

Abstract
Objectives:
Cephalometric norms of McNamara analysis have been studied in various populations due to their optimal efficiency. Dolphin cephalometric software greatly enhances the conduction of this analysis for orthodontic measurements. However, Dolphin is very expensive and cannot be afforded by many clinicians in developing countries. A suitable alternative software program in Farsi/English will greatly help Farsi speaking clinicians. The present study aimed to develop an affordable Iranian cephalometric analysis software program and compare it with Dolphin, the standard software available on the market for cephalometric analysis.
Materials and Methods:
In this diagnostic, descriptive study, 150 lateral cephalograms of normal occlusion individuals were selected in Mashhad and Qazvin, two major cities of Iran mainly populated with Fars ethnicity, the main Iranian ethnic group. After tracing the cephalograms, the McNamara analysis standards were measured both with Dolphin and the new software. The cephalometric software was designed using Microsoft Visual C++ program in Windows XP. Measurements made with the new software were compared with those of Dolphin software on both series of cephalograms. The validity and reliability were tested using intra-class correlation coefficient.
Results:
Calculations showed a very high correlation between the results of the Iranian cephalometric analysis software and Dolphin. This confirms the validity and optimal efficacy of the newly designed software (ICC 0.570–1.0).
Conclusion:
According to our results, the newly designed software has acceptable validity and reliability and can be used for orthodontic diagnosis, treatment planning and assessment of treatment outcome.
Keywords: Analysis, Software, Orthodontics, Cephalometry
INTRODUCTION
Cephalometric analysis is an important diagnostic tool for evaluation of dentofacial morphology. It provides a clear image of the skeletal changes that occur in the process of growth and treatment of patients.
Cephalometric parameters are measured and compared with standard values to assist in the diagnosis and classification of malocclusion. Software programs such as Dolphin Imaging Software were designed to assist in cephalometric techniques and are now commonly used by orthodontists worldwide. McNamara analysis has superior characteristics compared to other methods. It is based on natural head position (NHP) (Figure 1A) instead of Frankfort plane (Figure 1B), and therefore it establishes the true physiological horizontal plane. NHP has been found to be highly reproducible in adults and children, males and females, Caucasians and non-Caucasians, with a variance of only about 4°. Although NHP is not as precisely reproducible as orienting the head to Frankfort plane, the potential errors from lower reproducibility are smaller than those of accurate head orientation [1, 2].
Fig 1.
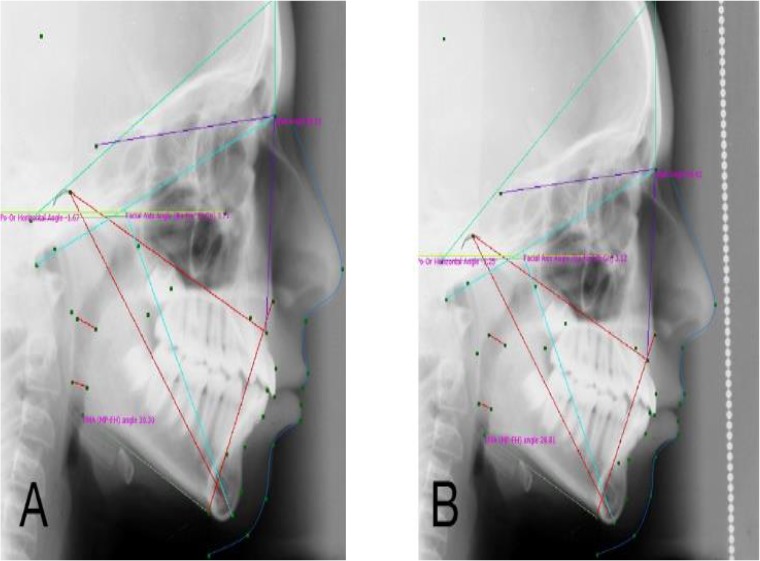
A traced cephalogram. A) a lateral cephalogram aquired in NHP, traced by designed software, B) a lateral cephalogram traced by designed software based on Frankfort plan.
