

Abstract
In the absence of overt structural abnormalities, the diagnostic approach to chronic abdominal pain can be challenging. Occupational particulate inhalation causing injury to an organ other than the lung is rare. We report a case of inadvertent glass microparticulate ingestion causing chronic abdominal pain with altered local and systemic inflammatory responses.
Introduction
Occupational particulate inhalation causing injury in an organ other than the lung is rare, and when present, can be difficult to diagnose.1,2 We report a case of inadvertent glass microparticulate ingestion causing chronic abdominal pain with altered local and systemic inflammatory responses. We also describe the specialized etiologic evaluation, including x-ray microanalysis, immunohistochemistry, and peripheral blood assays, that were used to confirm the diagnosis, and suggest that altered local and systemic inflammatory response might be responsible.
Case Report
The patient is a previously healthy 38-year-old man who developed chronic recurrent abdominal pain after starting work as a manager at a glass-cutting factory. He was present on the factory floor while glass was being cut, ground, and smoothed, and did not routinely use protective gear. The abdominal pain was episodic, periumbilical, lasted several days, and would resolve spontaneously. He was asymptomatic between episodes.
Physical exam was unremarkable both during and between pain episodes. An extensive laboratory work-up revealed only a mildly elevated C-reactive protein. Blood counts, electrolytes, liver and kidney function, thyroid tests, and iron studies were normal. Blood cultures were negative. Testing for HIV, C1 esterase, complement levels, porphyrins, heavy metals, and paroxysmal nocturnal hemoglobinuria was unrevealing. Upper endoscopy, colonoscopy, and capsule endoscopy were non-diagnostic. Abdominal CT during a pain flare showed mild thickening in the appendix and mesenteric stranding with sub-centimeter lymph nodes. Diagnostic laparoscopy revealed vermiform-appearing adhesions on the abdominal wall (Figure 1). Mesenteric biopsy showed chronic inflammation with evidence of foreign body reaction (Figure 2).
Figure 1.
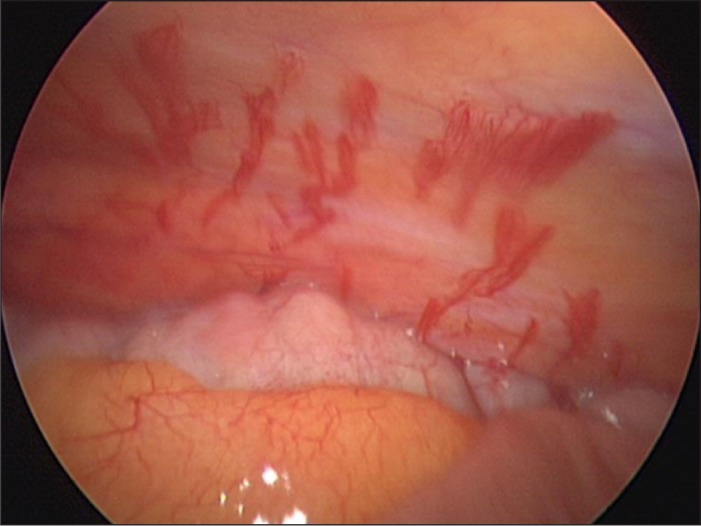
Intraoperative laparoscopic image showing unusual-appearing vermiform lesions in the right lateral abdominal sidewall with thin adherent omentum.
Figure 2.
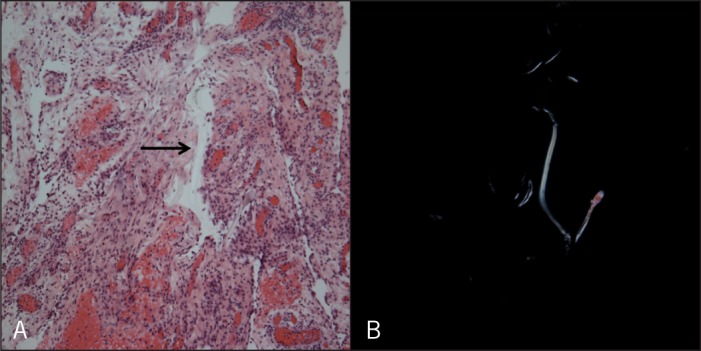
Histopathologic findings on examination of mesenteric biopsy specimens (40×). (A) Hematoxylin and eosin stain showing papillary mesothelial hyperplasia with the presence of a refractile foreign body (arrow). (B) The foreign body material is clearly illustrated when viewed under polarized light.
