

Abstract
Recent exponential increase in inferior vena cava (IVC) filter placements has led to a higher rate of filter complications. A 46-year-old man with a past history of IVC filter placement for bilateral deep vein thrombosis presented with lower abdominal pain. Imaging studies demonstrated IVC filter strut penetrations into multiple structures. Upper endoscopy confirmed an uncomplicated single IVC filter strut penetration into the duodenal wall. The abdominal pain was determined to be unrelated to IVC filter strut penetration, and the patient was managed conservatively. Although IVC filter strut penetrations can cause significant complications, current guidelines remain unclear for management of asymptomatic enteric IVC filter strut penetrations.
Introduction
Over the last decade, inferior vena cava (IVC) filter placement has increased dramatically. Complications due to IVC filter include perforation of the aorta, the psoas muscles, and the gastrointestinal (GI) tract.1,2 These perforations are exceedingly rare and usually symptomatic.3 Existing literature describes cases of symptomatic duodenal perforations from IVC filters managed by surgical procedures.2 However, there is a paucity of literature on the treatment of asymptomatic penetrations. We present a patient with an asymptomatic duodenal penetration by an IVC filter.
Case Report
A 46-year-old man with a history of paraplegia from prior trauma, bilateral lower extremity thrombus, and placement of an IVC filter 6 years ago underwent a computed tomography (CT) for evaluation of lower abdominal pain. The patient also complained of daytime urinary frequency, incontinence, nocturia, urgency, and weak urinary stream, and had evidence of microscopic hematuria. The CT scan was remarkable for IVC filter strut penetrations into the right psoas muscle, L3 vertebral body, and possibly the duodenum (Figure 1). The patient denied symptoms of GI bleeding and a complete blood count was unremarkable. An esophagogastroduodenoscopy (EGD) confirmed a single IVC filter strut penetrating into the second part of the duodenal wall. The intraluminal strut measured 1.5 cm in length, and the end of the strut was hooked, providing a soft end (Figure 2). There was no ulceration or bleeding at the site of penetration. The vascular surgeons felt that the potential complications from IVC filter removal would outweigh the benefits in an otherwise asymptomatic patient. Meanwhile, laboratory evaluation revealed that the patient had a urinary tract infection, and urology service diagnosed benign hypertrophy of prostate. His abdominal pain was attributed to this cause. He was started on tamsulosin with antibiotics and later reported resolution of lower abdominal pain and urological symptoms. After 1 year of follow-up, the patient remains asymptomatic and free of complications secondary to duodenal penetration by the IVC filter.
Figure 1.
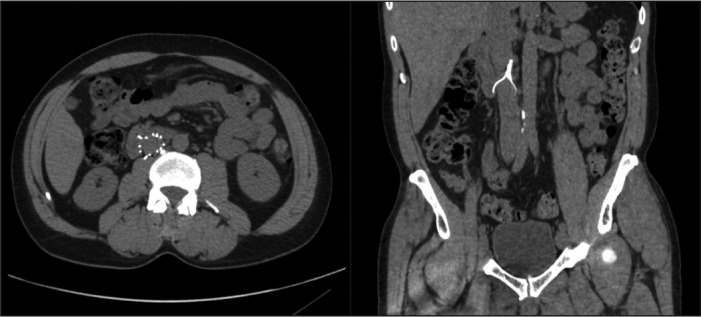
Abdominal CT showing IVC filter struts penetrating the duodenum and right psoas muscle.
Figure 2.
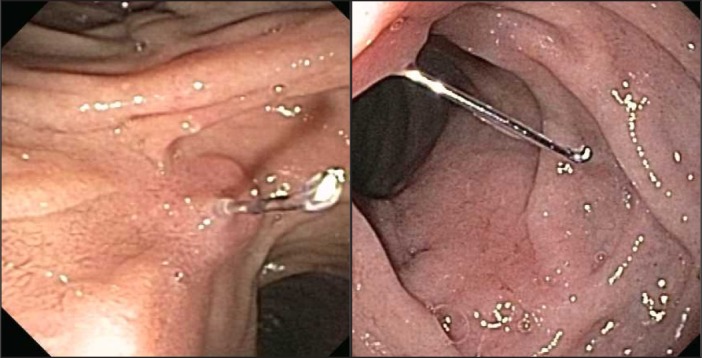
EGD showing an IVC filter strut perforating through the wall of the duodenum.
