrimination. The 1995 DAS, a multi-stage area probability sample involving adult respondents residing in three counties in Michigan, focused on social influences on health and oversampled African-Americans. This sample was 66.1% female (n = 146), with a mean age of 40.03 (SD = 14.31), and a median household income of $20,000–$39,000.
Measures
Discrimination
Everyday discrimination (M = 2.64, SD = .66, α = .70; original α = .88) comprised mean responses to nine items assessing everyday occurrences of negative treatment (Taylor, Kamarck, & Shiffman, 2004; Williams, Yu, Jackson, & Anderson, 1997). Following the prompt, ‘In your day-to-day life how often have any of the following things happened to you?’ participants rated items (e.g. ‘You are called names or insulted’, ‘You are treated with less courtesy than other people’, and ‘People act as if they are afraid of you’) on a Likert scale with options including 1 (never), 2 (fairly often), 3 (not too often), 4 (hardly ever) and 5 (never). Items were reverse coded so higher scores reflect more everyday discrimination (Taylor et al., 2004; Williams et al., 1997).
Vigilance
The vigilance scale included six items (M = 3.60, SD = .92, α = .77; original α = .72), rated on a Likert scale with options including 1 (never), 2 (fairly often), 3 (not too often), 4 (hardly ever) and 5 (never). Items were reverse coded so that higher scores reflect more vigilance. The measure of vigilance to discrimination was only administered to participants who indicated they experienced at least one of the discrimination items ‘very often’ or ‘fairly often’ and could be included in this analysis (N = 221 of 586). This scale was developed for the 1995 Detroit Area Study, however, it has been used in subsequent studies assessing the influence of vigilance on health (Clark et al., 2006; Hicken et al., 2013). Participants indicated how often they engaged in several behaviours in response to the everyday experiences described above. Sample behaviours included, ‘Carefully observe what happens around you’, ‘Try to avoid certain social situations and places’ and ‘Carefully watch what you say and how you say it’.
Stress
The four-item perceived stress scale (M = 2.39, SD = .77, α = .56; original α = .60) was used to measure stress (Cohen, 1988). Following the prompt, ‘In the past 30 days, how often did you feel’,-participants rated items on a Likert scale with options including 1 (never), 2 (fairly often), 3 (not too often), 4 (hardly ever) and 5 (never). Two items were reverse coded so higher scores reflect more stress (Cohen, 1988). The four items were ‘Confident about your ability to handle your personal problems?’ ‘That things were going your way?’ ‘You were unable to control important things in your life?’ and ‘That difficulties were piling up so high that you could not overcome them?’
Depressive symptomology
Depressive symptoms (M = 2.32, SD = .92, α = .82; original α = .89) included a six-item scale developed by Kessler and Mroczek (1994). Following the prompt ‘In the past 30 days, how often did you feel’, participants rated items on a Likert scale with options including 1 (never), 2 (fairly often), 3 (not too often), 4 (hardly ever) and 5 (never). Higher scores reflect a greater frequency of symptoms of psychological distress. Sample items included ‘Hopeless?’ ‘Restless or fidgety?’ and ‘That everything was an effort?’.
Self-reported health
Self-reported health (M = 3.23, SD = 1.15) was measured using a single item, ‘Would you say your health is excellent, very good, good, fair, or poor?’ Possible values included 1 (excellent), 2 (very good), 3 (good), 4 (fair) and 5 (poor) with higher scores indicating worse health. Single-item self-reported health measures have been shown to have good external validity (Desalvo, Bloser, Reynolds, He, & Muntner, 2005) and have spurred a research movement on the importance of self-rated health (Jylhä, 2009).
Covariates
In order to control for the known effects of income on stress and health (Adler & Conner Snibbe, 2003; Williams, 1999), and to distinguish discrimination-related stress from stressful life events, we included two covariates, distressing life events and income. Distressing life events (M = 1.99, SD = 1.72) was measured by counting affirmative responses to nine possible distressing life events in the year before the interview. Participants indicated whether the event happened (1, yes) or not (0, no). Higher numbers indicated more stressful life events (Williams et al., 1997). Sample items include, ‘Have you been the victim of a serious physical attack or assault?’ ‘Have you had any serious financial problems or difficulties?’ and ‘Were you robbed or was your home burglarized?’ Participants indicated income numerically and reported a category of total yearly income prior to taxes. Data were collapsed into a five-category income variable with the following possible responses: (1) less than $10,000; (2) $10,001–$19,999 (3) $20,000–$39,999; (4) $40,000–$59,999; and (5) greater than $60,000), and the median household income was $20,000–$39,000.
