

Abstract
Pancreatic tumors with osteoclast-like giant cells are rare, with only 50 cases published to date. We report a case of a 67-year-old male with a new diagnosis of follicular non-Hodgkin's lymphoma with an incidental pancreatic body mass on abdominal imaging. Cytology from the pancreatic mass obtained via endoscopic ultrasound-directed fine-needle aspiration (EUS-FNA) revealed an undifferentiated carcinoma with osteoclast-like giant cells.
Introduction
Undifferentiated carcinoma with osteoclast-like giant cells (UCWOGC) is a rare abdominal tumor that is estimated to account for 1% of pancreatic tumors.1,2 Although this cytologic variant has been identified in other tissues such as the skin, thyroid gland, ovary, and breast,3 it has been most commonly reported in the pancreas and was first described by Rosai in 1968.1,4 The tumor is often found on imaging and typically appears as a large heterogeneous mass with well-demarcated hyper- and hypoechoic areas that represent necrotic areas and cystic structures, respectively.1,5 About 50 reports of this tumor have been described, and most have been in Asia.6
Case Report
A 67-year-old Caucasian male presented with a non-tender, submandibular “lump.” He reported no fatigue, night sweats, weight loss, or abdominal pain. His past medical history was unremarkable. The clinical examination revealed an enlarged submandibular lymph node and tenderness in the right upper abdominal quadrant. Biopsy of the submandibular lymph node showed pathology consistent with follicular non-Hodgkin's lymphoma. He then underwent treatment with rituxan and bendamustine. A PET scan performed to stage the patient's lymphoma showed focal fluoro-2-deoxy-d-glucose (FDG) uptake in the body of the pancreas. An MRI revealed a multi-locular cystic mass with multiple intralesional septations in the pancreatic body; endoscopic ultrasound revealed a 4.9 × 4.1-cm solid mass in the body of the pancreas with anechoic complex structures and a regular border without vascular involvement (Figure 1). EUS-FNA with 4 aspiration passes obtained a specimen that consisted of atypical spindle cells admixed with multi-nucleated giant cells (Figure 2). The spindle cells were positive for CAM 5.2 and vimentin. The giant cells were positive for CD68. The morphology and immunohistologic profile supported a diagnosis of UCWOGC in the setting of grade III intraductal papillary mucinous neoplasm with no ovarian-type stroma.
Figure 1.
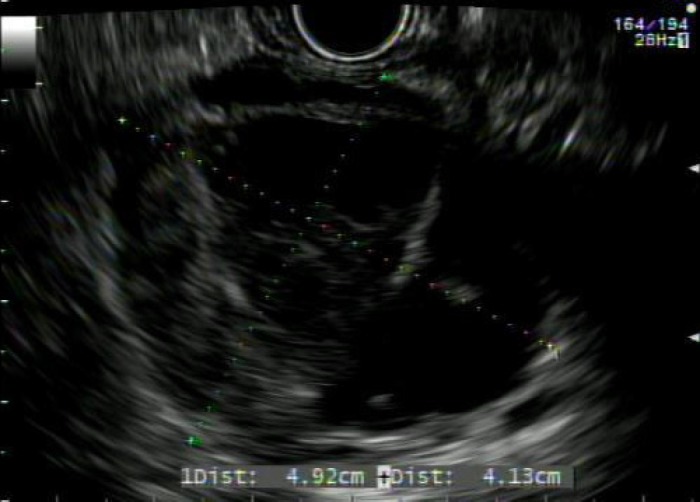
EUS showing a 4.9 × 4.1-cm solid pancreatic body mass with anechoic complex structures.
Figure 2.
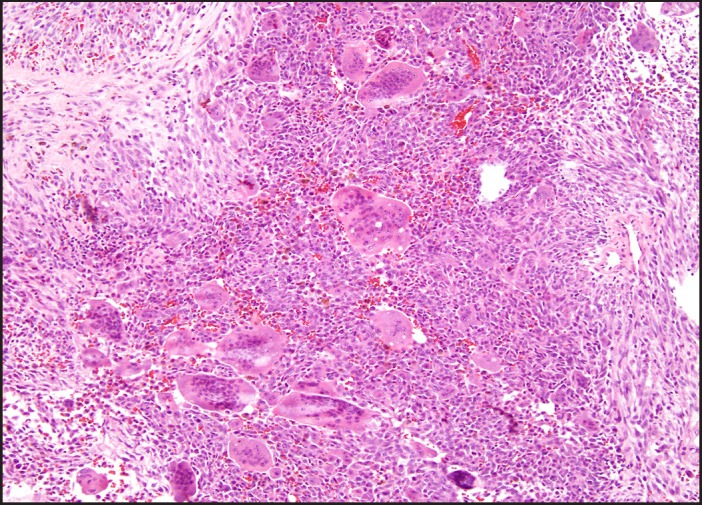
Surgical pathology shows marked nuclear atypia of the mononuclear cells. The osteoclast-like giant cells have bland nuclear features. The mononuclear cells of this tumor show large vesicular nuclei with prominent nucleoli.
The patient underwent a radical distal pancreatectomy and pathology was consistent with UCWOGC (Figure 2).