McNamara analysis is also a very practical, applicable test that can be used by orthodontists for communication with colleagues, and for the definition and description of the structural relationships that are fundamental for diagnosis [3–5].
Significant differences exist in cephalometric standards among different ethnicities and the available cephalometric analysis software programs have all been designed based on standard norms of other ethnicities.
It may be beneficial for an ethnic group to have its own specific database due to ethnic differences. Qazvin and Mashhad are mainly populated with Fars ethnic group. Moreover, the software is available only in English and is expensive. Thus, there was a clear need for a software program specifically designed for Iranians for the above-mentioned reasons [6,7].
The present study aimed at designing a cephalometric analysis software program that could be comparable to Dolphin Imaging Software for the conduction of McNamara cephalometric analysis. The null hypothesis of this study was that the validity and reliability of our software would be the same as those of Dolphin.
MATERIALS AND METHODS
In this descriptive diagnostic study, a software program was designed based on the evaluation of 85 existing lateral cephalograms of patients residing in the city of Qazvin (42 females, 43 males) and 65 cephalograms of patients living in Mashhad (32 females and 33 males). These cephalograms were all obtained in NHP. To position the patients’ head in NHP, the subjects were asked to stare at the reflection of their own eyes in the mirror, placed at 5 feet from the cephalostat. This was true for both locations to reduce bias.
A total of 150 lateral cephalograms were traced by orthodontic instructors in Qazvin and Mashhad universities of Medical Sciences in a previous study. We obtained their results by first asking permission of the researchers of the aforementioned project [7,8]. Validity of Dolphin was approved by comparing its norms with those of hand-traced cephalograms [11]. The inclusion criteria of the patients were: normal occlusion (according to Moyers definition), proportionate facial profile (according to a panel of 2 orthodontists and 1 dentist), full dentition (except for third molars) and no history of previous orthodontic treatment or maxillofacial surgery.
The new software program was designed using Microsoft Visual C++ for Windows. The distance between two points was first calculated in pixels and then the user specified a 1-cm distance on the image and the distance in pixels was converted to millimeter (local patent number: 72900).
Obtained cephalograms were scanned by Microtek ScanMaker i800 scanner, 48-bit color and traced first by using Dolphin Imaging Software (version 10.5, Canoga Park, CA) (Figure 2) and then by the designed software (Figure 3). A dentist performed both tracings. The tracings were re-evaluated by an expert orthodontist and any error in identifying the landmarks was checked and corrected. Cephalograms based on NHP were analyzed using 10 linear and 3 angular variables from McNamara cephalometric analysis (Tables 1 and 2). The reliability of the understudy variables was measured to assess intra-examiner error; which was found to be 0.973–1. Cephalometric measurements made by the designed software were compared with those of Dolphin software using intra-class correlation coefficient (ICC). Type I error (α) was defined as 0.05 and thus, P<0.05 was considered statistically significant.
Fig 2.
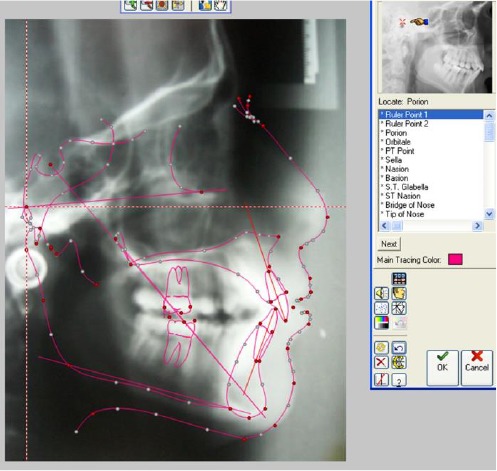
The traced cephalogram by Dolphin software.
Fig 3.