Results
Table 1 presents the statistics for the sample in this study presented separately by gender, and Table 2 presents the correlations for the combined study sample, however, the measures used and associated psychometrics for the entire DAS sample are described in detail in the DAS material online (Jackson & Williams, 1995) and in other publications using this sample (Brown et al., 2000).
Table 1.
Summary of intercorrelations, means and standard deviations for study variables by gender.
| Measure | Male
|
Female
|
1 | 2 | 3 | 4 | 5 | ||
|---|---|---|---|---|---|---|---|---|---|
| M | SD | M | SD | ||||||
| Discrimination | 2.71 | .69 | 2.61 | .65 | – | .35** | .31** | .16 | .1 |
| Vigilance | 3.52 | .94 | 3.65 | .92 | .32** | – | .27* | .12 | .15 |
| Stress | 2.26 | .77 | 2.45** | .76 | .18* | .27** | – | .57** | .09 |
| Depression | 2.08 | .8 | 2.44 *** | .92 | .28** | .27** | .62** | – | .19 |
| Self-Reported Poor Health | 2.53 | 1.18 | 2.89* | 1.13 | .03 | .14 | .25** | .28** | – |
Notes: Intercorrelations for men are presented above the diagonal and intercorrelations for women are presented below the diagonal. Means and standard deviations for men are presented in the vertical columns and means and standard deviations for women are presented in the horizontal columns.
p < .05
p < .01
p < .001.
Table 2.
Summary of intercorrelations for full sample.
| Measure | 1 | 2 | 3 | 4 | |
|---|---|---|---|---|---|
| 1. | Discrimination | ||||
| 2. | Vigilance | .33*** | |||
| 3. | Stress | .21** | .28*** | ||
| 4. | Depression | .22** | .23** | .61** | |
| 5. | Self-reported poor health | .04 | .15* | .20** | .27*** |
Notes: Intercorrelations are presented for the current sample. The model was estimated separately for men and women.
p < .05
p < .01
p < .001.
Preliminary analysis
We compared our sub-sample (N = 221) to the sample of Black-identified participants from the Detroit Area Study not included in the model (N = 365; see Participants section for more details). These excluded participants were 69.9% female (n = 255), with a mean age of 48.12 (SD = 17.66), and a median household income of $20,000–$39,000. Our sub-sample was significantly younger (M = 40.03, SD = 14.31; M = 48.12, SD = 17.66: t (575) = 5.72, p < .001), poorer (categorical income M = 2.58, SD = 1.38; M = 2.81, SD = 1.29: t (582) = 2.03, p = .042) and less likely to own a home (M = .51, SD = .50; M = .65, SD = .48: t (581) = 3.32, p = .001) than the Black-identified participants not included in the current study. The sub-sample included in the current study had an equivalent amount of education (categorical education M = 2.51, SD = .93; M = 2.44, SD = .97: t (581) = −.93, ns) and were equally likely to be married (M = .32, SD = .47; M = .35, SD = .48: t (582) = .69, ns) compared to the excluded Black-identified participants.
Statistical analysis plan
In order to investigate the aims of this study, we created a multiple-groups path model using maximum-likelihood estimation in MPlus 6.1 (see Figure 1; Muthén & Muthén, 2010). To examine the indirect effect (i.e. mediating impact) of vigilance on the relationship between discrimination and stress, we bootstrapped confidence intervals of the indirect effect within our final model (Kline, 2011). Bootstrapped confidence intervals are a robust method for testing for the significance of indirect effects, as they do not assume a normal distribution of effects. If there was a significant indirect effect of discrimination on stress through vigilance, we would expect that the bootstrapped confidence intervals would not contain zero. This test for mediation was embedded in the overall path model, and the confidence intervals for the indirect effect were produced using MPlus 6.1 (Kline, 2011). Following the discrimination-health model, we predicted that discrimination and vigilance would influence depression and self-reported health indirectly through stress (Pascoe & Richman, 2009), even while controlling for income and the effect of negative life events on stress. Given the impact of SES on discrimination and health (Williams, 1999), we controlled for income in every relationship in the model. Stressful life events were included as a covariate in the pathways to vigilance and stress to ensure that any relationship between discrimination, vigilance and stress was above and beyond that of stressful life events.
