

Abstract
Background:
Rotational injuries are the most common and usually classified as per the Lauge Hansen classification; with the most common subgroup being the supination external rotation (SER) mechanism. Isolated fractures of the distal fibula (SE2) without associated ligamentous injury are usually treated with a splint or brace and the patient may be allowed to weight bear as tolerated. This study reports the functional outcomes following a stable, low energy, rotational ankle fracture supination external rotation (SER2) when compared to unstable SER4 fractures treated operatively.
Materials and Methods:
64 patients who were diagnosed and treated nonoperatively for a stable SER2 ankle fracture were followed prospectively. In the comparison group, 93 operatively treated fibular fractures were extracted from a prospectively collected database and evaluated comparison. Baseline characteristics obtained by trained interviewers at the time of injury included: Patient demographics, short form-36, short musculoskeletal functional assessment (SMFA) and American Orthopedic Foot and Ankle Society (AOFAS) questionnaires. Patients were followed at 3, 6 and 12 months postsurgery. Additional information obtained at each followup point included any complications or evidence on fracture healing. Data were analyzed by the Student's t-test and theFisher's Exact Test to compare demographic and functional outcomes between the two cohorts. P < 0.05 was considered to be significant.
Results:
The average of patients’ age in the stable fracture cohort was 43 versus 45 in the SER4 group. Nearly 64% of the patient population was female when compared with 37% in the operative group. In the SER2 by 6 months all patients had returned to baseline functional status. There were 18 delayed unions (all healed by 6 months). Based on the functional outcome scores all patients had returned to preoperative level. In comparison, SE4 patients had less functional recovery at 3 and 6 months (P < 0.05) based on the SMFA scores and at 3, 6 and 12 months based on the AOFAS (P < 0.001) scores. There was no difference in pain levels between the two groups at all time points. There were three nonunions in the SE4 group and six delayed unions.
Conclusions:
An SER2 ankle fracture is a relatively benign injury with functional limitations resolving by 3 months while the need for surgical fixation in SER ankle fractures appears to affect lower extremity function to a greater degree for a longer time period. Patients should be counseled as to these expected outcomes.
Keywords: Fibular fractures, supination external rotation injuries, ankle fractures
Keywords: Ankle injuries, fractures, fibula
INTRODUCTION
Ankle fractures can range from nondisplaced, avulsion fractures to complex fracture dislocations requiring urgent reduction with the need for surgical stabilization.1 Rotational injuries are the most common and usually classified as per the Lauge Hansen classification; with the most common subgroup being the supination external rotation (SER) mechanism.2 Isolated fractures of the distal fibula (SE2) without associated ligamentous injury are usually treated with a splint or brace and the patient may be allowed to weight bear as tolerated. Most of these patients have an excellent outcome and are able to return to their preinjury level of function without significant disability.3 The presence of an intact deltoid ligament confers stability to the ankle such that nonsurgical treatment and weight bearing is feasible and allows fracture healing.4
The purpose of this study was two-fold: (1) Report on clinical and functional outcomes following a stable, low energy rotational ankle fracture (SE2, SE3) and (2) to compare these outcomes to that of a cohort of patients who sustained an unstable SER fracture (OTA 44B2.1/B3.1) treated operatively (SE4).
MATERIALS AND METHODS
Following IRB approval, all patients who sustained an isolated fibular fracture between January 2009 and 2010 and presented for treatment to one of the two senior authors were identified. Standard protocol was to determine the medial clear space widening on initial radiographs or manual stress radiograph [Figure 1]. These patients were classified into four SER types. Those with a “proven stable” (based on stress radiographs for those with medial tenderness or ecchymosis) ankle mortise were classified as either SE2 [Figure 2] or SE3 and treated functionally. 64 patients who presented with an isolated fibular fracture and a stable ankle mortise (SE2) were enrolled. Those patients with delayed evidence of deltoid ligament injury were excluded from this group. Other exclusion criteria included open fractures; skeletally immature patients and those unable or unwilling to consent.
Figure 1.

X-ray of ankle joint anteroposterior view showing example of supination external rotation (SE4) injuries with fibular fracture and medial space widening indicating a deltoid ligament disruption and unstable injury
Figure 2.

X-ray of ankle joint anteroposterior view showing example of a SE2 injury with fibular fracture and intact ankle mortise with no medial widening and stable injury
The standard protocol for the nonoperative treatment of this injury pattern consisted of weight bearing as tolerated with passive/active ankle motion exercises. Patients were placed in a fracture brace (air stirrup, CAM boot) and allowed to perform activities as tolerated.
Baseline characteristics obtained by trained interviewers at the time of injury included: Patient demographics and the short form-36, the short musculoskeletal functional assessment (SMFA) and the American Orthopedic Foot and Ankle Society (AOFAS) ankle-hindfoot questionnaires.
Patients were followed at 3, 6 and 12 months postinjury. Clinical examination for fracture site tenderness and ankle range of motion was performed by the treating physician. The time to fracture healing and return to work were documented.
