

Abstract
Portal hypertension leading to gastric polyposis has rarely been reported. More common gastric manifestations of portal hypertension are portal hypertensive gastropathy and gastric antral vascular ectasia (GAVE). We report a case of a patient in whom portal hypertension manifested as bleeding gastric polyps leading to transfusion-dependent iron deficiency anemia.
Introduction
Gastric polyps can occur in various settings, such as chronic proton pump inhibitor (PPI) use,1,2 chronic inflammation, infection from Helicobacter pylori, peptic ulcers, at sites of gastroenterostomies,3 secondary to prior argon plasma coagulation (APC) treatments,4,5 or as part of familial polyposis syndromes. Portal hypertension leading to gastric polyposis has rarely been reported.6
Case Report
A 64-year-old white woman with a history of diabetes mellitus, hypertension, hyperlipidemia, obesity (body mass index [BMI] 33 kg/m2), and compensated non-alcoholic steatohepatitis (NASH) cirrhosis presented for evaluation of recent onset iron-deficiency anemia. She had fatigue and shortness of breath. Her anemia was unresponsive to oral and IV iron therapy and required almost monthly blood transfusions. Esophagogastroduodenoscopy (EGD), colonoscopy, and capsule endoscopy were significant for mild portal hypertensive gastropathy without esophageal or gastric varices. Laboratory values showed a microcytic anemia, with mean corpuscular volume 70.3 fL, nadir hemoglobin 7.3 g/dL, ferritin 17.9 ng/mL, AST 183 U/L, ALT 153 U/L, BUN 15 mg/dL, creatinine 0.70 mg/dL, and INR 1.1. Calculated Model For End-Stage Liver Disease (MELD) score was 7.
Repeat EGD showed multiple bleeding gastric polyps and severe portal hypertensive gastropathy (Figure 1). Histopathology of the removed polyps (Figure 2) demonstrated the presence of a hyperplastic epithelium and an edematous lamina propria containing prominent ectatic blood vessels, many of which had a smooth muscle layer. There was absence of fibrin thrombi in the vessels within the polyp. She was treated with endoscopic mucosal resection of the polyps. Subsequently, she developed gastric antral vascular ectasia (GAVE), for which she received APC treatments. She was lost to follow-up after moving from the area.
Figure 1.
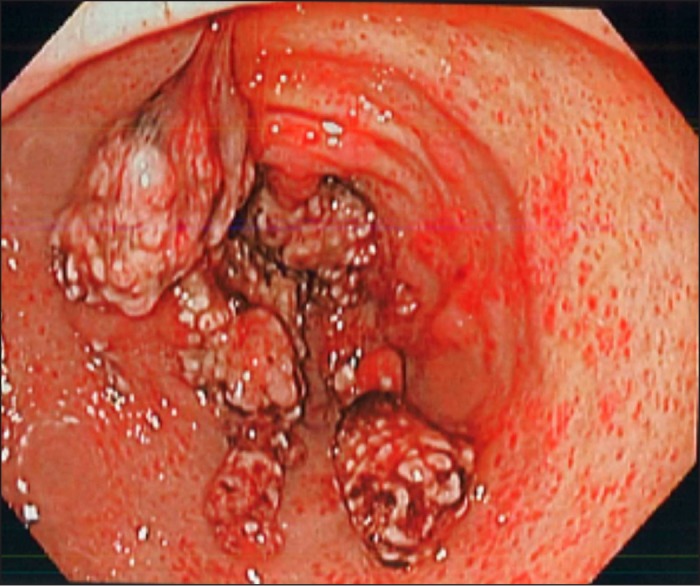
Multiple bleeding gastric polyps and severe portal hypertensive gastropathy.
Figure 2.
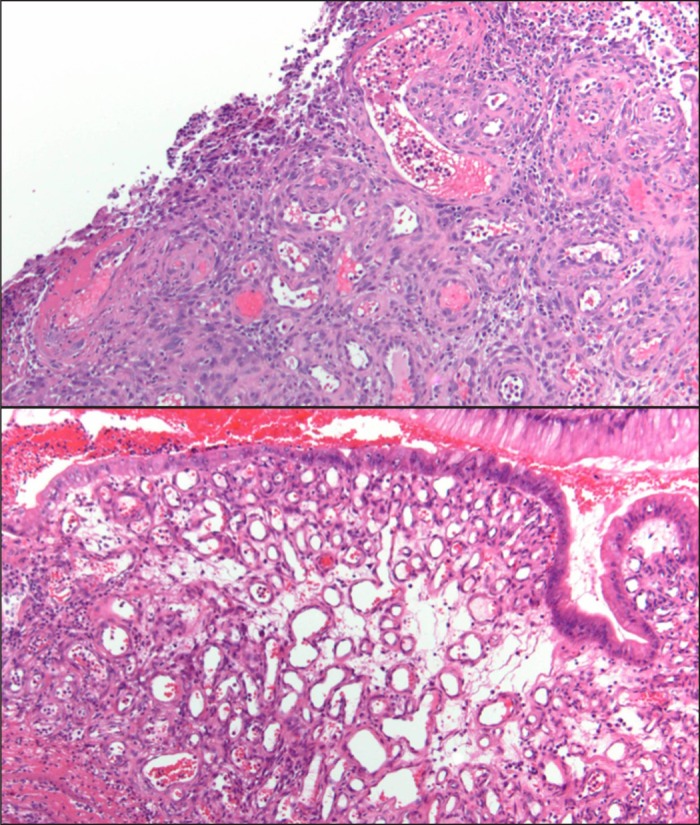
Histopathology of the removed polyps showing hyperplastic epithelium and an edematous lamina propria containing prominent ectatic blood vessels, many of which had a smooth muscle layer.