Figure 1.
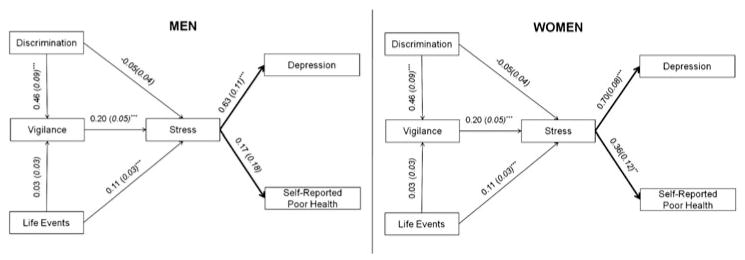
Multiple group path model comparing Black men and women. Unstandardized coefficients and standard errors are presented for each path. All paths control for income, though for simplicity income is not depicted in this figure. Paths indicated in bold varied by gender; all other paths were equal across groups.
**p < .01, ***p < .001.
To test for a difference in the relationship between stress and health dependent on gender, we investigated the differences between males and females in a multiple-groups path models (Kenny, Kashy, & Cook, 2006). This model tested the important downstream consequences of the discrimination-health model (see Figure 1) comparing men and women using maximum-likelihood estimation in MPlus 6.1 (Muthén & Muthén, 2010). We hypothesised stress would impact depression and poor self-reported health more strongly in women than men.
Multiple groups path analysis
Following Kline (2011), testing a multi-group model involves three steps (1) testing a model in which all paths are allowed to vary between groups (i.e. the common model) to examine model fit, (2) testing a path invariant model in which all paths are constrained to be equal across groups, and if model fit suffers and (3) testing which paths differ significantly between groups. Paths that are significantly different are then released, allowing them to vary between groups, enabling an examination of which relationships are different by group membership, in this case gender.
Good-fitting models should have a root mean square error of approximation (RMSEA) less than or equal to .08, a comparative fit index (CFI) greater than or equal to .95, and a Tucker-Lewis index (TLI) greater than or equal to .95 (Hu & Bentler, 1998; Kline, 2011). The common model met all fit criteria (Hu & Bentler, 1998; Kline, 2011) and constraining paths to be equal across groups caused the model fit to suffer ( , p < .001), suggesting that there were gender differences. Chi-square difference tests, which are standard modification indices in path analysis, were used to determine which, if any, paths should be allowed to vary between men and women. These difference tests represent the difference in chi-square values for the original model and the model where a path is unconstrained (Kline, 2011). These modification indices suggested that the paths between stress and depression ( , p < .001), and stress and self-rated health ( , p = .005), should be released in the final model. Chi-square difference tests indicated the following paths were not different across groups: discrimination to vigilance ( , p = .975), life events to vigilance ( , p = .444), stress to vigilance ( , p = .528), life events to stress ( , p = .153) and discrimination to stress ( , p = .224). Following existing guidelines (Hu & Bentler, 1998; Kline, 2011), this final model fit well to the data (χ2 (27) = 24.41, p = .274; RMSEA = .04 (.00, .09); CFI = .98; TLI = .97) and was not significantly different from the common model ( , p = .329). The coefficients from this final, two-group, model are presented in Figure 1. Covariates did not significantly contribute to the model, with the exception that income negatively predicted depression in women, such that a lower income was associated with higher depressive symptoms, and stressful life events positively predicted stress.
Vigilance effects
The relationship between discrimination and stress in the model was mediated by vigilance for both men and women. A 95% bootstrapped confidence interval in the context of the larger model indicated vigilance mediated the relationship between discrimination and stress (.07, .20). Stressful life events did not directly impact vigilance, however, these life events were associated with increased stress in both men and women. Thus, the relationship between discrimination and stress was significantly explained by vigilance, suggesting that coping with discrimination through anticipatory vigilance can help explain why discrimination may be stress inducing.