To investigate these histopathologic findings in more detail, specialized testing was performed. X-ray microanalysis revealed the presence of silicon (Figure 3), silver chloride, tungsten, titanium, and vanadium, which are metals commonly used in glass manufacturing. On immunohistochemistry, there was scant staining for IL-1ß. Lipopolysaccharide (LPS)-induced IL-1ß protein secretion was also significantly lowered in this patient compared to healthy controls (Figure 4).
Figure 3.
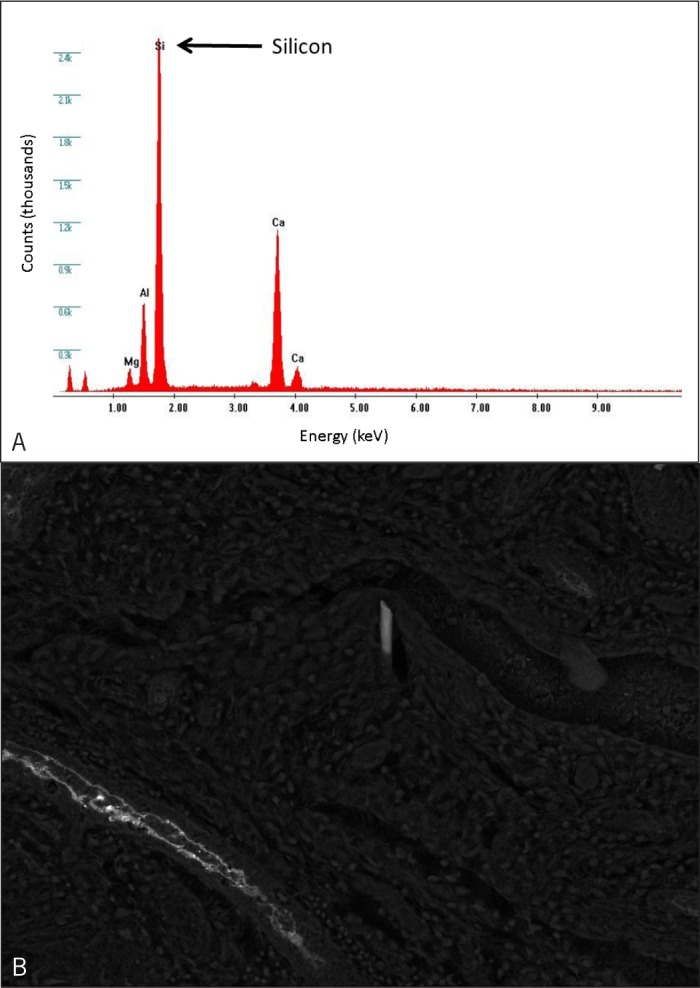
Results of specialized testing with x-ray microanalyses. (A) High levels of silicon are demonstrated in the x-ray microanalysis from the biopsy specimen. The energy applied, measured in keV, is on the x axis, and the resulting counts are on the y axis. (B) An electron microscopy image of the silicon foreign body.
Figure 4.
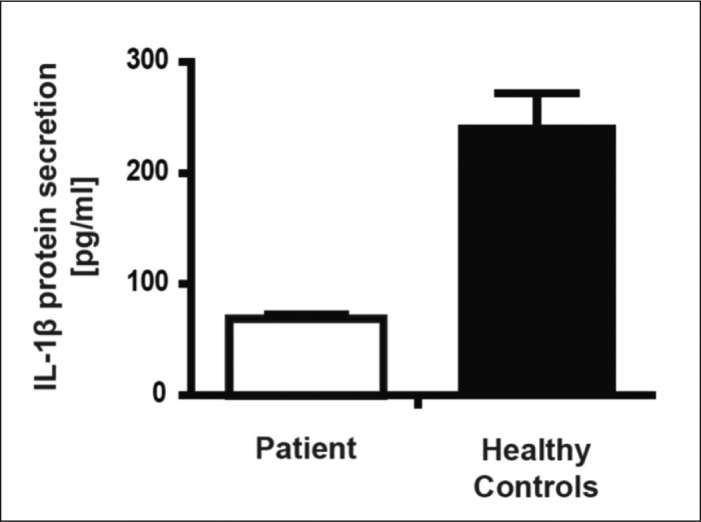
White blood cells from the patient display impaired LPS-induced IL-lB protein secretion compared to healthy controls (n=3). Error bars represent the standard deviation of the measurements (each experiment was performed in triplicate for each of the samples).
On clinical follow-up of 3 years, exposure avoidance with a respirator mask at work led to significant symptom improvement, and lapses in exposure avoidance led to recurrent symptoms.