The gross specimen appeared as an 11 × 5.5 × 4-cm mass with a focally softened solid portion and a portion of multiple smooth-walled cysts containing mucoid material. The patient did well postoperatively without adjuvant chemotherapy.
Discussion
UCWOGC is a classified by the World Health Organization as a rare variant of ductal adenocarcinoma7 with two distinct cell lines, including a mononuclear cell line population and osteoclastic tumor cells.1 The tumor is further described by the Stanford Surgical Pathology Criteria as multinucleated giant cells with malignant background cells.8 Due to the poor differentiation of the underlying tumor cells, it is unclear where these neoplastic cells originate. Many authors favor an epithelial origin while others favor a mesenchymal origin.2,9
UGWOGC is thought to have an equal male–female predominance with an average age of incidence around 60 years.1 The presentation is variable depending on the location of the tumor within the pancreas; pancreatic head masses present with jaundice and weight loss, and pancreatic body and tail tumors present with abdominal pain.7 Patients typically present with advanced disease. Imaging, including abdominal ultrasound, CT, and MRI are used for diagnosis of these tumors. These masses are typically further evaluated by EUS-FNA of the mass, as in this case, or through mass resection. In patients with UCWOGC, numerous reports have shown that treatment choice is resection if possible,6 though resection can rarely be performed since the disease typically presents in advanced stage.
The prognosis of UCWOGC is poor, but it is better than that of ductal carcinomas and pleomorphic giant cell tumors of the pancreas. In some studies, 10-year survival with UGWOGC has been reported, which shows that this tumor may have a better prognosis than undifferentiated carcinoma of the pancreas without osteoclast-like giant cells.11,12 In general, the average survival has been shown to be about only 20 months.10 There have been trials investigating the use of chemotherapeutic agents, such as gemcitabine, but no conclusive evidence has been found to indicate their use.
Disclosures
Author contributions: All the authors were responsible for literature search, drafting the manuscript, and giving final approval. AA Siddiqui is the article guarantor.
Financial disclosure: The authors attest that they have no commercial associations that might be a conflict of interest in relation to the submitted manuscript.
Informed consent was obtained for this manuscript.
References
- 1.Bauditz J, Rudolph B, Wermke W. Osteoclast-like giant cell tumors of the pancreas and liver. World J Gastroenterol. 2006;12(48):7878–83. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Sivanandham S, Subashchandrabose R, Muthusamy KR. FNA diagnosis of osteoclast-like giant cell tumor of the pancreas. J Cytol. 2012;29(4):270–272. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Wada T, Itano O, Oshima G, et al. . A male case of an undifferentiated carcinoma with osteoclast-like giant cells originating in an indeterminate mucin-producing cystic neoplasm of the pancreas. A case report and review of the literature. World J Surg Oncol. 2011;9:100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Rosai J. Carcinoma of the pancreas simulating giant cell tumor of bone. Electron-microscopic evidence of its acinar cell origin. Cancer. 1968;22(2):333–44. [DOI] [PubMed] [Google Scholar]
- 5.Moore JC, Bentz JS, Hilden K, Adler DG. Osteoclastic and pleomorphic giant cell tumors of the pancreas: A review of clinical, endoscopic, and pathologic features. World J Gastrointest Endosc. 2010;2(1):15–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Hur YH, Kim HH, Seoung JS, et al. . Undifferentiated carcinoma of the pancreas with osteoclast-like giant cells. J Korean Surg Soc. 2011;81(2):146–150. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Togawa Y, Tonouchi A, Chiku T, et al. . A case report of undifferentiated carcinoma with osteoclast-like giant cells of the pancreas and literature review. Clin J Gastroenterol. 2010;3(4):195–203. [DOI] [PubMed] [Google Scholar]
- 8.Rouse R. Undifferentiated carcinoma with osteoclast-like giant cells of the pancreas. Stanford School of Medicine Surgical Pathology Criteria Web site. http://surgpathcriteria.stanford.edu/pancreas/unifferentiated_carcinoma_osteoclast_like_giant_cells_pancreas Published January 5, 2008. Updated January 5, 2012 Accessed October 15, 2013.
- 9.Goldberg RD, Michelassi F, Montag AG. Osteoclast-like giant cell tumor of the pancreas: Immunophenotypic similarity to giant cell tumor of bone. Hum Pathol. 1991;22(6):618–622. [DOI] [PubMed] [Google Scholar]
- 10.Nai GA, Amico E, Gimenez VR, Guilmar M. Osteoclast-like giant cell tumor of the pancreas associated with mucus-secreting adenocarcinoma. Case report and discussion of the histogenesis. Pancreatology. 2005;5(2–3):279–84. [DOI] [PubMed] [Google Scholar]
- 11.Shimosegawa T, Saegusa S, Sekoguchi T, et al. . Anaplastic ductal carcinoma of the pancreas with more than 10 year postoperative survival: Report of 3 cases. Pancreas. 2006;33(1):88–9. [Google Scholar]
- 12.Deckard-Janatpour K, Kragel S, Teplitz RL, et al. . Tumors of the pancreas with osteoclast-like and pleomorphic giant cells: Immunohistochemical and ploidy study. Arch Pathol Lab Med. 1998;122:266–72. [PubMed] [Google Scholar]