Gender effects
The relationship between stress and both self-reported health and depression was different for men and women (see Figure 1). Both men and women experienced a significant, positive, relationship between depression symptoms and stress, such that an increase in stress was associated with an increase in depression symptoms; however, this relationship was stronger for women than men. In contrast, women, but not men, rated their health more poorly in response to stress.
Discussion
The current study examined direct and indirect effects of vigilance in the discrimination-health model for Black men and women. As predicted, vigilance mediated the relationship between discrimination and stress. Consistent with the discrimination-health model (Pascoe & Richman, 2009), vigilance exacerbated stress to negatively impact health outcomes. Stress predicted symptoms of depression in Black men and women. Stress also predicted lower self-rated health for women. Thus, the effects of stress were meaningfully different for Black women and Black men who have experienced discrimination.
This study was the first to investigate vigilance as a mediator in the relationship between discrimination and stress for Black Americans. Prior work suggested that mere anticipation of discrimination evoked physiological arousal and stress (Sawyer et al., 2012). Consistent with this research, we demonstrated that Black men and women who adopted a vigilant coping style in response to discrimination reported greater stress. To guard against future threats, stigmatised group members may remain in an aroused, vigilant state to protect themselves psychologically, yet this maladaptive strategy puts them at risk for greater stress. As vigilance is more common among those who experience greater discrimination, and those who experience discrimination are least likely to seek health care (Williams, 1999), individuals who adopt vigilant coping strategies may also be at heightened risk for untreated physical and mental health-related problems. In a broader context, if vigilance to discrimination exacerbates stress as our results suggest, further research is warranted to investigate effective coping mechanisms which may serve to buffer negative health outcomes related to discrimination-induced stress. Given the potential negative impact of vigilance coping, health interventions may need to focus on developing more adaptive coping strategies. The current research underscores the importance of research on coping styles (Pascoe & Richman, 2009). Coping strategies are a particularly malleable aspect of discrimination-health model, and future intervention research could be greatly informed by a better understanding of the relationship between coping with discrimination and health.
This study further addresses potential gender differences in the discrimination-health model, adding to the limited intersectional research addressing the relationship between discrimination and health (Greer, 2011; Pascoe & Richman, 2009). Prior research implicated discrimination in depression (Borrell et al., 2006; Brown et al., 2000) and gender differences in depression favouring more prevalence among women (Nolen-Hoeksema, 2001). Thus, we hypothesised and found a stronger relationship between stress and depression in women compared to men, though the relationship between stress and health was significant in both men and women. Likewise, prior research implicated discrimination in self-reported poor health (Brondolo et al., 2011; Molina et al., 2013) and literature indicated more self-reported poor health among women compared to men (Bertakis et al., 2000; McGee et al., 1999). Thus, we hypothesised a stronger relationship between stress and self-reported poor health in women compared to men; our results indicated a significant relationship for women only. It may be that men inflate their health status or minimise health-related problems (see Courtenay, 2003) explaining why a significant relationship exists only for women. This study expands upon that research by suggesting gender may be important in understanding in the relationship between stress and the outcomes of depression and self-rated health. These findings suggest that among a sample of Black men and women who experienced discrimination, stress may impact health outcomes in significantly different ways. Interventions aiming to reduce health disparities through stress reduction should continue to consider gender differences in the relationship between discrimination and health. Future research is also needed to disentangle the gender-specific stress outcomes related to vigilance and discrimination.
Limitations and future directions
This study is the first, to our knowledge, to examine vigilance in the context of the discrimination-health model. It is also the first to assess whether vigilance may account for the relationship between discrimination and stress. Furthermore, it adds to the limited body of research (Clark et al., 2006) on the potential gender differences in the relationships between vigilance, stress and health (Pascoe & Richman, 2009). Despite these strengths, this study is not without limitations.