Discussion
Gastric polyps are seen in about 6% of upper gastrointestinal endoscopies in the United States,1 with fundic polyps being more common due to widespread use of PPIs1,2 and a relatively lower prevalence of Helicobacter pylori infection than in other countries.7,8 Lam et al found that gastric hyperplastic polyps in patients with portal hypertension exhibited a unique histology showing prominent capillary ectasia in an edematous lamina propria when compared to polyps in patients without portal hypertension.6
Endoscopic appearance alone cannot distinguish between hyperplastic gastric polyps, gastric polyps secondary to portal hypertension, and the nodular subtype of GAVE.9 The presence of histologic features such as prominent capillary ectasia in an edematous lamina propria without of histologic features suggestive of nodular GAVE suggests that these polyps are a distinct entity. The presence of a smooth muscle layer in many of these vessels also suggests that the formation of gastric polyps was a direct consequence of the patient's portal hypertension, leading to congestion in the gastric wall. These unique histologic features distinguish these polyps from hyperplastic polyps that occur in the setting of PPI use, which may appear to be a confounding factor for our patient. It is not known whether these polyps develop secondary to congestion from increased pressure or angioneogenesis in the gastric mucosa, or a combination of both factors. The natural course of such polyps, molecular mechanisms leading to their development and/or recurrence, and similarities/dissimilarities from polyps elsewhere in the gastrointestinal tract are also not known. It is also unclear whether these polyps have underlying malignant potential or if they eventually regress with the reduction of portal pressures after the placement of a transjugular intrahepatic portosystemic shunt (TIPS).
Disclosures
Author contributions: SJS Nagpal, C. Macaron, and N. Alkhouri designed the study, acquired and analyzed the data, and drafted and critically revised the manuscript. RK Pai acquired and analyzed the data, and drafted and critically revised the manuscript. N. Alkhouri supervised the study and is the article guarantor.
Financial disclosure: None to report.
Informed consent was obtained for this case report.
References
- 1.Carmack SW, Genta RM, Schuler CM, Saboorian MH. The current spectrum of gastric polyps: A 1-year national study of over 120,000 patients. Am J Gastroenterol. 2009;104(6):1524–32. [DOI] [PubMed] [Google Scholar]
- 2.Jalving M, Koornstra JJ, Wesseling J, et al. Increased risk of fundic gland polyps during long-term proton pump inhibitor therapy. Aliment Pharmacol Ther. 2006;24(9):1341–8. [DOI] [PubMed] [Google Scholar]
- 3.Dirschmid K, Platz-Baudin C, Stolte M. Why is the hyperplastic polyp a marker for the precancerous condition of the gastric mucosa? Virchows Arch. 2006;448(1):80–4. [DOI] [PubMed] [Google Scholar]
- 4.Izquierdo S, Rey E, Gutiérrez Del Olmo A, et al. Polyp as a complication of argon plasma coagulation in watermelon stomach. Endoscopy. 2005;37(9):921. [DOI] [PubMed] [Google Scholar]
- 5.Baudet JS, Salata H, Soler M, et al. Hyperplastic gastric polyps after argon plasma coagulation treatment of gastric antral vascular ectasia (GAVE). Endoscopy. 2007;39( 1 suppl): E320. [DOI] [PubMed] [Google Scholar]
- 6.Lam MCW, Tha S, Owen D, et al. Gastric polyps in patients with portal hypertension. Eur J Gastroenterol Hepatol. 2011;23(12):1245–9. [DOI] [PubMed] [Google Scholar]
- 7.Archimandritis A, Spiliadis C, Tzivras M, et al. Gastric epithelial polyps: A retrospective endoscopic study of 12974 symptomatic patients. Ital J Gastroenterol. 1996;28(7):387–90. [PubMed] [Google Scholar]
- 8.Morais DJ, Yamanaka A, Zeitune JMR, Andreollo NA. Gastric polyps: A retrospective analysis of 26,000 digestive endoscopies. Arq Gastroenterol. 2007;44(1):14–7. [DOI] [PubMed] [Google Scholar]
- 9.Marsteller WF, Lewin DN, Reuben A. The biopsy GAVE the diagnosis. Clin Gastroenterol Hepatol. 2012;10(9):e75–76. [DOI] [PubMed] [Google Scholar]