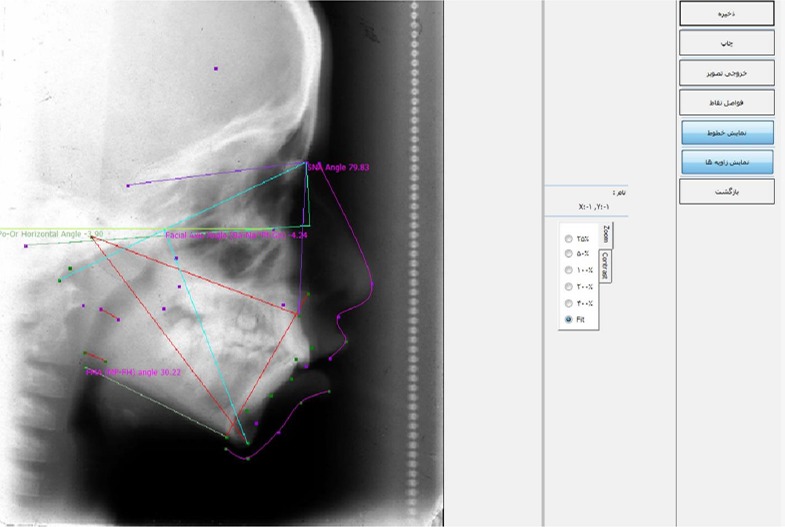
The traced cephalogram by our Designed software.
Table 1.
| Variables | Definition |
|---|---|
| Nasion (Na point) | The anterior point of the intersection between the nasal and frontal bones |
| Pogonion (Pog) | The most anterior point on the contour of the chin |
| S point | The midpoint of the cavity of sella turcica |
| U1 | Most facial aspect of Upper incisor in incisal edge |
| L1 | Most facial aspect of lower incisor in incisal edge |
| Gonion (Go) | The midpoint of the contour connecting the ramus and mandibular body |
| Gnathion (Gn) | The center of the inferior point on the mandibular symphysis |
| Anterior nasal spine (ANS) | The tip of the anterior nasal spine |
| A point | Innermost point on the contour of the premaxilla |
| Menton (Me) | The most inferior point on the mandibular symphysis |
| Condylon (Co) | The upper midpoint of the mandibular condyle |
| B point | Innermost point on the contour of the mandible |
| Pterygomaxillary fissure (PTM) | The point at the base of the fissure where the anterior and posterior walls meet |
Table 2.
| Na-A distance | Perpendicular distance between point A to Nasion |
| Pog-Na distance | Perpendicular distance from Pogonion to Na |
| SNA angle | Sella-Nasion-Point A angle |
| U1-A distance | Distance between the facial surface of upper incisor and a vertical line drawn through point A |
| L1-A distance | Distance between the edge of the incisors and a line drawn from point A-Pog |
| Upper airway space | Point on the posterior outline of the soft palate to the closest point on the pharyngeal wall |
| Lower airway space | Point of intersection of the posterior border of the tongue and the inferior border of the mandible to the closest point on the posterior pharyngeal wall |
| Lower Anterior Facial Height(LAFH) | Distance from ANS to Me |
| Mandibular length | Distance between Co-Gn |
| Mid-face length | Distance between Co-A point |
| Facial axial angle | Formed by a line constructed from PTM to Gn and the line perpendicular to the N point |
| Mandibular plane angle | Angle between the anatomic Frankfort horizontal plane and the line drawn along Go and Me |
| Maxillary and mandibular differentiation | Relationship between the mandibular length and midfacial length (Co-Gn)_(Co-A) |
RESULTS
When comparing the new software with Dolphin Imaging Software, the obtained results revealed highly reliable values for cephalometric analysis of patients residing in Qazvin city (Table 3). The ICC was between 0.562 for U1-A to 1 for most of the variables such as Pogonion-Nasion in females, mandibular length, lower anterior facial height and also for male midfacial length. Measuring the distance from the upper incisor to vertical line through point A (U1-A) was found to be the least reliable mainly due to the difficulty in landmark identification of point A. When comparing the reliability of the two software analyses, high correlations were also found in most of the cephalometric variables of Mashhad patients in the newly designed software (Table 4). The maximum and minimum reliability values were 1 and 0.815, respectively. The minimum value was again found for the distance between the upper incisor and vertical line through point A because of difficulty in finding the accurate position of this point and the tracing error. The maximum reliability was found in most of the variables such as lower anterior facial height and mandibular plane angle. Also, we did Bland-Altman analysis for one of the variables, SNA Angle, in Qazvin city samples. The graph displayed a scatter diagram of the differences plotted against the average of the two measurements. It is apparent from the graph that the means of both techniques are close to zero and most of the line lies within the confidence interval level and the points do not present any systematic error (Figure 4).