First, cross-sectional data leave open the alternative possibility that stress mediates the relationship between discrimination and vigilance. That is, it is possible that individuals who are more stressed by discrimination will engage in more vigilance coping. Though this question deserves empirical study, it should be noted that everyday experiences of discrimination, not stressful life events, significantly contributed to vigilance in this model. As stressful life events did not increase vigilant responses, this lends evidence that stress itself also did not increase this style of coping. Furthermore, an alternative model representing this relationship did not fit the data well, (χ2 (27) = 139.82, p < .001; RMSEA = .20 (.16, .23); CFI = .46; TLI = .01) nor was the fit as good as the hypothesised and reported model (AIC Final Model, 3182.73; AIC Alternate Model, 3294.17). This evidence suggests that vigilance as a coping mechanism is not simply an artefact of general stress, but a specific consequence of prior experience with discrimination. However, only longitudinal designs can confirm this mediation effect, and future studies should draw upon longitudinal data to investigate the causal relationship between discrimination, vigilance and stress.
Second, the sample was limited to participants who reported significant discrimination experiences; only these participants answered questions about vigilance. Vigilant coping behaviours in response to discrimination were largely expected to be utilised by those who had significant prior discrimination experiences. Moreover, using only a sample of participants who experienced discrimination allowed us to focus on an at-risk health population. Still, it is unclear whether some individuals who were unwilling to report racial discrimination still engage in vigilant behaviours, or use vigilance to discrimination as a coping strategy to avoid discrimination. For example, prior research suggests that members of stigmatised groups recognise that their groups experience discrimination while seeing themselves as personally experiencing little, if any, discrimination (Dion & Kawakami, 1996). Seeing one’s group as a target of discrimination could lead to vigilant coping despite no prior personal experience. Vigilance may be deleterious to health outcomes only to participants who have experienced personal discrimination, or it may have effects independent of personal discrimination experiences. This study also did not control for cognitions that are conceptually related to vigilance, such as rumination and anxiety disorders. Thus, it is possible that only individuals who are generally high in anxiety or experience clinical levels of anxiety may rely on vigilance coping strategies. We did not control for psychopathology in these analyses, but future research should examine the role of mental health in vigilance coping.
The measure of stress is also a limitation of this work. First, self-reported perceived stress was measured, so it is unknown if the perceptions of stress, or the physiological repercussions of stress, are the most to blame for negative health outcomes. Furthermore, the four-item Cohen’s stress scale measured in this study is less reliable than the 10-item scale. Despite the low reliability of our stress measure, we believe there is reason to have confidence in our findings. The stress results in this paper are congruent with previous research on the discrimination-stress model, suggesting links between discrimination and stress, and stress and health outcomes. Furthermore, our findings also converge with emerging evidence suggesting that vigilance can increase stress (Hicken et al., 2013; Sawyer et al., 2012). However, future work should incorporate both more reliable self-report measures, as well as physiological measures, of stress.
Finally, though the current research largely focuses on the pitfalls of vigilance, these negative consequences may be an artefact of a focus on discrimination-related health outcomes. It is therefore possible that vigilance is effective in preparing individuals for stressful events in psychological or interpersonal pathways not measured here. For example, vigilance may foster feelings of autonomy and control among racial and ethnic group minority members that could aid in dealing with social stigma. Moreover, coping strategies are not mutually exclusive; some individuals may engage in vigilant coping in conjunction with other coping strategies that tend to be more protective and health promoting. Future research should examine the interactive effects of multiple, and multifaceted, coping styles.
Future research should also investigate how vigilance influences the health outcomes across different racial and ethnic groups, and across geographies. The nature of discrimination racial and ethnic group minority members experience is not uniform across racial and ethnic groups, especially when gender is taken into consideration (e.g. Molina et al., 2013). In addition, geographical contexts (e.g. neighbourhood segregation, region of the country) can greatly influence forms of discrimination deployed as well as perceptions of discrimination (Hunt, Wise, Jipguep, Cozier, & Rosenberg, 2007). Coping mechanisms, such as vigilance, may also present differentially across geography and racial and ethnic groups, both in the cause and consequence of these strategies. Research explicating the similarities and differences between groups and geographical locations can benefit understanding of health disparities, and in turn, policies to address them.
The current results extend the limited knowledge on vigilant coping in the discrimination-health model. This study reveals that vigilance among Black men and women may promote stress that affects multifaceted health outcomes, and points towards crucial avenues for future research. Vigilance, as a mediator between discrimination and stress, may be a vital link to understanding the relationship between discrimination and health.