A control group of 93 previous, operatively treated fibular fractures were extracted from a prospectively collected database and evaluated for comparison. These patients too presented to one of the senior authors with an isolated fibular fracture, with an associated medial ligamentous injury, diagnosed on either the injury film or stress views as unstable ankle fractures (SE4 group). All were treated operatively with small fragment plates and screws. Baseline and followup data were collected in a similar manner to the nonoperative group. Patients underwent external rotation stress radiographs which showed medial widening of 5 mm or more indicating instability and underwent surgery. During surgery, the fibular fracture was fixed with a lateral or posterolateral plate; once this was done, the ankle was stressed again under fluoroscopy to confirm intact and stable ankle mortise. If the medial side or the symdesmosis appeared wide, a bone reduction clamp was used for reduction and a syndesmosis screw was inserted. If the medial side was persistently wide, a medial incision was taken to explore the medial side and any in folded deltoid ligament was removed and the ankle was then reduced.
Standard statistical analysis was performed. Data were analyzed by the Student's t-test and the Fisher's Exact Test to compare demographic and functional outcomes between the two cohorts. A P < 0.05 was considered to be significant.
RESULTS
64 patients enrolled in the study, the average followup at 6 months was completed by 80% of the patients while at 1 year, 70% completed the followup questionnaire respectively. The average age in the SE2/3 cohort was 43 years (range 18-81 years). 64% of the patient population was female. 9% of fractures were work related.
At 3 months, (90%) of the SE2 patients had returned to work either full time or with some restrictions which included limited ambulation or carrying heavy loads. At 3 months, 6 months and 12 months, the cohort with restricted work limitations was reported as 23%, 22% and 8% respectively. By 6 months, all patients had returned to baseline functional status. Based on the functional outcome scores (SMFA and AOFAS) all patients had returned to preoperative level at the 6 month followup.
Radiographic followup revealed eighteen patients who were not completely healed at 12 weeks (30% delayed union); however by 6 months all fractures had united.
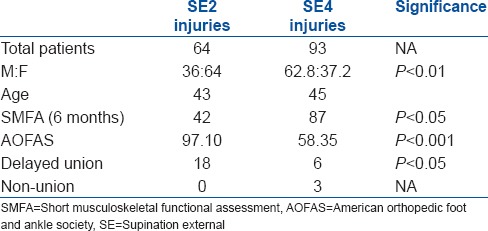
When comparing the SE2 patients to the SE4, there were a greater percentage of female patients in the nonoperative group (64%) than in the operative group (37.2%) (P < 0.01). There were no other differences between the two groups with regard to socio-demographic factors. The SE4 patients had diminished functional recovery at 3 and 6 months (P < 0.05) based on SMFA scores (emotional and mobility sub-groups) and at all followups based on the AOFAS (P < 0.001) scores. Interestingly, there was no difference in pain levels between the two groups at all time points.
Radiographically, there were six delayed unions and three symptomatic nonunions in the SE4 group which required revision of fixation and bone grafting. There were two superficial infections noted that resolved with antibiotic treatment alone without surgical intervention [Table 1].
Table 1.
Comparing the demographics and results (at 6 months followup)
DISCUSSION
Isolated fibular fractures are considered as stable ankle injuries which can be treated successfully with nonoperative treatment, utilizing early weight bearing and return to function. It is important to differentiate these stable injuries from those with a medial ligamentous or syndesmosis injury. The difference between an SE2/3 and SE4 injury is the presence of additional injuries leading to ankle instability; with the medial injury being either a deltoid ligament rupture or a medial malleolus fracture. We compared two groups of fibular fractures, those who had isolated fibular fractures (SE2/3 group) and those with a fibular fracture and a medial deltoid injury (SE4 group).
While biomechanical studies have shown alteration in the tibiotalar contact pressures with displaced fibular fractures;5 most of the authors agree that isolated fibular fractures can be treated nonsurgically. Yde and Kristensen in a comparative study of operative and nonoperative care for these fractures, demonstrated equivalent outcomes at followups ranging from 3 to 10 years.6 The presence of other injuries may lead to instability as confirmed on stress views and most likely necessitate operative stabilization. We did not perform surgical repair on any isolated fibular fracture; and only those injuries that were confirmed to be unstable on stress views and/or had medial injury underwent surgery and were included in the SE4 group.
Stufkens et al. in a review of literature compared the outcomes of distal fibular fractures treated nonoperatively (SE2) with those treated operatively (SE4). Of the 442 fractures where this comparison was carried out, SE2 fractures had a 92.2% good excellent outcome, while only 81.7% of patients had the same outcome in the SE4 group. Since, they were able to associate poorer outcome to the presence of medial injury, they recommend using this differentiation for reporting function following these injuries.7 This finding is confirmed in the current comparative study, where the SE2 injury group had an uneventful recovery and return to function within the first 6 months; while the SE4 group continued to have symptoms even at 1 year followup. SE4 patients also had significantly worse scores on the SMFA at 6 months and on the AOFAS scores at all-time points when compared to SE2 patients.