Table 3.
Intraclass correlation coefficients for comparison of different landmarks between our designed software and Dolphin software in Qazvin residents
| Landmark | ICC | ICC in females | ICC in males |
|---|---|---|---|
| Na-A distance | 0.997 | 0.997 | 0.996 |
| Pog-Na distance | 0.999 | 1.0 | 0.999 |
| SNA angle | 0.982 | 0.996 | 0.975 |
| U1-A distance | 0.570 * | 0.87 | 0.562 * |
| L1-A distance | 0.987 | 0.998 | 0.982 |
| Upper airway space | 0.993 | 0.987 | 0.997 |
| Lower airway space | 0.975 | 0.94 | 0.998 |
| LAFH | 0.992 | 0.975 | 1.0 |
| Mandibular length | 0.989 | 0.969 | 1.0 |
| Mid-face length | 0.988 | 0.972 | 1.0 |
| Facial axial angle | 0.986 | 0.972 | 0.994 |
| Mandibular plane angle | 0.982 | 0.957 | 0.998 |
| Maxillary and mandibular differentiation | 0.831 | 0.995 | 0.648 |
• Statistically significant difference
*LAFH Lower anterior facial height*ANS Anterior nasal spine
Table 4.
Intra-class correlation coefficients for comparison of different landmarks between our designed software and Dolphin software in Mashhad residents
| Landmarks | ICC | ICC in females | ICC in males |
|---|---|---|---|
| Na-A distance | 1.0 | 1.0 | 1.0 |
| Pog-Na distance | 1.0 | 1.0 | 1.0 |
| SNA angle | 0.999 | 1.0 | 0.997 |
| U1-A distance | 0.815 | 0.842 | 0.824 |
| L1-A distance | 0.999 | 1.0 | 0.999 |
| Upper airway space | 1.0 | 1.0 | 1.0 |
| Lower airway space | 1.0 | 1.0 | 0.999 |
| LAFH | 1.0 | 1.0 | 1.0 |
| Mandibular length | 0.841 | 0.822 | 0.830 |
| Mid-face length | 1.0 | 1.0 | 0.999 |
| Facial axial angle | 0.941 | 1.0 | 0.898 |
| Mandibular plane angle | 1.0 | 1.0 | 1.0 |
| Maxillary and mandibular differentiation | 1.0 | 1.0 | 0.999 |
• Statistically significant difference
LAFH Lower anterior facial height*ANS Anterior nasal spine
Fig 4.
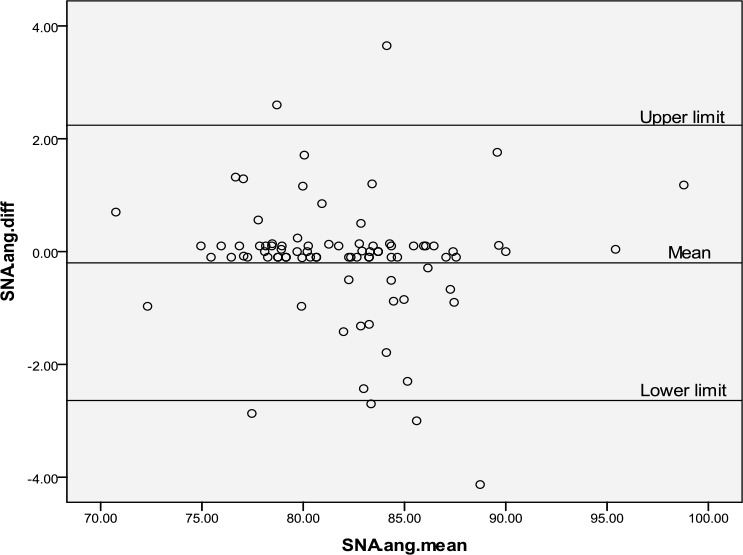
Bland-Altman analysis graph for SNA angle
DISCUSSION
In this study, a total of 150 lateral cephalograms of patients with normal occlusion and skeletal relationship were selected from the archives [7, 8]. The sample size was calculated by a statistician. Cephalograms were all scanned with the same scanner to eliminate any possible error. Tracing and analysis of cephalograms were performed by a dentist and re-evaluated by an orthodontist; this significantly diminished landmark identification errors. In the present study, McNamara cephalometric analysis norms were used to design a software program for cephalometric analysis of Fars subjects. The cephalograms were taken in NHP, which is essential for cephalometric analysis because an extra-cranial reference line is used instead of an intracranial reference line. Patients have considerable biological variations in inclination. Moreover, the McNamara analysis is based on NHP. For this reason, lateral cephalograms of subjects residing in Qazvin and Mashhad were obtained and the results of cephalometric analysis of the new software were compared with those of Dolphin software. This comparison demonstrated that our designed software had a very high correlation with Dolphin software in McNamara cephalometric analysis and this correlation was observed in both groups of Qazvin (ICC 0.570 to 1) and Mashhad residents (ICC 0.815 to 1).