References
- Adler NE, Conner Snibbe A. The role of psychosocial processes in explaining the gradient between socioeconomic status and health. Current Directions in Psychological Science. 2003;12:119–123. doi: 10.1111/1467-8721.01245. [DOI] [Google Scholar]
- Bertakis KD, Azari R, Helms LJ, Callahan EJ, Robbins JA. Gender differences in the utilization of health care services. The Journal of Family Practice. 2000;49:147–152. [PubMed] [Google Scholar]
- Bianchi FT, Zea MC, Poppen PJ, Reisen CA, Echeverry JJ. Coping as a mediator of the impact of sociocultural factors on health behavior among HIV-positive Latino gay men. Psychology & Health. 2004;19:89–101. doi: 10.1080/08870440410001655340. [DOI] [Google Scholar]
- Borrell LN, Kiefe CI, Williams DR, Diez-Roux AV, Gordon-Larsen P. Self-reported health, perceived racial discrimination, and skin color in African Americans in the CARDIA study. Social Science and Medicine. 2006;63:1415–1427. doi: 10.1016/j.socsci-med.2006.04.008. [DOI] [PubMed] [Google Scholar]
- Brondolo E, Brady Ver Halen N, Pencille M, Beatty D, Contrada RJ. Coping with racism: A selective review of the literature and a theoretical and methodological critique. Journal of Behavioral Medicine. 2009;32:64–88. doi: 10.1007/s10865-008-9193-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brondolo E, Hausmann LR, Jhalani J, Pencille M, Atencio-Bacayon J, Kumar A, Schwartz J. Dimensions of perceived racism and self-reported health: Examination of racial/ethnic differences and potential mediators. Annals of Behavioral Medicine. 2011;42:14–28. doi: 10.1007/s12160-011-9265-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brosschot JF, Gerin W, Thayer JF. The perseverative cognition hypothesis: A review of worry, prolonged stress-related physiological activation, and health. Journal of Psychosomatic Research. 2006;60:113–124. doi: 10.1016/j.jpsychores.2005.06.074. [DOI] [PubMed] [Google Scholar]
- Brown TN, Williams DR, Jackson JS, Neighbors HW, Torres M, Sellers SL, Brown KT. “Being Black and feeling blue”: The mental health consequences of racial discrimination. Race and Society. 2000;2:117–131. doi: 10.1016/S1090-9524(00)00010-3. [DOI] [Google Scholar]
- Clark R. Interethnic group and intraethnic group racism: Perceptions and coping in Black University students. Journal of Black Psychology. 2004;30:506–526. doi: 10.1177/0095798404268286. [DOI] [Google Scholar]
- Clark R, Adams JH. Moderating effects of perceived racism on John Henryism and blood pressure reactivity in Black female college students. Annals of Behavioral Medicine. 2004;28:126–131. doi: 10.1207/s15324796abm2802_8. [DOI] [PubMed] [Google Scholar]
- Clark R, Benkert R, Flack J. Large arterial elasticity varies as a function of gender and racism-related vigilance in Black youth. Journal of Adolescent Health. 2006;39:562–569. doi: 10.1016/j.jadohealth.2006.02.012. [DOI] [PubMed] [Google Scholar]
- Cohen S. Perceived stress in a probability sample of the United States. In: Spacapan S, Oskamp S, editors. The social psychology of health. Newbury Park, CA: Sage; 1988. pp. 31–67. [Google Scholar]
- Courtenay WH. Key determinants of the health and well-being of men and boys. International Journal of Men’s Health. 2003;1:1–30. doi: 10.3149/jmh.0201.1. [DOI] [Google Scholar]
- Desalvo KB, Bloser N, Reynolds K, He J, Muntner P. Mortality prediction with a single general self-rated health question. Journal of General Internal Medicine. 2005;21:267–275. doi: 10.1111/j.1525-1497.2005.0291.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dion KL, Kawakami K. Ethnicity and perceived discrimination in Toronto: Another look at the personal/group discrimination discrepancy. Canadian Journal of Behavioural Science. 1996;28:203–213. doi: 10.1037/0008-400X.28.3.203. [DOI] [Google Scholar]
- Greer TM. Coping strategies as moderators of the relation between individual race-related stress and mental health symptoms for African American women. Psychology of Women Quarterly. 2011;35:215–226. doi: 10.1177/0361684311399388. [DOI] [Google Scholar]
