

Abstract
Perforation is one of the most serious complications of endoscopic sphincterotomy (ES) necessitating immediate surgical intervention. We present a case of successful management of such a complication with endoclipping. A 85-year-old woman developed duodenal perforation after ES. The perforation was identified early and its closure was achieved using three metallic clips in a single session. There was no procedure-related morbidity or complications and our patient was discharged from hospital 10 d later. Endoclipping of duodenal perforation induced by ES is a safe, effective and alternative to surgery treatment.
Keywords: Endoclipping, Duodenal perforation, Endoscopic sphincterotomy
INTRODUCTION
The most serious complications of endoscopic sphincterotomy (ES) are pancreatitis, hemorrhage and perforation[1]. Although perforation is uncommon, occurring in less than 1% of patients undergoing ES, it is associated with high morbidity and mortality[2].
Applications of endoscopic metallic clips other than the treatment of bleeding lesions have been reported, such as sealing of iatrogenic endoscopic perforations[3].
We describe a 85-year-old woman who developed symptomatic post-ES perforation and was successfully treated by endoscopic clip placement. To our knowledge, this is the second reported case of post-ES perforation that was treated endoscopically with clip placement.
CASE REPORT
A 85-year-old woman was admitted because of recurrent episodes of abdominal pain, fever, and jaundice over a period of 1 mo. Her past medical history revealed a cholecystectomy 10 years ago, mild heart failure and hypertension. Laboratory tests showed cholestasis. US demonstrated intra- and extra-hepatic biliary dilatation. Magnetic resonance imaging cholangiography showed a large stone (diameter 18 mm) in the lower part of the common bile duct.
Endoscopic biliary sphincterotomy was performed using an electrosurgical unit with standard pull sphincterotome without the use of guidewire. The length of sphincterotomy was large, according to the size of the common bile duct stone. The extraction of the stone was impossible. We performed a successful mechanical lithotripsy and the fragments were extracted with a basket.
Twelve hours later, the patient complained of moderate pain in the upper abdomen, which diminished after analgesics administration. Physical examination disclosed fever of 37.8 °C but no signs of peritoneal irritation. A chest X-ray was normal. Laboratory studies revealed an elevated ESR (75 mm/h) and C-reactive protein concentration (3.62 mg/dL, normal <0.5 mg/dL). The WBC count was 11 888/mL (normal 4 000-8 000/mL) and the percentage of neutrophils was high (86%).
An abdominal CT demonstrated free retroperitoneal air and a small amount of dirty fluid around the duodenum as well as enhancement of choledochal duct with gastrografin (Figure 1).
Figure 1.
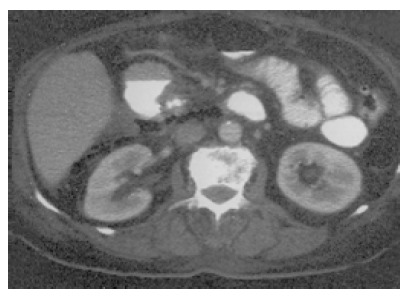
Free retroperitoneal air and a small amount of dirty fluid around the duodenum.
We decided to try endoscopic repair of the duodenal perforation, after an extensive discussion about the type of therapy with her relatives, and an informed consent was signed. With a rotating colon clipping device (HX-6UR-1, Olympus), five clips were carefully placed in the upper part of sphincterotomy. Although two were misclipped, the other three were well fitted (Figure 2). A standard 0.035-inch biliary super-stiff guidewire (Jagwire, Microvasive) was then passed endoscopically and fluoroscopically into the jejunum and a nasogastric tube with the tip removed was passed into the duodenum and centered over the perforation site.
Figure 2.