Landmark identification for point A was much more sophisticated than for other landmarks. The lower ICC for U1-A demonstrated this fact and higher reliability was found for Mashhad residents because their cephalograms were obtained by the digital imaging system while cephalograms of Qazvin residents were taken by the conventional imaging systems. Therefore, it seems that our designed software has sufficient accuracy and reliability for diagnosis, treatment planning and assessment of the outcome of orthodontic treatments for both digital and conventional radiographic systems (cephalograms). Application of McNamara cephalometric analysis has several advantages. This analysis is mainly based on linear calculations; this is especially beneficial for treatment planning for orthognathic surgery. McNamara analysis has higher sensitivity for vertical changes compared to the analyses based on ANB angle [9,10] and therefore can be successfully applied during growth periods. Furthermore, McNamara analysis is based on NHP and thus, patient position error is eliminated leading to higher reliability [3,4].
Previous studies have demonstrated the accuracy of cephalometric analysis with Dolphin software compared to the manual technique [11–13]. Ozsoy et al. studied 30 lateral cephalograms and compared the accuracy of Vistadent O.C1.1 software measurements with that of manual measurements. Assessment was performed in two phases of pre- and post-treatment. Statistically, significant differences were found in SNB, Cd-A, Cd-Gn, L1-NB and U1-NA after treatment in both manual and software calculations. No significant difference was found between the two techniques confirming our results [13]. Power et al. evaluated and compared the reliability and reproducibility of cephalometric digitization with Dolphin Imaging Software and the conventional manual technique. They evaluated 60 lateral cephalograms and analyzed the obtained data using Lin's Correlation of Concordance. They showed that each technique had 95% reliability. Comparison of standard deviations of differences revealed that manual tracing was more reliable for SNA, SNB, and maxilla/mandible difference; whereas, digital tracing with Dolphin software had higher reliability for U1-A point and L1-A point. However, Dolphin software calculated the “lower anterior facial height” 4% higher than the manual technique, which was clinically significant [14]. Many studies have compared available cephalometric analysis software programs and found no clinically significant difference between the measured values [15–17]. Magro Filho et al. compared 2 software programs for prediction of profile changes in Class III patients undergoing orthognathic surgery. Dolphin imaging software was able to more accurately predict the nasal tip, chin, and submandibular areas; while, Dentofacial Planner Plus was superior in predicting nasolabial angle, upper lip and lower lip. The two software programs had no clinically significant difference in total profile comparison [15]. Gregeston et al. compared the results of cephalometric analysis with the conventional manual technique and three software programs of Dolphin, Vistadent 8 and Vistadent 7.33. Digital images were superior in eliminating the film processing steps and software programs were not as efficient as the manual technique in predicting incisal apices, Gnathion and Gonion. However, no clinically significant differences were found in inter- and intra-class comparisons [16]. Aside from the growth and development, some other factors are involved in changes of cephalometric indices. Cephalometric measurements and calculations can be affected by errors and factors such as the quality of the radiograph, clinician’s interpretation of the graph and method of prediction of indices and landmarks [18]. Our designed software program has several advantages; it saves time by performing analysis and measurements faster than the manual technique and allows for the adjustment of magnification, density, contrast and image quality for easier landmark identification [19–21]. Ravindranath et al. compared the reliability of Dolphin Imaging 10 and Vistadent OC in predicting the soft tissue changes of the mandible. The differences in soft tissue cephalometric parameters between the two software programs were found to be minimal except for the lower lip parameters [22]. Akhoundi et al. evaluated the accuracy and reliability of Dolphin Imaging Software for prediction of soft tissue changes and demonstrated that the nasal tip had the highest reliability while the sub-nasal and upper lip showed the least accuracy [23].