- Hicken MT, Lee H, Ailshire J, Burgard SA, Williams DR. “Every shut eye, ain’t sleep”: The role of racism-related vigilance in racial/ethnic disparities in sleep difficulty. Race and Social Problems. 2013;5:100–112. doi: 10.1007/s12552-013-9095-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hu L, Bentler PM. Fit indices in covariance structure modeling: Sensitivity to un-derparameterized model misspecification. Psychological Methods. 1998;3:424–453. doi: 10.1037//1082-989X.3.4.424. [DOI] [Google Scholar]
- Hunt MO, Wise LA, Jipguep MC, Cozier YC, Rosenberg L. Neighborhood racial composition and perceptions of racial discrimination: Evidence From the Black women’s health study. Social Psychology Quarterly. 2007;70:272–289. [Google Scholar]
- Hyde JS, Mezulis AH, Abramson LY. The ABCs of depression: Integrating affective, biological, and cognitive models to explain the emergence of the gender difference in depression. Psychological Review. 2008;115:291–313. doi: 10.1037/0033-295X.115.2.291. [DOI] [PubMed] [Google Scholar]
- Jackson JS, Williams DR. Detroit area study, 1995: Social influence on health: Stress, racism, and health protective resources. Ann Arbor, MI: Inter-university Consortium for Political and SocialResearch [distributor]; 1995. ICPSR03272-v1. 2002-08-16. [DOI] [Google Scholar]
- Johnson KL, Freeman JB, Pauker K. Race is gendered: How covarying phenotypes and stereotypes bias sex categorization. Journal of Personality and Social Psychology. 2012;102:116–131. doi: 10.1037/a0025335. [DOI] [PubMed] [Google Scholar]
- Jylhä M. What is self-rated health and why does it predict mortality? Towards a unified conceptual model. Social Science and Medicine. 2009;69:307–316. doi: 10.1016/j.socsci-med.2009.05.013. [DOI] [PubMed] [Google Scholar]
- Kenny DA, Kashy DA, Cook WL. Dyadic data analysis. New York, NY: Guilford Press; 2006. Using structural equation modeling to study dyads; pp. 100–118. [Google Scholar]
- Kessler RC, Mroczek D. Scoring the UM-CIDI short forms. Ann Arbor, MI: Survey Research; 1994. [Google Scholar]
- Kline RB. Principles and practice of structural equation modeling. 3. New York, NY: Guilford Press; 2011. [Google Scholar]
- Krieger N, Sidney S. Racial discrimination and blood pressure: The CARDIA study of young black and white adults. American Journal of Public Health. 1996;86:1370–1378. doi: 10.2105/AJPH.86.10.1370. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Landrine H, Klonoff E. The schedule of racist events: A measure of racial discrimination and a study of its negative physical and mental health consequences. Journal of Black Psychology. 1996;22:144–168. Retrieved from http://jbp.sagepub.com/content/22/2/144.short. [Google Scholar]
- Mays VM, Cochran SD, Barnes NW. Race, race-based discrimination, and health outcomes among african americans. Annual Review of Psychology. 2007;58:201–225. doi: 10.1146/annurev.psych.57.102904.190212. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McGee DL, Liao Y, Cao G, Cooper RS. Self-reported health status and mortality in a multiethnic US Cohort. American Journal of Epidemiology. 1999;149:41–46. doi: 10.1093/oxfordjournals.aje.a009725. [DOI] [PubMed] [Google Scholar]
- Molina KM, Alegría M, Mahalingam R. A multiple-group path analysis of the role of everyday discrimination on self-rated physical health among Latina/os in the USA. Annals of Behavioral Medicine. 2013;45:33–44. doi: 10.1007/s12160-012-9421-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muthén LK, Muthén BO. Mplus user’s guide. 6. Los Angeles, CA: Author; 2010. [Google Scholar]
- Noh S, Beiser M, Kaspar V. Perceived racial discrimination, depression, and coping: A study of Southeast Asian refugees in Canada. Journal of Health and Social Behavior. 1999;40:193–207. doi: 10.2307/2676348. [DOI] [PubMed] [Google Scholar]