In our study of nonoperatively treated fibular fractures, we did have a significant number of patients with delayed union, all of whom healed eventually. Development of nonunion following stable SE2/3 injuries have been reported by various authors.8,9 Walsh and DiGiovanni9 reported treating six fibular nonunions for pain and antalgic gait and concluded that distal fibula nonunion appears to be a relatively common cause of persistent lateral ankle symptoms in patients who do not enjoy a satisfactory recovery after appropriate conservative treatment. The authors believe that the persistent lateral pain in such patients results from micro motion strain at the un-united fracture site.9 In our series of SE2/3 fractures, there were 18 delayed unions (30%) but all proceeded to unite by 6 months without any surgical intervention. In contrast, the SE4 group had six delayed unions (7%) and three nonunions (3%), the latter requiring revision of fixation with bone grafting. Long term outcome of these injuries have been reported as being satisfactory and it is possible that over time differences between our patient groups will even out.10
The limitations of our study include the use of a separate control group that may not represent a true comparison to the injury pattern studied. Our purpose was to provide a comparison to a similar injury pattern (isolated fibula, however with ligamentous disruption) treated by the same authors at the same institution. The diagnosis of stable or unstable injury pattern and the resultant treatment was based on X-rays and not magnetic resonance imaging scans which may have helped delineate more ligamentous injuries. Our numbers were low with followup at 1 year of only 70% with SE2 injuries; however, as most of these patients appeared to be doing well by 6 months and further followup was difficult in getting the patients to return for evaluation.
The SE2/3 fracture pattern is a relatively benign injury pattern with complete return of function and resolution of symptoms by 6 months; while patients with associated medial injury (SE4 pattern) have sustained a more significant injury and function at a lower capacity at 1 year. Patients who sustain an SE2 ankle fracture should be counseled that their fracture may take between 3 and 6 months to heal and return to preinjury levels of function.
Footnotes
Source of Support: Nil
Conflict of Interest: None.
REFERENCES
- 1.Baron JA, Karagas M, Barrett J, Kniffin W, Malenka D, Mayor M, et al. Basic epidemiology of fractures of the upper and lower limb among Americans over 65 years of age. Epidemiology. 1996;7:612–8. doi: 10.1097/00001648-199611000-00008. [DOI] [PubMed] [Google Scholar]
- 2.Lauge-Hansen N. Fractures of the ankle. II. Combined experimental-surgical and experimental-roentgenologic investigations. Arch Surg. 1950;60:957–85. [PubMed] [Google Scholar]
- 3.Pakarinen HJ, Flinkkil TE, Ohtonen PP, Ristiniemi JY. Stability criteria for nonoperative ankle fracture management. Foot Ankle Int. 2011;32:141–7. doi: 10.3113/FAI.2011.0141. [DOI] [PubMed] [Google Scholar]
- 4.Michelsen JD, Ahn UM, Helgemo SL. Motion of the ankle in a simulated supination-external rotation fracture model. J Bone Joint Surg Am. 1996;78:1024–31. doi: 10.2106/00004623-199607000-00006. [DOI] [PubMed] [Google Scholar]
- 5.Harris J, Fallat L. Effects of isolated Weber B fibular fractures on the tibiotalar contact area. J Foot Ankle Surg. 2004;43:3–9. doi: 10.1053/j.jfas.2003.11.008. [DOI] [PubMed] [Google Scholar]
- 6.Yde J, Kristensen KD. Ankle fractures: Supination-eversion fractures of stage IV. Primary and late results of operative and nonoperative treatment. Acta Orthop Scand. 1980;51:981–90. doi: 10.3109/17453678008990904. [DOI] [PubMed] [Google Scholar]
- 7.Stufkens SA, van den Bekerom MP, Kerkhoffs GM, Hintermann B, van Dijk CN. Long term outcome after 1822 operatively treated ankle fractures: A systematic review of the literature. Injury. 2011;42:119–27. doi: 10.1016/j.injury.2010.04.006. [DOI] [PubMed] [Google Scholar]
- 8.McGonagle L, Ralte P, Kershaw S. Nonunion of Weber B distal fibula fractures: A case series. Foot Ankle Surg. 2010;16:e63–7. doi: 10.1016/j.fas.2010.03.008. [DOI] [PubMed] [Google Scholar]
- 9.Walsh EF, DiGiovanni C. Fibular nonunion after closed rotational ankle fracture. Foot Ankle Int. 2004;25:488–95. doi: 10.1177/107110070402500708. [DOI] [PubMed] [Google Scholar]
- 10.Donken CC, Verhofstad MH, Edwards MJ, van Laarhoven CJ. Twenty-one-year followup of supination-external rotation type II-IV (OTA type B) ankle fractures: A retrospective cohort study. J Orthop Trauma. 2012;26:e108–14. doi: 10.1097/BOT.0b013e31822c4ea5. [DOI] [PubMed] [Google Scholar]