The current study confirmed the accuracy and reliability of our designed software in comparison with Dolphin software. This software is less expensive than similar software programs available in the market and therefore, can greatly reduce the related expenses for orthodontists practicing in Iran.
CONCLUSION
The cephalometric analysis of the newly designed software had a high correlation with Dolphin Imaging Software, signifying the high accuracy and reliability of our software (ICC=1). The advantages of our designed cephalometric analysis software include faster analysis and adjustment of magnification, density, contrast, and image quality in comparison with the manual technique, as well as lower cost in comparison with Dolphin software, facilitating diagnosis, treatment planning, and prediction of treatment outcome. This new software can be considered as a substitute for Dolphin software, which is not easily accessible in developing countries mainly due to financial restrictions.
ACKNOWLEDGMENTS
This paper was part of a thesis for DDS degree by Dr. SH. Hamidiaval under the supervision of Dr. M. Nouri and was financially supported by the Dental Research Institute of Shahid Beheshti University of Medical Sciences, Tehran, Iran (Grant NO.3566).
REFERENCES
- 1-.Bansal N, Singla J, Gera G, Gupta M, Kaur G.Reliability of natural head position in orthodontic diagnosis: A cephalometric study. Contemp Clin Dent. 2012April; 3( 2): 180– 3. doi: 10.4103/0976-237X.96824 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2-.Lundström A, Lundström F, Lebret LM, Moorrees CF.Natural head position and natural head orientation: basic considerations in cephalometric analysis and research. Eur J Orthod. 1995April; 17( 2): 111– 20. [DOI] [PubMed] [Google Scholar]
- 3-.Proffit WR, Sarver MD, Ackerman JL.Orthodontic diagnosis: The Problem-Oriented Approach. In: Proffit WR, Fields Henry W., JrContemporary orthodontics. 5th ed.Canada: Elsevier Mosby; 2013. p. 156– 203. [Google Scholar]
- 4-.McNamara JA., Jr.A method of cephalometric evaluation. Am J Orthod. 1984December; 86( 6): 449– 69. [DOI] [PubMed] [Google Scholar]
- 5-.Jacobson A.McNamara analysis. In: Jacobson A, Jacobson R.L.Radiographic cephalometry from basic to video imaging. Chicago: Quintessence book; 2006. p. 113– 23. [Google Scholar]
- 6-.Ahangaratashi MH, Bardal R.A template based on concepts of natural head position for Tabriz's adults. J Dent Sch 2007; 25: 119– 26. [Google Scholar]
- 7-.Nouri M, AdeliNajafi M, Azimi S.Longitudinal comparison of cephalometric norms in children after 2 years using DentoPlanner Plus software. J Dent Sch 2008; 26: 85– 94. [Google Scholar]
- 8-.Basafa M, Shahri F.Cephalometric analysis of Mashhad children based on “natural head position”. J Mash Dent Sch 2007; 31: 4– 8. [Google Scholar]
- 9-.Steiner CC.Cephalometrics for you and me. Am J Orthod 1953; 39: 729– 55. [Google Scholar]
- 10-.Steiner CC.Cephalometrics in clinical practice. Angle Orthod 1959; 29: 8– 29. [Google Scholar]
- 11-.Nouri M, Akbarzadeh A, Hamidi Aval Sh, Hemmati Sh.Assessment of errors in cephalometric measurements: Comparison of manual technique with software program. J Dent Sch 2011; 29: 76– 83 [Google Scholar]