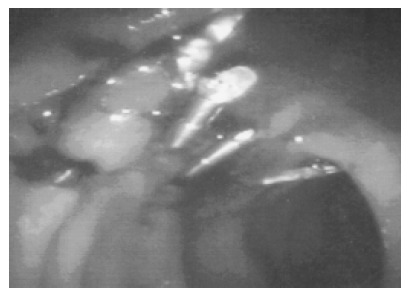
Three clips placed on the upper part of sphincterotomy.
Intravenous hyperalimentation and treatment with antibiotics (ciprofloxacin 1 g/d and metronidazole 1.5 g/d) were administered. Clinically, the patient did well and the abdominal pain that was initially present decreased, no signs of peritonitis developed and the fever subsided. Three days later, a water-soluble contrast was instilled via the nasogastric tube and on radiography no leakage of contrast was found. She began to eat 7 d after the clipping procedure and was discharged on d 10. A second abdominal CT performed 20 d later demonstrated resolution of the retroperitoneal air and inflammation.
No further problems occurred after 5 mo of follow-up.
DISCUSSION
The approach to management of duodenal perforation after ES is controversial. Some investigators advocate conservative management based on clinical course, while others advocate surgical repair in all cases because of the complications associated with delayed operative intervention[4-6].
Dunham et al[4] have reported about the outcome after conservative treatment in seven patients when free air was recognized immediately. Two of these patients died after the development of toxic shock despite delayed surgery. In a recent prospective study by Freemanet al[1] five of the eight ES perforations were severe and one resulted in death.
In recent years, endoscopic clip placement, developed as a hemostatic procedure, has been used for closure of iatrogenic perforations[3]. Binmoeller et al[7] described the first successful endoscopic closure of an iatrogenic perforation by using a clip-application device in 1993. Subsequently, the use of this method in the esophagus[8,9], duodenum[10], and colon[11,12] has been described. Baron et al[13] described the first case of a 39-year-old man with familial adenomatous polyposis who presented duodenal perforation after a papillectomy and ES. They identified immediately free air in the retroperitoneum and the perforation was closed by the use of a clipping device and the placement of five clips.
The decision about the treatment after an iatrogenic perforation must be made very carefully, because conservative treatment may surely be used when perforation is small and retroperitoneal, non-operative management failed but with delayed laparotomy results in greater contamination necessitating major surgery. In our patient, the perforation was small, well defined, and detected without delay, thus meeting all the criteria for a conservative approach. Therefore, we decided to try to close the perforation immediately with metallic clips. After successful endoscopic clipping, our patient recovered quickly without any complication and was discharged early from hospital. The immediate closure of the perforation prevented any further abdominal contamination and contributed to the good outcome of the patient. Although this complication could be resolved with the conservative management strategy of nasogastric suction and antibiotics, we believe that our patient with the size of the duodenal wall defect may require prolonged hospitalization and/or surgical management.
It must be emphasized that the endoclipping device has been designed for use through the end-viewing endoscope. Therefore, the deployment of clips is more difficult when a side-viewing endoscope is used and damage to the endoclipping device may occur. The deployment of the clips requires significant experience from the endoscopist when a duodenoscope is used, especially in a limited space as is the major papilla area. The placement of the clips should be made carefully on the upper part of the sphincterotomy to avoid closure of pancreatic or common bile duct orifice.
In cases of iatrogenic perforation, if the defect is closed early with metallic clips, contamination of the peritoneal cavity or retroperitoneal space can be minimized. Although the difference in outcome between conservative management and clipping is unknown, clipping therapy is more certain to prevent contamination.
In conclusion, when perforation is caused by ES, endoscopic closure using metallic clips without laparotomy might be the first choice of treatment, although it is essential to monitor the patient closely, with particular attention to signs of transition from localized to generalized peritonitis.