Discussion
Occupational particulate ingestion causing inhalational lung injury is well reported. However, particulate involvement of other organ systems is rare, and the clinical significance of such exposures is not well understood.1–2 The inflammatory response and cellular changes generated by foreign body reaction have been recently reported for inhalational exposures in coal miners, ship-builders, and glass manufacturers.3–6 Ferrira et al described a glass laminator with inflammatory lung granulomas consisting of silica-predominant particulate.7 However, only 1 report has described similar exposures involving the GI tract in “glass dust esophagitis” in a glass grinder who presented with chest pain.8
Dysfunction of the intestinal inflammasome, particularly with altered levels of cytokines such as IL-1ß, may contribute to many gastrointestinal conditions, including inflammatory bowel disease, colon cancer, and functional bowel disorders.9 In our patient, we detected a number of mesenteric glass microparticulates suggestive of inadvertent ingestion and subsequent microperforation. We also found lower IL-1B levels locally in mesenteric tissue and systemically with blunted IL-1ß secretion after LPS stimulation. There is evidence that silica can suppress murine macrophage production of the pro-inflammatory cytokines IL-1 and IL-6,3 and this mechanism provides a possible explanation for our findings. IL-lB receptors are now therapeutic targets for novel immunomodulatory medications such as anakinra, an IL-lB receptor antagonist.10,11 A side effect of this medication is chronic abdominal pain; in theory, excess inhibition resulting in reduced IL-1ß levels may contribute to abdominal pain.
We hypothesize that inadvertent glass microparticulate ingestion and microperforation led to a silica-induced impairment of IL-1ß secretion and subsequent chronic inflammation and pain. It is important to consider occupational exposures in patients with unexplained chronic gastrointestinal complaints that do not fit with symptom patterns in other established disorders.
Disclosures
Author contributions: RB Vance collected and interpreted data, and drafted, critically revised, and approved the manuscript. M. Mühlbauer collected, interpreted, and analyzed data, and critically revised and approved the manuscript. EB Dreesen provided patient care and critically revised and approved the manuscript. CR Bagnell and GA Dent provided pathologic analysis and interpretation, and critically revised and approved the manuscript. H. Herfarth and C. Jobin designed the study, interpreted data, and critically revised and approved the manuscript. ES Dellon designed the study, provided patient care, collected and interpreted data, drafted, critically revised, and approved the manuscript, and is the article guarantor.
Financial disclosure: None to report.
Informed consent was obtained for this case report.
Previous Presentation: This paper was presented as a poster at the 2012 ACG Annual Meeting.
References
- 1.Gerhardsson de Verdier M, Plato N, Steineck G, Peters JM. Occupational exposures and cancer of the colon and rectum. Am J Ind Med. 1992;22(3):291–303. [DOI] [PubMed] [Google Scholar]
- 2.Bunderson-Schelvan M, Pfau JC, Crouch R, Holian A. Nonpulmonary outcomes of asbestos exposure. J of Toxicol Environ Health B Crit Rev. 2011;14(1–4):122–52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Hwang M, Park KK, Chang YC, et al. Silica-ceramic suppresses the expression of pro-inflammatory cytokines induced by lipopolysaccharide macrophages. J Biomed Mater Res A. 2007;80(3):513–9. [DOI] [PubMed] [Google Scholar]
- 4.Castranova V, Vallyathan V. Silicosis and coal workers' pneumoconiosis. Environ Health Perspect. 2000;108(suppl 4):675–84. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Hedly-Whyte J, Milamed DR. Asbestos and ship-building: Fatal consequences. Ulster Med J. 2008;77(3):191–200. [PMC free article] [PubMed] [Google Scholar]
- 6.Ji X, Hou Z, Wang T, et al. Polymorphisms in inflammasome genes and risk of workers' pneumoconiosis in a Chinese population. PLoS One. 2012;7(10):. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Ferriera AS, Moreira VB, Castro MC, et al. Case report: Analytical electron microscopy of lung granulomas associated with exposure to coating materials carried by glass wool fibers. Environ Health Perspect. 2010;118(2):249–52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Park HS, Han DS, Bae JH. Glass dust esophagitis: An unusual cause of chest pain. Gastrointest Endosc. 2012;75(3):668. [DOI] [PubMed] [Google Scholar]
- 9.Chen GY, Núñez G. Inflammasomes in intestinal inflammation and cancer. Gastroenterology. 2011;141(6):1986–99. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Marchand F, Perreti M, McMahon SB. Role of the immune system in chronic pain. Nat Rev Neurosci. 2005;6(7):521–32. [DOI] [PubMed] [Google Scholar]
- 11.McDermott MF. Rilonacept in the treatment of chronic inflammatory disorders. Drugs Today (Barc). 2009;45(6):423–30. [DOI] [PubMed] [Google Scholar]