Discussion
Caval filters are classified by their anatomical site: infrarenal or suprarenal. Further categories include permanent filters (indicated for patients with life-long risk of pulmonary embolism) or retrievable/optional filters (for perioperative use).4 The optional filters have a retrieval hook facilitating easy removal, and the majority of filters currently being used are the retrievable type.4 Interventional radiology guidelines list access site thromboses, IVC occlusions, and IVC penetration as the most frequently reported complications. Other complications include filter movement and tilt, fracture or embolization, deployment outside the target area, and recurrent pulmonary embolism.5 Filter tilt is the resultant angulation after insertion and is usually minimal after placement in the IVC. A tilt of >15° away from the long axis of the IVC reduces efficacy and predisposes to caval perforation. To reduce risk of filter tilt, manufacturers have implemented ‘hooks’ and ‘legs’ at the end of the filter.4 The overall incidence of filter perforation through the IVC wall is approximately 0.3%.6
Currently, there are no guidelines for the management of patients with asymptomatic IVC filter penetrations into the duodenum. As the risks of removing the filter overweigh the any likely benefits in such cases, asymptomatic patients require a multidisciplinary approach involving interventional radiology, gastroenterology, and vascular surgery, and a closely monitored non-operative follow-up. In symptomatic patients, removal of the filter is difficult due to exposure of the IVC bounded by inflammatory reaction, so surgical treatment is recommended only after definitive failure of conservative management and if symptom relief is certain.7 When removal is contemplated, CT and EGD should be used to evaluate filter strut penetrations, and an open procedure by exploratory laparotomy is the typical removal technique. Venotomy is performed to remove the filter, and if the filter struts are not extractable, they should be trimmed with wire cutters.7 In our patient, a non-surgical approach was successfully adopted for the management of IVC filter strut penetration through the duodenal wall.
Disclosures
Author contributions: JR Park and VM Oza completed the literature review and wrote the manuscript. SG Krishna participated in clinical management of the patient, reviewed the manuscript, and is the author guarantor.
Financial disclosure: None to report.
Informed consent was obtained for this case report.
References
- 1.DuraiRaj R, Fogarty S. A penetrating inferior vena caval filter. Eur J Vasc Endovasc Surg. 2006;32(6):737–9. [DOI] [PubMed] [Google Scholar]
- 2.Vandy F, Rectenwald JE, Criado E. Late gastrointestinal complications of inferior vena cava filter placement: Case report and literature review. Perspect Vasc Surg Endovasc Ther. 2011;23(4):261–4. [DOI] [PubMed] [Google Scholar]
- 3.Malgor RD, Hines GL, Terrana L, Labropoulos N. Persistent abdominal pain caused by an inferior vena cava filter protruding into the duodenum and the aortic wall. Ann Vasc Surg. 2012;26(6):858.e3–6. [DOI] [PubMed] [Google Scholar]
- 4.Harvey JJ, Hopkins J, McCafferty IJ, Jones RG. Inferior vena cava filters: What radiologists need to know. Clin Radiol. 2013;68(7):721–2. [DOI] [PubMed] [Google Scholar]
- 5.Caplin DM, Nikolic B, Kalva SP, et al. Quality improvement guidelines for the performance of inferior vena cava filter placement for the prevention of pulmonary embolism. J Vasc Interv Radiol. 2011;22(11):1499–1506. [DOI] [PubMed] [Google Scholar]
- 6.Bogue CO, John PR, Connolly BL, et al. Symptomatic caval penetration by a Celect inferior vena cava filter. Pediatr Radiol. 2009;39(10):1110–3. [DOI] [PubMed] [Google Scholar]
- 7.Malgor RD, Hines GL, Terrana L, Labropoulos N. A systematic review of symptomatic duodenal perforation by inferior vena cava filters. J Vasc Surg. 2012;55(6):856–61.e3. [DOI] [PubMed] [Google Scholar]