- 12-.Uysel T, Baysal A, Yagsi A.Evaluation of speed, repeatability and reproducibility of digital radiography with manual versus computer-assisted cephalometric analyses. Eur J Orthod. 2009October; 31( 5): 523– 8. doi: 10.1093/ejo/cjp022 . Epub 2009 May 14. [DOI] [PubMed] [Google Scholar]
- 13-.Polat-Ozsoy O, Gokcelik A, ToygarMemikoglu TU.Differences in cephalometric measurements: a comparison of digital versus hand-tracing methods. Eur J Orthod. 2009June; 31( 3): 254– 9. doi: 10.1093/ejo/cjn121 . Epub 2009 Apr 6. [DOI] [PubMed] [Google Scholar]
- 14-.Power G, Breckon J, Sherriff M, McDonald F.Dolphin imaging software: an analysis of the accuracy of cephalometric digitization and orthognathic prediction. Int J Oral Maxillofac Surg. 2005September; 34( 6): 619– 26. [DOI] [PubMed] [Google Scholar]
- 15-.Magro-Filho O, Magro-Emica N, Queiroz TP, Aranega AM, Garcia IR., Jr.Comparative study of 2 software programs for predicting profile changes in class 111 patients having double-jaw orthognathic surgery. Am J Orthod Dentofacial Orthop. 2010April; 137( 4): 452.e1– 5; discussion 452–3. doi: 10.1016/j.ajodo.2009.02.027 . [DOI] [PubMed] [Google Scholar]
- 16-.Gregston M. D, Kula Th, Hardman P, Alan G, Kula K.A comparison of conventional and digital radiographic methods and cephalometric analysis software: I. Hard tissue. Seminars in Orthodontics 2004; 10: 204– 211. [Google Scholar]
- 17-.Baskin H, Cisneros GJ.A comparison of two computer cephalometric programs. J Clin Orthod. 1997April; 31( 4): 231– 3. [PubMed] [Google Scholar]
- 18-.Thilander B, Persson M, Adolfsson U.Roentgen-cephalometric standards for a Swedish population. A longitudinal study between the ages of 5 and 31 years. Eur J Orthod. 2005August; 27( 4): 370– 89. [DOI] [PubMed] [Google Scholar]
- 19-.Bruntz LQ, Paolmo JM, Baden S, Hans MG.A comparison of scanned lateral cephalogram with corresponding original radiographs. Am J Orthod Dentofacial Orthop. 2006September; 130( 3): 340– 8. [DOI] [PubMed] [Google Scholar]
- 20-.Dvortsin DP, Sandham A, Pruim GJ, Dijkstra PU.A comparison of the reproducibility of manual tracing on screen digitization for cephalpmetric profile variables. Eur J Orthod. 2008December; 30( 6): 586– 91. doi: 10.1093/ejo/cjn041 . Epub 2008 Aug 21. [DOI] [PubMed] [Google Scholar]
- 21-.Silveira HL, Silveira HE, Dalla-Bona RR, Abdala DD, Bertoldi RF, von Wangenheim A.Software system for calibrating examiners in cephalometric point identification. Am J Orthod Dentofacial Orthop. 2009March; 135( 3): 400– 5. [DOI] [PubMed] [Google Scholar]
- 22-.Ravindranath S, Krishnaswamy NR, Sandaram G.Comparison of two imaging programs in predicting the soft tissue changes with Mandibular advancement surgery. Orthodontics (Chic.). 2011Winter; 12( 4): 354– 65. [PubMed] [Google Scholar]
- 23-.Ahmad Akhoundi MS, Shirani G, Arshad M, Heidar H, Sodagar A.Comparison of an imaging software and manual prediction of soft tissue changes after orthognathic surgery. J Dent (Tehran). 2012Summer; 9( 3): 178– 87. Epub 2012 Sep 30. [PMC free article] [PubMed] [Google Scholar]