- Noh S, Kaspar V. Perceived discrimination and depression: Moderating effects of coping, acculturation, and ethnic support. American Journal of Public Health. 2003;93:232–238. doi: 10.2105/AJPH.93.2.232. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nolen-Hoeksema S. Gender differences in depression. Current Directions in Psychological Science. 2001;10:173–176. doi: 10.1111/1467-8721.00142. [DOI] [Google Scholar]
- Paradies Y. A systematic review of empirical research on self-reported racism and health. International Journal of Epidemiology. 2006;35:888–901. doi: 10.1093/ije/dyl056. [DOI] [PubMed] [Google Scholar]
- Pascoe EA, Richman LS. Perceived discrimination and health: A meta-analytic review. Psychological Bulletin. 2009;135:531–554. doi: 10.1037/a0016059. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Perry BL, Harp KLH, Oser CB. Racial and gender discrimination in the stress process: Implications for African American women’s health and well-being. Sociological Perspectives. 2013;56:25–48. doi: 10.1525/sop.2012.56.1.25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sawyer PJ, Major B, Casad BJ, Townsend SS, Mendes WB. Discrimination and the stress response: Psychological and physiological consequences of anticipating prejudice in interethnic interactions. American Journal of Public Health. 2012;102:1020–1026. doi: 10.2105/AJPH.2011.300620. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schulz AJ, Gravlee CC, Williams DR, Israel BA, Mentz G, Rowe Z. Discrimination, symptoms of depression, and self-rated health among African American women in detroit: Results from a longitudinal analysis. American Journal of Public Health. 2006;96:1265–1270. doi: 10.2105/AJPH.2005.064543. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smith TW, Ruiz JM, Uchino BN. Vigilance, active coping, and cardiovascular reactivity during social interaction in young men. Health Psychology. 2000;19:382–392. doi: 10.1037//0278-6133. [DOI] [PubMed] [Google Scholar]
- Szymanski DM, Stewart DN. Racism and sexism as correlates of african American women’s psychological distress. Sex Roles. 2010;63:226–238. doi: 10.1007/s11199-010-9788-0. [DOI] [Google Scholar]
- Taylor TR, Kamarck TW, Shiffman S. Validation of the Detroit area study discrimination scale in a community sample of older African American adults: The Pittsburgh healthy heart project. International Journal of Behavioral Medicine. 2004;11:88–94. doi: 10.1207/s15327558ijbm1102_4. [DOI] [PubMed] [Google Scholar]
- Utsey SO, Payne YA, Jackson ES, Jones AM. Race-related stress, quality of life indicators, and life satisfaction among elderly African Americans. Cultural Diversity & Ethnic Minority Psychology. 2002;8:224–233. doi: 10.1037//1099-9809.8.3.224. [DOI] [PubMed] [Google Scholar]
- Wei M, Heppner PP, Ku TY, Liao KYH. Racial discrimination stress, coping, and depressive symptoms among Asian Americans: A moderation analysis. Asian American Journal of Psychology. 2010;1:136–150. doi: 10.1037/a0020157. [DOI] [Google Scholar]
- Williams DR. Race, socioeconomic status, and health the added effects of racism and discrimination. Annals of the New York Academy of Sciences. 1999;896:173–188. doi: 10.1111/j.1749-6632.1999.tb08114.x. [DOI] [PubMed] [Google Scholar]
- Williams DR, Mohammed SA. Discrimination and racial disparities in health: Evidence and needed research. Journal of Behavioral Medicine. 2009;32:20–47. doi: 10.1007/s10865-008-9185-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Williams DR, Neighbors HW, Jackson JS. Racial/ethnic discrimination and health: Findings from community studies. American Journal of Public Health. 2008;98:S29–S37. doi: 10.2105/AJPH.93.2.200. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Williams DR, Yu Y, Jackson JS, Anderson NB. Racial differences in physical and mental health: socio-economic status, stress and discrimination. Journal of Health Psychology. 1997;2:335–351. doi: 10.1177/135910539700200305. [DOI] [PubMed] [Google Scholar]