Footnotes
Science Editor Wang XL and Guo SY Language Editor Elsevier HK
References
- 1.Freeman ML, Nelson DB, Sherman S, Haber GB, Herman ME, Dorsher PJ, Moore JP, Fennerty MB, Ryan ME, Shaw MJ, et al. Complications of endoscopic biliary sphincterotomy. N Engl J Med. 1996;335:909–918. doi: 10.1056/NEJM199609263351301. [DOI] [PubMed] [Google Scholar]
- 2.Cotton PB, Lehman G, Vennes J, Geenen JE, Russell RC, Meyers WC, Liguory C, Nickl N. Endoscopic sphincterotomy complications and their management: a attempt at consensus. Gastrointest Endosc. 1991;37:383–393. doi: 10.1016/s0016-5107(91)70740-2. [DOI] [PubMed] [Google Scholar]
- 3.Raju GS, Gajula L. Endoclips for GI endoscopy. Gastrointest Endosc. 2004;59:267–279. doi: 10.1016/s0016-5107(03)02110-2. [DOI] [PubMed] [Google Scholar]
- 4.Dunham F, Bourgeois N, Gelin M, Jeanmart J, Toussaint J, Cremer M. Retroperitoneal perforations following endoscopic sphincterotomy; clinical course and management. Endoscopy. 1982;14:92–96. doi: 10.1055/s-2007-1021589. [DOI] [PubMed] [Google Scholar]
- 5.Chung RS, Sivak MV, Ferguson DR. Surgical decisions in the management of duodenal perforation complicating endoscopic sphincterotomy. Am J Surg. 1993;165:700–703. doi: 10.1016/s0002-9610(05)80791-3. [DOI] [PubMed] [Google Scholar]
- 6.Chaudhary A, Aranya RC. Surgery in perforation after endoscopic sphincterotomy: sooner, later or not at all? Ann R Coll Surg Engl. 1996;78:206–208. [PMC free article] [PubMed] [Google Scholar]
- 7.Binmoeller KF, Grimm H, Soehendra N. Endoscopic closure of a perforation using metallic clips after snare excision of a gastric leiomyoma. Gastrointest Endosc. 1993;39:172–174. doi: 10.1016/s0016-5107(93)70060-7. [DOI] [PubMed] [Google Scholar]
- 8.Wewalka FW, Clodi PH, Haidinger D. Endoscopic clipping of esophageal perforation after pneumatic dilation for achalasia. Endoscopy. 1995;27:608–611. doi: 10.1055/s-2007-1005768. [DOI] [PubMed] [Google Scholar]
- 9.Cipolletta L, Bianco MA, Rotondano G, Marmo R, Piscopo R, Meucci C. Endoscopic clipping of perforation following pneumatic dilation of esophagojejunal anastomotic strictures. Endoscopy. 2000;32:720–722. doi: 10.1055/s-2000-7032. [DOI] [PubMed] [Google Scholar]
- 10.Rosés LL, Ramirez AG, Seco AL, Blanco ES, Alonso DI, Avila S, Lopez BU. Clip closure of a duodenal perforation secondary to a biliary stent. Gastrointest Endosc. 2000;51:487–489. doi: 10.1016/s0016-5107(00)70454-8. [DOI] [PubMed] [Google Scholar]
- 11.Mana F, De Vogelaere K, Urban D. Iatrogenic perforation of the colon during diagnostic colonoscopy: endoscopic treatment with clips. Gastrointest Endosc. 2001;54:258–259. doi: 10.1067/mge.2001.114959. [DOI] [PubMed] [Google Scholar]
- 12.Yoshikane H, Hidano H, Sakakibara A, Ayakawa T, Mori S, Kawashima H, Goto H, Niwa Y. Endoscopic repair by clipping of iatrogenic colonic perforation. Gastrointest Endosc. 1997;46:464–466. doi: 10.1016/s0016-5107(97)70045-2. [DOI] [PubMed] [Google Scholar]
- 13.Baron TH, Gostout CJ, Herman L. Hemoclip repair of a sphincterotomy-induced duodenal perforation. Gastrointest Endosc. 2000;52:566–568. [PubMed] [Google Scholar]